Systemic lupus erythematosus: Difference between revisions
| Line 264: | Line 264: | ||
*Complete physical examination | *Complete physical examination | ||
*Laboratory tests: | *Laboratory tests: | ||
:*Complete blood count (CBC) | :*[[Complete blood count]] ([[CBC]]) | ||
:*Erythrocyte sedimentation rate (ESR) | :*Erythrocyte sedimentation rate (ESR) | ||
:*Urinalysis | :*Urinalysis | ||
Revision as of 14:32, 24 March 2009
| Lupus Erythematosus | |
 | |
|---|---|
| Typical "butterfly"-like rash over the cheeks in lupus | |
| ICD-10 | L93, M32 |
| ICD-9 | 710.0 |
| OMIM | 152700 |
| DiseasesDB | 12782 |
| MedlinePlus | 000435 |
| eMedicine | med/2228 emerg/564 |
| MeSH | D008180 |

Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [3] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Click here for The heart in Systemic Lupus Erythematosus
Overview
Systemic Lupus Erythematosus (SLE or lupus) is a chronic autoimmune disease that can be fatal, though with recent medical advances fatalities are becoming increasingly rare. As with other autoimmune diseases, the immune system attacks the body’s cells and tissue, resulting in inflammation and tissue damage. [1]
SLE can affect any part of the body, but most often harms the heart, joints, skin, lungs, blood vessels, liver, kidneys and nervous system.[2]
The course of the disease is unpredictable, with periods of illness (called flares) alternating with remission. Lupus can occur at any age, and is most common in women, particularly of non-European descent.[3] Lupus is treatable symptomatically, mainly with corticosteroids and immunosuppressants, though there is currently no cure. However, many people with Lupus lead long and substantial lives.
Differential Diagnosis
- Acute disseminated encephalomyelitis
- Acute inflammatory demyelinating polyradiculoneuropathy
- Acute memory disorders
- Blood dyscrasias and stroke
- Brainstem gliomas
- Cardioembolic stroke
- Chorea in adults
- Chronic inflammatory demyelinating polyradiculoneuropathy
- Confusional states
- Dermatomyositis
- Diffuse sclerosis
- Endocrine myopathies
- HIV-1 associated CNS complications
- Intracranial hemorrhage
- Lambert-Eaton myasthenic syndrome
- Lyme disease
- Metabolic myopathies
- Myasthenia gravis
- Neurological sequelae of infectious endocarditis
- Polyarteritis nodosa
- Polymyositis
- Spinal cord infarction
- Sudden visual loss
- Temporal / Giant cell arteritis
- Vasculitic neuropathy
Etymology
There are several explanations ventured for the term lupus erythematosus. Lupus is Latin for wolf, and 'erythro' is derived from ερυθρόςTemplate:Polytonic, Greek for "red." All explanations originate with the reddish, butterfly-shaped malar rash that the disease classically exhibits across the nose and cheeks.
- In various accounts, some doctors thought the rash resembled the pattern of fur on a wolf's face.
- In other accounts doctors thought that the rash, which was often more severe in earlier centuries, created lesions that resembled wolf bites or scratches.
- Stranger still is the account that the term "Lupus" didn't come from Latin at all, but from the term for a French style of mask which women reportedly wore to conceal the rash on their faces. The mask is called a "loup", French for "Wolf"
- Another common explanation for the term is that the disease's course involves repeated attacks like those of a voracious predator, leaving behind the red blotches.
History
Medical historians have theorized people with porphyrias (a disease that shares many symptoms with Lupus) generated folklore stories of vampires and werewolves due to the photosensitivity, scarring, hair growth and porphyrin brownish-red stained teeth in severe recessive forms of porphyria or combinations of the disorders known as dual, homozygous or compound heterozygous porphyrias.
The history of lupus erythematosus can be divided into three periods: the classical, neoclassical, and modern. The classical period began when the disease was first recognized in the Middle Ages and saw the description of the dermatological manifestation of the disorder. The term lupus is attributed to the 12th century physician Rogerius, who used it to describe the classic malar rash. The neoclassical period was heralded by Móric Kaposi's recognition in 1872 of the systemic manifestations of the disease. The modern period began in 1948 with the discovery of the LE cell (the Lupus Erythematosus cell, a misnomer as it occurs with other diseases as well) and is characterised by advances in our knowledge of the pathophysiology and clinical-laboratory features of the disease, as well as advances in treatment.
Useful medication for the disease was first found in 1894, when quinine was first reported as an effective therapy. Four years later, the use of salicylates in conjunction with quinine was noted to be of still greater benefit. This was the best available treatment to patients until the middle of the twentieth century, when Hench discovered the efficacy of corticosteroids in the treatment of SLE.
Epidemiology
Previously believed to be a rare disease, Lupus has seen an increase in awareness and education since the 1960s. This has helped many more patients get an accurate diagnosis making it possible to estimate the number of people with lupus. In the United States alone, it is estimated that between 270,000 and 1.5 million people have lupus, making it more common than cystic fibrosis or cerebral palsy. The disease affects both females and males, though young women are diagnosed nine times more often than men. SLE occurs with much greater severity among African-American women, who suffer more severe symptoms as well as a higher mortality rate. [4] Worldwide, a conservative estimate states that over 5 million people have lupus.
Although SLE can occur in anyone at any age, it is most common in women of childbearing age. It affects 1 in 4000 people in the United States, with women becoming afflicted far more often than men. The disease appears to be more prevalent in women of African, Asian, Hispanic and Native American origin but this may be due to socioeconomic factors. People with relatives who suffer from SLE, rheumatoid arthritis or thrombotic thrombocytopenic purpura are at a slightly higher risk than the general population.[5]
Classification
Lupus is a chronic autoimmune disease in which the body's own defense system attacks otherwise healthy tissue. Clinically, it can affect multiple organ systems including the heart, skin, joints, kidneys and nervous system. There are several types of lupus; in general, when the word lupus alone is used, reference is to systemic lupus erythematosus, as discussed in this article. Other types include:[6] Other types include:
- Chronic cutaneous lupus erythematosus
- Discoid lupus erythematosus, a skin disorder that causes a red, raised rash on the face and scalp. Discoid lupus occasionally (1–5%) develops into SLE.[7]
- Localized discoid lupus erythematosus
- Generalized discoid lupus erythematosus
- Childhood discoid lupus erythematosus
- Chilblain lupus erythematosus (Hutchinson)
- Lupus erythematosus-lichen planus overlap syndrome
- Lupus erythematosus panniculitis (Lupus erythematosus profundus)
- Subacute cutaneous lupus erythematosus, which causes nonscarring skin lesions on patches of skin exposed to sunlight.[8]
- Tumid lupus erythematosus
- Verrucous lupus erythematosus (Hypertrophic lupus erythematosus)
- Discoid lupus erythematosus, a skin disorder that causes a red, raised rash on the face and scalp. Discoid lupus occasionally (1–5%) develops into SLE.[7]
- Neonatal lupus erythematosus, a rare disease affecting babies born to women with SLE, Sjögren's syndrome, or sometimes no autoimmune disorder. It is theorized that maternal antibodies attack the fetus, causing skin rash; liver problems; low blood counts, which gradually fade; and heart block, leading to bradycardia.[8]
- Childhood systemic lupus erythematosus, the pediatric variant of systemic lupus erythematosus.
- Drug-induced lupus erythematosus, a drug-induced form of SLE; this type of lupus can occur equally in either sex.
- Lupus nephritis, an inflammation of the kidneys caused by SLE.
- Complement deficiency syndromes
Causes
Despite the dramatic rise in Lupus research in recent years, the exact cause of the disease remains unknown. Indeed, consensus is still lacking on whether Lupus is a single condition or a group of related diseases. SLE is a chronic inflammatory disease believed to be a type III hypersensitivity response with potential type II involvement,[9] characterized by the body's production of antibodies against the nuclear components of its own cells. There are three mechanisms by which lupus is thought to develop: genetic predisposition, environmental triggers and drug reaction (drug-induced lupus).
Genetics
The first mechanism may arise genetically. Research indicates that SLE may have a genetic link. Lupus does run in families, but no single "lupus gene" has yet been identified. Instead, multiple genes appear to influence a person's chance of lupus developing when triggered by environmental factors. The most important genes are located on chromosome 6, where mutations may occur randomly (de novo) or be inherited. Additionally, people with SLE have an altered RUNX-1 binding site, which may be either cause or contributor (or both) to the condition. Altered binding sites for RUNX-1 have also been found in people with psoriasis and rheumatoid arthritis.
Environmental triggers
The second mechanism may be due to environmental factors. These factors may not only exacerbate existing lupus conditions, but also trigger the initial onset. They include certain medications (such as some antidepressants and antibiotics), extreme stress, exposure to sunlight, hormones, and infections. Some researchers have sought to find a connection between certain infectious agents (viruses and bacteria), but no pathogen can be consistently linked to the disease. UV radiation has been shown to trigger the photosensitive lupus rash, but some evidence also suggests that UV light is capable of altering the structure of the DNA, leading to the creation of autoantibodies. Some researchers have found that women with silicone gel-filled breast implants have produced antibodies to their own collagen, but it is not known how often these antibodies occur in the general population and there is no data that show these antibodies cause connective tissue diseases such as lupus.
Drug reactions
Drug-induced lupus erythematosus is a reversible condition that usually occurs in patients being treated for a long-term illness. Drug-induced lupus mimics systemic lupus. However, symptoms of drug-induced lupus generally disappear once a patient is taken off the medication which triggered the episode. There are about 400 medications currently in use that can cause this condition, though the most common drugs are procainamide, hydralazine and quinidine.
Non-SLE forms of lupus
Discoid (cutaneous) lupus is limited to skin symptoms and is diagnosed via biopsy of skin rash on the face, neck or scalp. Often an anti-nuclear antibody (ANA) test for discoid patients is negative or a low-titre positive. About 10% of discoid lupus patients eventually develop SLE.
Pathophysiology
Lupus is an example of pathophysiology, a disturbance of the normal functioning of the body. One manifestation of lupus is abnormalities in apoptosis, a type of programmed cell death in which aging or damaged cells are neatly disposed of as a part of normal growth or functioning.
Transmission
In SLE, the body's immune system produces antibodies against itself, particularly against proteins in the cell nucleus. SLE is triggered by environmental factors that are unknown.
"All the key components of the immune system are involved in the underlying mechanisms" of SLE, according to Rahman, and SLE is the prototypical autoimmune disease. The immune system must have a balance (homeostasis) between being sensitive enough to protect against infection, and being too sensitive and attacking the body's own proteins (autoimmunity). From an evolutionary perspective, according to Crow, the population must have enough genetic diversity to protect itself against a wide range of possible infection; some genetic combination's result in autoimmunity. The likely environmental triggers include ultraviolet light, drugs, and viruses. These stimuli cause the destruction of cells and expose their DNA, histones, and other proteins, particularly parts of the cell nucleus. Because of genetic variations in different components of the immune system, in some people the immune system attacks these nuclear-related proteins and produces antibodies against them. In the end, these antibody complexes damage blood vessels in critical areas of the body, such as the glomeruli of the kidney; these antibody attacks are the cause of SLE. Researchers are now identifying the individual genes, the proteins they produce, and their role in the immune system. Each protein is a link on the autoimmune chain, and researchers are trying to find drugs to break each of those links. [10][11][12]
SLE is a chronic inflammatory disease believed to be a type III hypersensitivity response with potential type II involvement.[13]
Abnormalities in apoptosis
- Apoptosis is increased in monocytes and keratinocytes
- Expression of Fas by B cells and T cells is increased
- There are correlations between the apoptotic rates of lymphocytes and disease activity
Tangible body macrophages (TBMs) are large phagocytic cells in the germinal centers of secondary lymph nodes. They express CD68 protein. These cells normally engulf B cells which have undergone apoptosis after somatic hypermutation. In some patients with SLE, significantly fewer TBMs can be found, and these cells rarely contain material from apoptotic B cells. Also, uningested apoptotic nuclei can be found outside of TBMs. This material may present a threat to the tolerization of B cells and T cells. Dendritic cells in the germinal center may endocytose such antigenic material and present it to T cells, activating them. Also, apoptotic chromatin and nuclei may attach to the surfaces of follicular dendritic cells and make this material available for activating other B cells which may have randomly acquired self-specificity through somatic hypermutation.[14]
Clearance deficiency

The exact mechanisms for the development of systemic lupus erythematosus (SLE) are still unclear since the pathogenesis is a multifactorial event. Beside discussed causations, impaired clearance of dying cells is a potential pathway for the development of this systemic autoimmune disease. This includes deficient phagocytic activity, scant serum components in addition to increased apoptosis.
Monocytes isolated from whole blood of SLE patients show reduced expression of CD44 surface molecules involved in the uptake of apoptotic cells. Most of the monocytes and tingible body macrophages (TBM), which are found in the germinal centres of lymph nodes, even show a definitely different morphology in patients with SLE. They are smaller or scarce and die earlier. Serum components like complement factors, CRP and some glycoproteins are furthermore decisively important for an efficiently operating phagocytosis. In patients these components are often missing, diminished or inefficient.
The clearance of early apoptotic cells is an important function in multicellular organisms. It leads to a progression of the apoptosis process and finally to secondary necrosis of the cells, if this ability is disturbed. Necrotic cells release nuclear fragments as potential autoantigens as well as internal danger signals, inducing maturation of dendritic cells (DC), since they have lost their membranes integrity. Increased appearance of apoptotic cells also is simulating inefficient clearance. That leads to maturation of DC and also to the presentation of intracellular antigens of late apoptotic or secondary necrotic cells, via MHC molecules.
Autoimmunity possibly results by the extended exposure to nuclear and intracellular autoantigens derived from late apoptotic and secondary necrotic cells. B and T cell tolerance for apoptotic cells is abrogated and the lymphocytes get activated by these autoantigens; inflammation and the production of autoantibodies by plasma cells is initiated. A clearance deficiency in the skin for apoptotic cells has also been observed in patients with cutaneous lupus erythematosus (CLE).
Accumulation in germinal centres (GC)

In healthy conditions apoptotic lymphocytes are removed in germinal centres by specialised phagocytes, the tingible body macrophages (TBM); that’s why no free apoptotic and potential autoantigenic material can bee seen.
In some patients with SLE accumulation of apoptotic debris can be observed in GC, because of an ineffective clearance of apoptotic cells.
In close proximity to TBM, follicular dendritic cells (FDC) are localized in GC, which attach antigen material to their surface and in contrast to bone marrow-derived DC, neither take it up nor present it via MHC molecules.
Autoreactive B cells can accidentally emerge during somatic hypermutation and migrate into the GC light zone. Autoreactive B cells, maturated coincidently, normally don’t receive survival signals by antigen planted on follicular dendritic cells and perish by apoptosis.
In the case of clearance deficiency apoptotic nuclear debris accumulates in the light zone of GC and gets attached to FDC. This serves as a germinal centre survival signal for autoreactive B-cells.
After migration into the mantle zone autoreactive B cells require further survival signals from autoreactive helper T cells, which promote the maturation of autoantibody producing plasma cells and B memory cells.
In the presence of autoreactive T cells a chronic autoimmune disease may be the consequence.
Anti-nRNP autoimmunity
Autoantibodies to nRNP A and nRNP C initially targeted restricted, proline-rich motifs. Antibody binding subsequently spread to other epitopes. The similarity and cross-reactivity between the initial targets of nRNP and Sm autoantibodies identifies a likely commonality in cause and a focal point for intermolecular epitope spreading.[15]
Others
Elevated expression of HMGB1 was found in the sera of patients and mice with systemic lupus erythematosus, High Mobility Group Box 1 (HMGB1) is a nuclear protein participating in chromatin architecture and transcriptional regulation. Recently, there is increasing evidence that HMGB1 contributes to the pathogenesis of chronic inflammatory and autoimmune diseases due to its pro-inflammatory and immunostimulatory properties.[16]
Signs and symptoms
SLE is one of several diseases known as the great imitator[17] because its symptoms vary so widely it often mimics or is mistaken for other illnesses, and because the symptoms come and go unpredictably. Diagnosis can be elusive, with patients sometimes suffering unexplained symptoms and untreated SLE for years. Common initial and chronic complaints are fever, malaise, joint pains, myalgias and fatigue. Because they are so often seen with other diseases, these signs and symptoms are not part of the diagnostic criteria for SLE. When occurring in conjunction with other signs and symptoms (below), however, they are considered suggestive.
Most Common Symptoms
Complete List of Signs and Symptoms
- Abdominal pain
- Discoid skin lesions
- Erythematous macules
- Fatigue
- Hemolytic anemia
- Interstitial lung disease
- Keratoconjunctivitis sicca
- Leukopenia
- Mucosal lesions
- Pericarditis
- Photo distributed rash
- Pleural effusion
- Pleuritic chest pain
- Pneumonitis
- Polyarthritis / polyarthralgia
- Raynaud phenomenon
- Renal disease
- Renal vasculitis
- Seizures
- Stroke
- Thrombocytopenia
- Weight loss
Common Symptoms Explained
- Dermatological manifestations
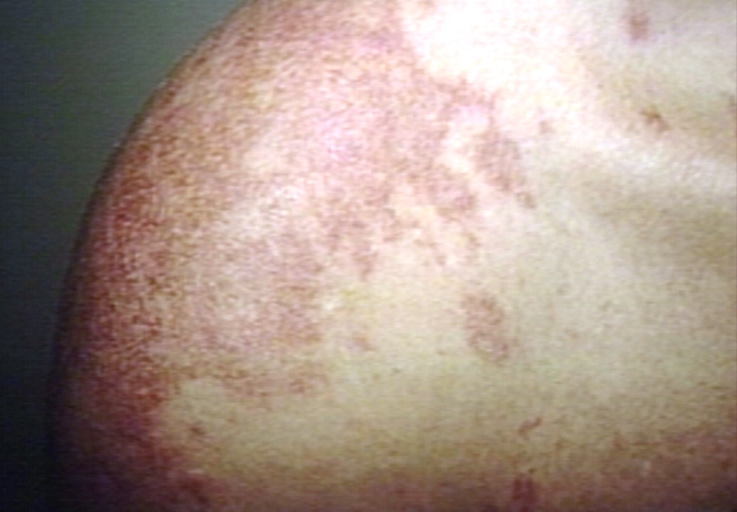
- As many as 30% of patients present with some dermatological symptoms (and 65% suffer such symptoms at some point), with 30% to 50% suffering from the classic malar rash (or butterfly rash) associated with the disease. Patients may present with discoid lupus (thick, red scaly patches on the skin). Alopecia, mouth, nasal, and vaginal ulcers, and lesions on the skin are also possible manifestations.
- Musculoskeletal manifestations
- Patients most often seek medical attention for joint pain, with small joints of the hand and wrist usually affected, although any joint is at risk. The Lupus Foundation of America "estimates that 95 percent of lupus cases involve achy joints [5] Unlike rheumatoid arthritis, SLE arthropathy is not usually destructive of bone, however, deformities caused by the disease may become irreversible in as many as 20% of patients.This small percentage may experience "damage to tendons or joint coverings in the hand" which leads to "deformity of the finger joint" [5]
- Hematological manifestations
- Anemia and iron deficiency may develop in as many as half of patients. Low platelet and white blood cell counts may be due to the disease or a side-effect of pharmacological treatment. Patients may have an association with antiphospholipid antibody syndrome (a thrombotic disorder) where autoantibodies to phospholipids are present in the patient's serum. Abnormalities associated with antiphospholipid antibody syndrome include a paradoxical prolonged PTT (which usually occurs in hemorrhagic disorders) and a positive test for antiphospholipid antibodies; the combination of such findings have earned the term "lupus anticoagulant positive". Another autoantibody finding in lupus is the anticardiolipin antibody which can cause a false positive test for syphilis.
- Cardiac manifestations
- Patients may present with inflammation of various parts of the heart, such as pericarditis, myocarditis, and endocarditis. The endocarditis of SLE is characteristically non-infective (Libman-Sacks endocarditis) and involves either the mitral valve or the tricuspid valve. Atherosclerosis also tends to occur more often and advance more rapidly in SLE patients than in the general population.[18][19][20]
- Pulmonary manifestations
- Lung and pleura inflammation can cause pleuritis, pleural effusion, lupus pneumonitis, chronic diffuse interstitial lung disease, pulmonary hypertension, pulmonary emboli, pulmonary hemorrhage.
- Hepatic involvement
- See autoimmune hepatitis
- Renal involvement
- Painless hematuria or proteinuria may often be the only presenting renal symptom. Acute or chronic renal impairment may develop with lupus nephritis, leading to acute or end stage renal failure. Because of early recognition and management of SLE, end stage renal failure occurs in less than 5% of patients.
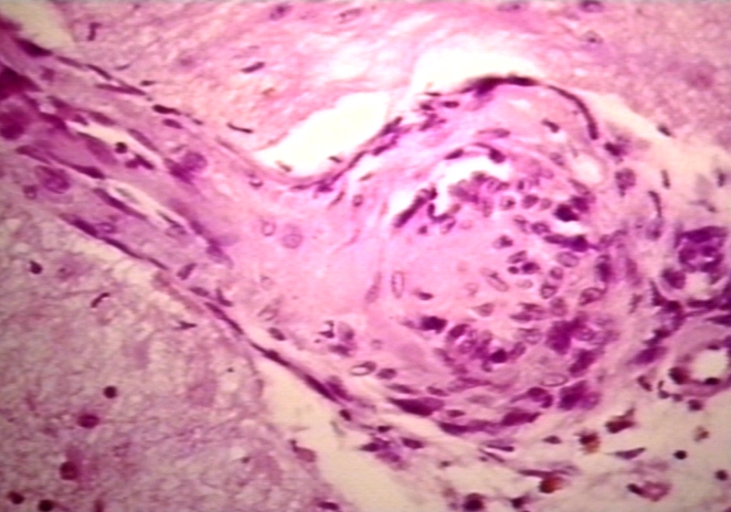
- Histologically, a hallmark of SLE is membranous glomerulonephritis with "wire loop" abnormalities.[21] This finding is due to immune complex deposition along the glomerular basement membrane leading to a typical granular appearance in immunofluorescence testing.
- Neurological manifestations
- About 10% of patients may present with seizures or psychosis. A third may test positive for abnormalities in the cerebrospinal fluid.
- T-cell abnormalities
- Abnormalities in T cell signaling are associated with SLE, including deficiency in CD45 phosphatase and increased expression of CD40 ligand.
- Other rarer manifestations
- lupus gastroenteritis, lupus pancreatitis, lupus cystitis, autoimmune inner ear disease, parasympathetic dysfunction, retinal vasculitis, and systemic vasculitis.
Other abnormalities include:
- Increased expression of FcεRIγ, which replaces the sometimes deficient TCR ζ chain
- Increased and sustained calcium levels in T cells
- Moderate increase of inositol triphosphate
- Reduction in PKC phosphorylation
- Increased desire of animal protein intake.
- Reduction in Ras-MAP kinase signaling
- Deficiencies in protein kinase A I activity
Diagnosis
Antinuclear antibody (ANA) testing and anti-extractable nuclear antigen (anti-ENA) form the mainstay of serologic testing for SLE.Several techniques are used to detect ANAs.Clinically the most widely used method is indirect immunofluorescence.The pattern of fluorescence suggests the type of antibody present in the patient's serum.
ANA screening yields positive results in many connective tissue disorders and other autoimmune diseases, and may occur in normal individuals. Subtypes of antinuclear antibodies include anti-Smith and anti-double stranded DNA (dsDNA) antibodies (which are linked to SLE) and anti-histone antibodies (which are linked to drug-induced lupus). Anti-dsDNA antibodies are highly specific for SLE; they are present in 70% of cases, whereas they appear in only 0.5% of people without SLE.[10] The anti-dsDNA antibody titers also tend to reflect disease activity, although not in all cases.[10] Other ANA that may occur in SLE sufferers are anti-U1 RNP (which also appears in systemic sclerosis), SS-A (or anti-Ro) and SS-B (or anti-La; both of which are more common in Sjögren's syndrome). SS-A and SS-B confer a specific risk for heart conduction block in neonatal lupus.[22]
Other tests routinely performed in suspected SLE are complement system levels (low levels suggest consumption by the immune system), electrolytes and renal function (disturbed if the kidney is involved), liver enzymes, complete blood count and recently By proteomics, we can directly detect proteins as gene products as well as their alterations by post-translational modification and internal abscission which are characteristically observed in proteins.[23]
Previously, the lupus erythematosus (LE) cell test was not commonly used for diagnosis because those LE cells are only found in 50–75% of SLE cases, and are also found in some people with rheumatoid arthritis, scleroderma, and drug sensitivities. Because of this, the LE cell test is now performed only rarely and is mostly of historical significance.[24]
As a summary:
- Medical history
- Complete physical examination
- Laboratory tests:
- Complete blood count (CBC)
- Erythrocyte sedimentation rate (ESR)
- Urinalysis
- Blood chemistries
- Complement levels
- Antinuclear antibody test (ANA)
- Other autoantibody tests (anti-DNA, anti-Sm, anti-RNP, anti-Ro [SSA], anti-La [SSB])
- Anticardiolipin antibody test
- Skin biopsy
- Kidney biopsy
Diagnostic criteria
Some physicians make a diagnosis on the basis of the ACR classification criteria (see below). The criteria, however, were established mainly for use in scientific research (i.e. inclusion in randomized controlled trials), and patients may have lupus but never meet the full criteria.
Anti-nuclear antibody testing and anti-extractable nuclear antigen (anti-ENA) form the mainstay of serologic testing for lupus. Antiphospholipid antibodies occur more often in SLE, and can predispose for thrombosis. More specific are the anti-smith and anti-dsDNA antibodies. Other tests routinely performed in suspected SLE are complement system levels (low levels suggest consumption by the immune system), electrolytes and renal function (disturbed if the kidney is involved), liver enzymes and a complete blood count.
Formerly, the lupus erythematosus (LE) cell test was used for diagnosis, however those LE cells are only found in 50-75% of SLE patients, and are also found in some patients with rheumatoid arthritis, scleroderma, and drug sensitivities. Because of this, the LE cell test is now performed only rarely and is mostly of historical significance. [25]
The American College of Rheumatology (ACR) has established eleven criteria in 1982,[26] which were revised in 1997[27] as a classificatory instrument to operationalise the definition of SLE in clinical trials. They were not intended to be used to diagnose individual patients and do not do well in that capacity.
For inclusion in clinical trials, patients must meet the following three criteria to be classified as having SLE:
- (i) patient must present with four of the below eleven symptoms
- (ii) either simultaneously or serially
- (iii) during a given period of observation.
- Malar rash (rash on cheeks). sensitivity = 57%; specificity = 96%[28]
- Discoid lupus (red, scaly patches on skin which cause scarring) sensitivity = 18%; specificity = 99%[28]
- Photosensitivity (exposure to ultraviolet light causes rash). sensitivity = 43%; specificity = 96%[28]
- Oral ulcers: include oral or nasopharyngeal ulcers
- Arthritis: nonerosive arthritis of two or more peripheral joints, with tenderness, swelling or effusionsensitivity = 86%; specificity = 37%[28]
- Renal disorder: More than 0.5 g per day protein in urine, or cellular casts seen in urine under a microscope.sensitivity = 51%; specificity = 94%[28]
- Neurologic disorder: Seizures or psychosis. sensitivity = 20%; specificity = 98%[28]
- Serositis: Pleuritis (inflammation of the membrane around the lungs) or pericarditis (inflammation of the membrane around the heart)sensitivity = 56%; specificity = 86% (pleural is more sensitive; cardiac is more specific)[28]
- Hematologic disorder: Hemolytic anemia (low red blood cell count) or leukopenia (white blood cell count<4000/ul), lymphopenia ( <1500/ul ) or thrombocytopenia (<100000/uL) in the absence of offending drug.sensitivity = 59%; specificity = 89%[28] Hypocomplementemia is also seen, due to either consumption of C3 and C4 by immune complex-induced inflammation, or to congenitally complement deficiency, which may predispose to SLE.
- Anti-nuclear antibody test positive. sensitivity = 99%; specificity = 49%[28]
- Immunologic disorder: Positive anti-Sm, anti-ds DNA, anti-phospholipid antibody and/or false positive serological test for syphilis. sensitivity = 85%; specificity = 93%[28]. Presence of anti-ss DNA in 70% of patients (though also positive in patients with rheumatic disease and healthy persons[29])
A useful mnemonic for these 11 criteria is SOAP BRAIN MD
- Serositis
- Oral ulcers
- Arthritis
- Photosensitivity
- Blood Changes
- Renal involvement (proteinuria or casts)
- ANA
- Immunological changes
- Neurological signs (seizures, frank psychosis)
- Malar Rash
- Discoid Rash
Some patients, especially those with antiphospholipid syndrome, may have SLE without four criteria and SLE is associated with manifestations other than those listed in the criteria.[30][31][32]
Alternative criteria
Recursive partitioning has been used to identify more parsimonious criteria. [28] This analysis presented two diagnostic classification trees:
1. Simplest classification tree: LSE is diagnosed if the patient has an immunologic disorder (anti-DNA antibody, anti-Smith antibody, false positive syphilis test, or LE cells) or malar rash.
- sensitivity = 92%
- specificity = 92%
2. Full classification tree: Uses 6 criteria.
- sensitivity = 97%
- specificity = 95%
Other alternative criteria have been suggested.[33]
Common misdiagnoses
Porphyria
Porphyrias are complex genetic disorders that share many symptoms with lupus, but impact the enzymes responsible for building heme, a component needed in heme proteins. Porphyrias are ecogenic disorders requiring both environmental and genetic backgrounds to manifest with a variety of symptoms and medical complications. They are noted for photosensitivity and have been associated with transient and permanent production of autoantibodies. The five major forms of dominantly inherited porphyrias (acute intermittent porphyria, porphyria cutanea tarda, hereditary coproporphyria, variegate porphyria and erythropoietic protoporphyria) have been detected in systemic lupus erythematosus and discoid lupus patients over the past 50 years. Physicians should have a high degree of suspicion of porphyrias in all lupus cases and act accordingly when patients are in a medical crisis that may be due to an underlying acute hepatic porphyria. Drug-induced lupus and photosensitivity warrant an investigation for an underlying porphyria since multiple drug reactions are a hallmark complication of porphyrias. Patients with both lupus and porphyrias should avoid porphyrinogenic drugs and hormone preparations.
Patients with acute hepatic porphyrias (acute intermittent porphyria, hereditary coproporphyria, variegate porphyria) have been detected in lupus patients with severe life-threatening "lupus" complications known as neurolupus. Symptoms are identical to acute hepatic porphyria attacks and include seizures, psychosis, peripheral neuropathy and syndrome of inappropriate antidiuretic hormone (SIADH) associated with dangerously low sodium levels (hyponatremia). Porphyria attacks require intervention with intravenous glucose, heme preparations and the discontinuation of dangerous porphyrinogenic drugs including antiseizure drugs. Several other lupus complications have been associated with porphyrias including pancreatitis and pericarditis. Porphyrin testing should be performed on urine, stool/bile and blood to detect all types of porphyrias, and repeat testing should be performed in suspicious cases. Appropriate enzyme tests or DNA testing should also be pursued to obtain a complete diagnosis which could include a dual porphyria.
Common dual diagnoses
SLE is sometimes diagnosed in conjunction with other conditions, including Rheumatoid Arthritis, Scurvy and Fibromyalgia.
Treatment
As lupus erythematosus is a chronic disease with no known cure, treatment is restricted to dealing with the symptoms; essentially this involves preventing flares and reducing their severity and duration when they occur. There are several means of preventing and dealing with flares, including drugs, alternative medicine and lifestyle changes.
Drug therapy
Due to the variety of symptoms and organ system involvement with Lupus patients, the severity of the SLE in a particular patient must be assessed in order to successfully treat SLE. Mild or remittent disease can sometimes be safely left untreated. If required, non-steroidal anti-inflammatory drug and anti-malarials may be used.[34]
Disease-modifying antirheumatic drugs (DMARDs) are used preventively to reduce incidence of flares, the process of the disease, and lower the need for steroid use; when flares occur, they are treated with corticosteroids. DMARDs commonly in use are anti-malarials and immunosupressants (e.g. methotrexate and azathioprine). Hydroxychloroquine (trade name Plaquenil) is an FDA approved anti-malarial used for constitutional, cutaneous, and articular manifestations, while Cyclophosphamide (trade names Cytoxan and Neosar) is used for severe glomerulonephritis or other organ-damaging complications, and in 2005, CellCept became accepted for treatment of lupus nephritis.
In more severe cases, medications that modulate the immune system (primarily corticosteroids and immunosuppressants) are used to control the disease and prevent re-occurrence of symptoms (known as flares[8]). Patients who require steroids frequently may develop obesity, diabetes and osteoporosis. Depending on the dosage, corticosteroids can cause other side effects such as a puffy face, an unusually large appetite and difficulty sleeping. Those side effects can subside if and when the large initial dosage is reduced, but long term use of even low doses can cause elevated blood pressure and cataracts. Due to these side effects, steroids are avoided if possible.
Since a large percentage of Lupus patients suffer from varying amounts of chronic pain, stronger prescription analgesics may be used if over-the-counter drugs, mainly non-steroidal anti-inflammatory drug do not provide effective relief. Moderate pain in Lupus patients if typically treated with mild prescription opiates such as Dextropropoxyphene (trade name Darvocet), and Co-codamol (trade name Tylenol #3). Moderate to severe chronic pain is treated with stronger opioids such as Hydrocodone (trade names Lorcet, Lortab, Norco, Vicodin, Vicoprofen) or longer-acting continuous release opioids such as Oxycodone (trade names OxyContin), MS Contin, or Methadone. The Fentanyl Duragesic Transdermal patch is also a widely-used treatment option for chronic pain due to Lupus complications because of its long-acting timed release and easy usage. When opioids are used for prolonged periods drug tolerance, chemical dependency and (rarely) addiction may occur. Opiate addiction is not typically a concern for Lupus patients, since the condition is not likely to ever completely disappear. Thus, lifelong treatment with opioids is fairly common in Lupus patients that exhibit chronic pain symptoms; accompanied by periodic increased titration that is typical of any long-term opioid regimen.
Acupuncture
A 1985 study on lupus and acupuncture reported improvement of lupus sufferers over matched controls, though there was no placebo group for comparison.[35] It is possible that acupuncture may be useful for the treatment some of the symptoms of lupus, but there needs to be more research done before a definitive statement can be made regarding acupuncture. [36]
UVA1 Phototherapy
In 1987, Tina Lomardi, MD first reported that long-wave ultraviolet radiation (UVA1) had a favorable effect on disease activity in SLE model mice. Several clinicals trials investigating this new, counter-intuitive therapeutic approach, conducted by both McGrath and independent Dutch searchers, have confirmed these findings in SLE patients. [37] Devices for administering therapeutic doses of UVA1 are available in Europe but not in the U.S. However, the U.S. Food and Drug Administration Office of Science and Technology conducted UVA1 phototherapy studies in an SLE mouse model in 1997 “to prepare for future reviews of UVA-emitting tanning devices for such clinical applications." [4]
Lifestyle changes
Other measures such as avoiding sunlight or covering up with sun protective clothing can also be effective in preventing problems due to photosensitivity. Weight loss is also recommended in overweight and obese patients to alleviate some of the effects of the disease, especially where joint involvement is significant.
Renal transplantation
is the treatment of choice for end-stage renal disease, which is one of the complications of lupus nephritis, but the recurrence of the full disease is common in up to 30% of patients.[38]
Treatment Research
Other immunosuppressants and autologous stem cell transplants are under investigation as a possible cure. Recently, treatments that are more specific in modifying the particular subset of the immune cells (e.g. B- or T- cells) or cytokine proteins they secrete have been gaining attention. Research into new treatments has recently been accelerated by genetic discoveries, especially mapping of the human genome. According to a June 2006 market analysis report by Datamonitor, treatment for SLE could be on the verge of a breakthrough as there are numerous late-Phase trials currently being carried out.[39]
Prevention
Lupus is not understood well enough to be prevented, but when the disease develops, quality of life can be improved through flare prevention. The warning signs of an impending flare include increased fatigue, pain, rash, fever, abdominal discomfort, headache and dizziness. Early recognition of warning signs and good communication with a doctor can help individuals with lupus remain active, experience less pain and reduce medical visits.[8]
Prevention of complications during pregnancy
While most infants born to mothers who have SLE are healthy, pregnant mothers with SLE should remain under a doctor's care until delivery. Neonatal lupus is rare, but identification of mothers at highest risk for complications allows for prompt treatment before or after birth. In addition, SLE can flare during pregnancy, and proper treatment can maintain the health of the mother longer. Women pregnant and known to have the antibodies for anti-Ro (SSA) or anti-La (SSB) should have echocardiograms during the 16th and 30th weeks of pregnancy to monitor the health of the heart and surrounding vasculature.[8]
Even contraception was routinely advised in treating SLE patients, getting pregnant during active disease was eventually found. Lupus nephritis was the most common manifestation. Overall live-birth was 72.7%. Pregnancy lost was due to abortion and dead fetus in utero. Pregnancy outcome was worse in SLE patients who had disease flares up or emerging during pregnancy.[40]
Prognosis
In the 1950s, most people diagnosed with SLE lived fewer than five years. Advances in diagnosis and treatment have improved survival to the point where over 90% now survive for more than ten years, and many can live relatively asymptomatically. Prognosis is normally worse for men and children than for women; however, if symptoms are present after age 60, the disease tends to run a more benign course. Early mortality, within 5 years, is due to organ failure or overwhelming infections, both of which can be modified by early diagnosis and treatment. The mortality risk is five-fold when compared to the normal population in the late stages, which can be attributed to cardiovascular diseases acquired from corticosteroid therapy. To reduce potential for cardiovascular issues, steroids should be used at the lowest dose for the shortest possible period. High serum creatinine, hypertension, nephrotic syndrome, anemia and hypoalbuminemia are poor prognostic factors.[41]
The ANA is the most sensitive screening test for evaluation, whereas anti-Sm (anti-Smith) is the most specific. The dsDNA (double-stranded DNA) antibody is also fairly specific and often fluctuates with disease activity; as such, the dsDNA titer is sometimes useful to monitor disease flares or response to treatment.[42]
Lupus and Quality of Life
Despite the symptoms of lupus and the potential side-effects of treatment, people with lupus can maintain a high quality of life overall. One key to managing lupus is to understand the disease and its impact. Learning to recognize the warning signs of a flare can help the patient take steps to ward it off or reduce its intensity. Many people with lupus experience increased fatigue, pain, a rash, fever, abdominal discomfort, headache, or dizziness just before a flare. Developing strategies to prevent flares can also be helpful, such as learning to recognize your warning signals and maintaining good communication with your doctor.
It is also important for people with lupus to receive regular health care, instead of seeking help only when symptoms worsen. Results from a medical exam and laboratory work on a regular basis allows the doctor to note any changes and to identify and treat flares early. The treatment plan, which is tailored to the individual's specific needs and circumstances, can be adjusted accordingly. If new symptoms are identified early, treatments may be more effective. Other concerns also can be addressed at regular checkups. The doctor can provide guidance about such issues as the use of sunscreens, stress reduction, and the importance of structured exercise and rest, as well as birth control and family planning. Because people with lupus can be more susceptible to infections, the doctor may recommend yearly influenza vaccinations or pneumococcal vaccinations for some patients.
Women with lupus should receive regular preventive health care, such as gynecological and breast examinations. Men with lupus should have the prostate-specific antigen (PSA) test. Both men and women need to have their blood pressure and cholesterol checked on a regular basis. If a person is taking corticosteroids or antimalarial medications, an eye exam should be done at least yearly to screen for and treat eye problems.
Staying healthy requires extra effort and care for people with lupus, so it becomes especially important to develop strategies for maintaining wellness. Wellness involves close attention to the body, mind, and spirit. One of the primary goals of wellness for people with lupus is coping with the stress of having a chronic disorder. Effective stress management varies from person to person. Some approaches that may help include exercise, relaxation techniques such as meditation, and setting priorities for spending time and energy.
Developing and maintaining a good support system is also important. A support system may include family, friends, medical professionals, community organizations, and support groups. Participating in a support group can provide emotional help, boost self-esteem and morale, and help develop or improve coping skills.
Warning Signs of a Flare
Histopathological Findings
-
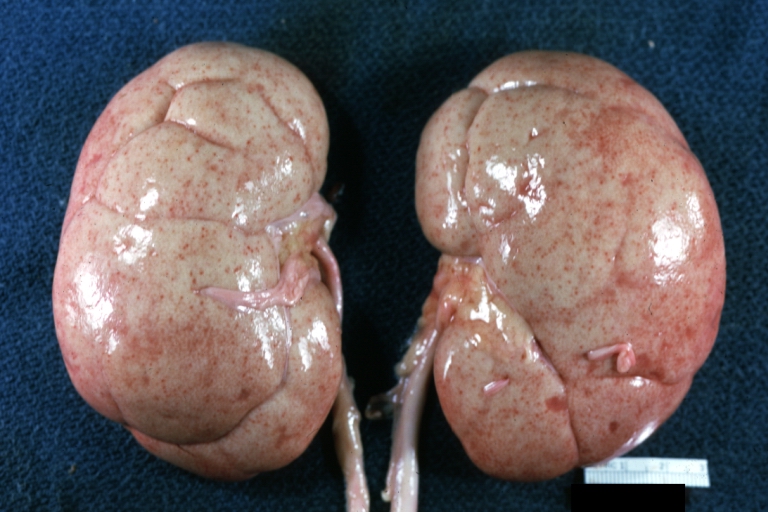
Kidney: Lupus erythematosus: Gross, enlarged very pale kidneys with flea bite or ectasia. A good example of kidneys from a patient with nephrotic syndrome (subacute glomerulonephritis)
-
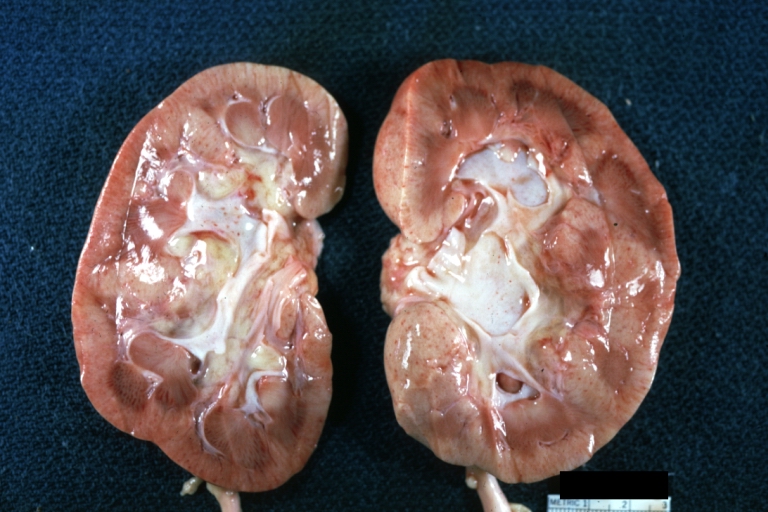
Kidney: Lupus erythematosus: Gross cut surface pale kidneys typical of nephrotic syndrome (subacute glomerulonephritis)
-
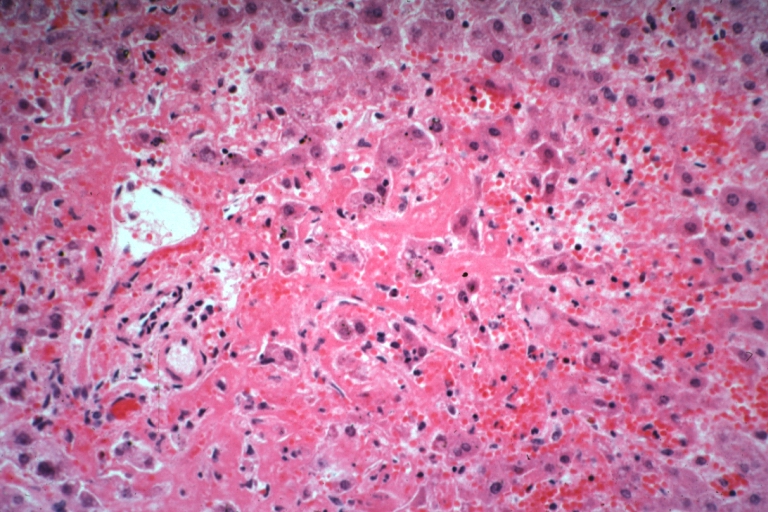
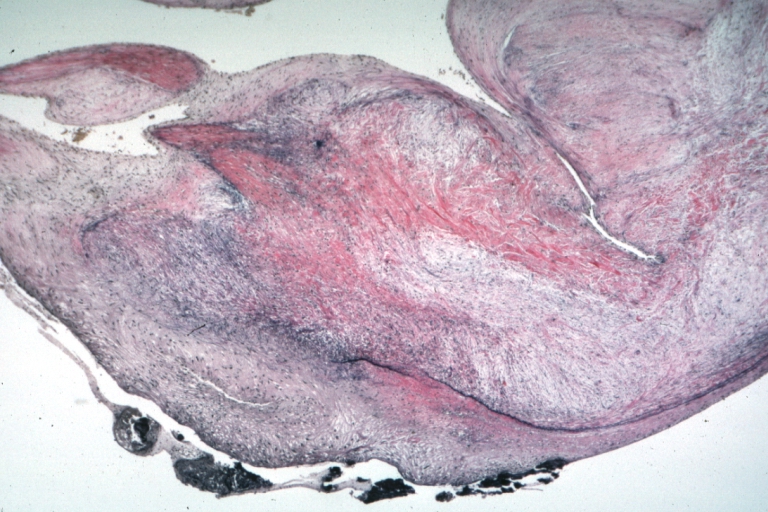
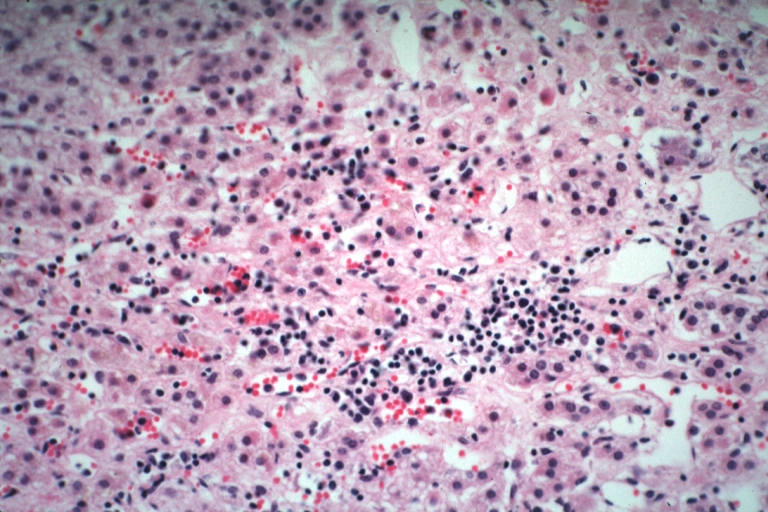
Lupus erythematosus hepatitis: Micro high mag H&E, periportal sinus thrombosis with liver cell necrosis and noninflammatory infiltrate (possibly viral). A 19yo female with lupus erythematosus
-
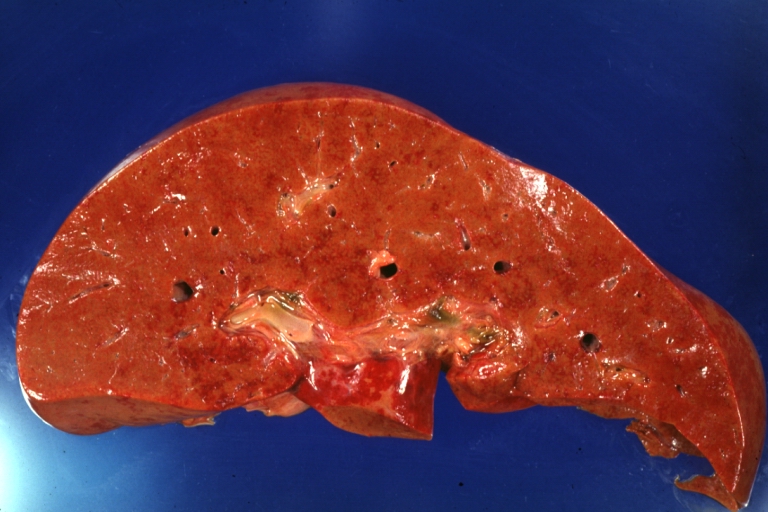
Lupus Erythematosus Hepatitis: Gross natural color. A 19yo female with lupus erythematosus and hepatitis characterized by periportal cell necrosis and sinus thrombosis cause uncertain photo shows focal grid-like hyperemia
-
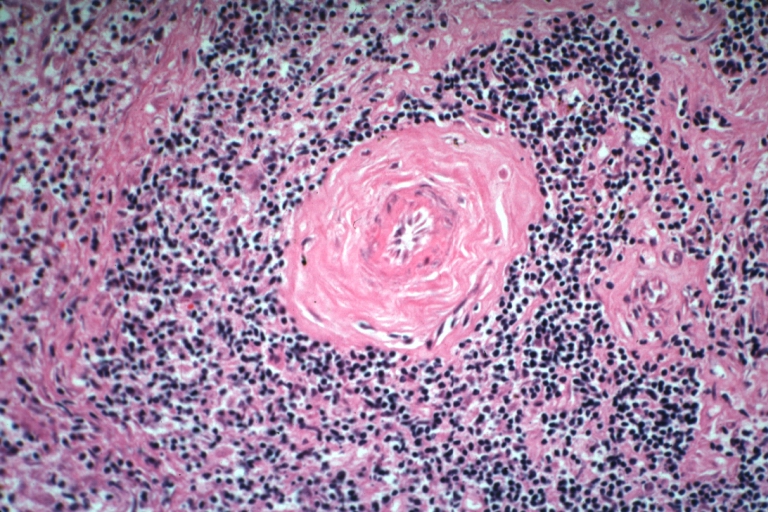
Spleen: Lupus erythematosus Periarterial Fibrosis: Micro high may H&E. An excellent example of periarterial fibrosis
-
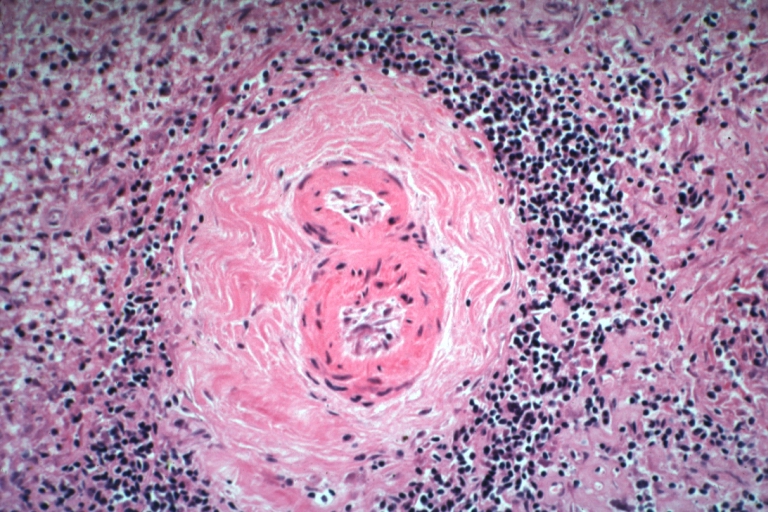
Spleen: Lupus erythematosus, periarterial fibrosis: Micro high may H&E. An excellent example of periarterial fibrosis
-
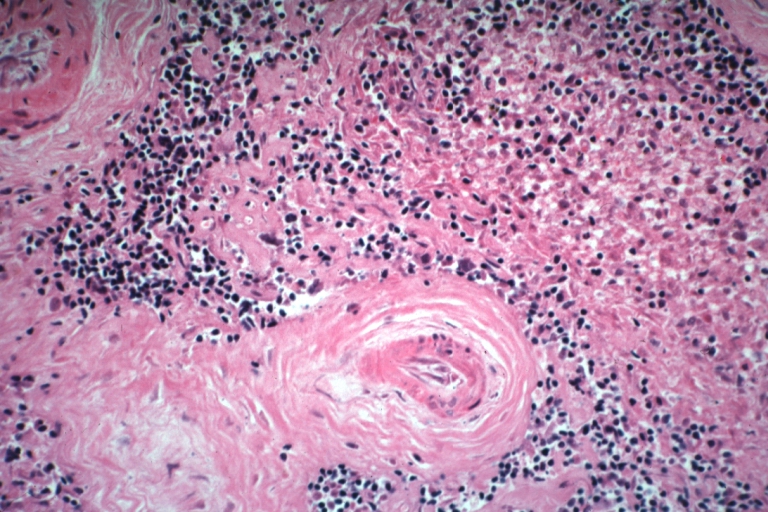
Spleen: Lupus erythematosus. Basophilic bodies and periarterial fibrosis: Micro high mag, H&E. Two basophilic bodies and periarterial fibrosis. An excellent example of this rarely seen lupus lesion.
-
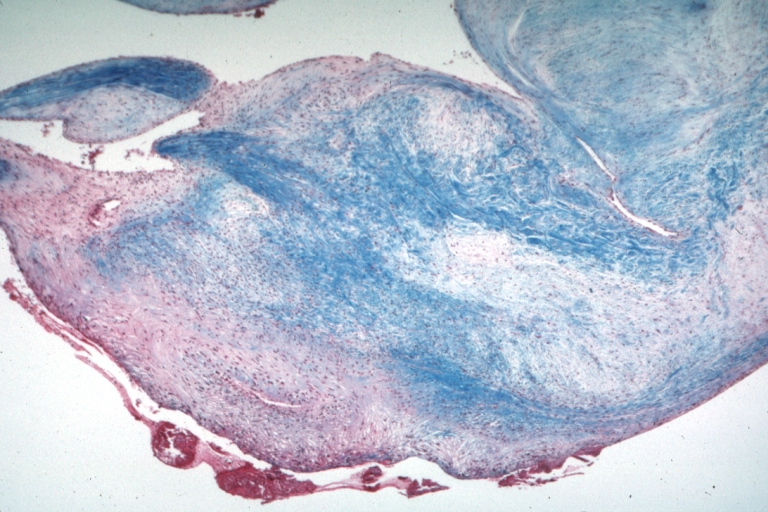
Lupus Erythematosus, Libman Sacks Endocarditis: Micro low mag trichrome stain thickened valve leaflet with small mural fibrin deposit. A 19yo female with cerebral lupus in form of TIAs due to this lesion.
-
Lupus Erythematosus, Libman Sacks Endocarditis: Micro low mag, elastic van Gieson stain, mitral valve thickened, leaflet with small mural fibrin deposit that caused TIAs in 19yo female
-
Adrenal: Autoimmune Adrenalitis: Micro high mag H&E focal area of lymphocytic infiltration in zona reticularis in a 19yo female with lupus erythematosus
-
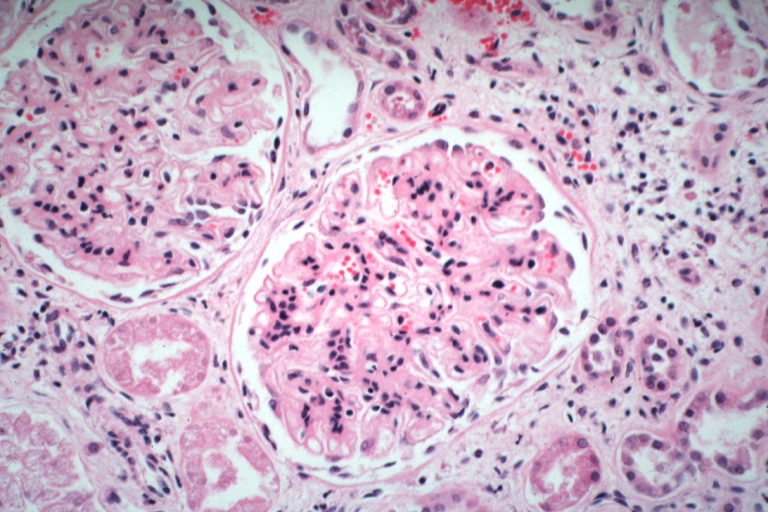
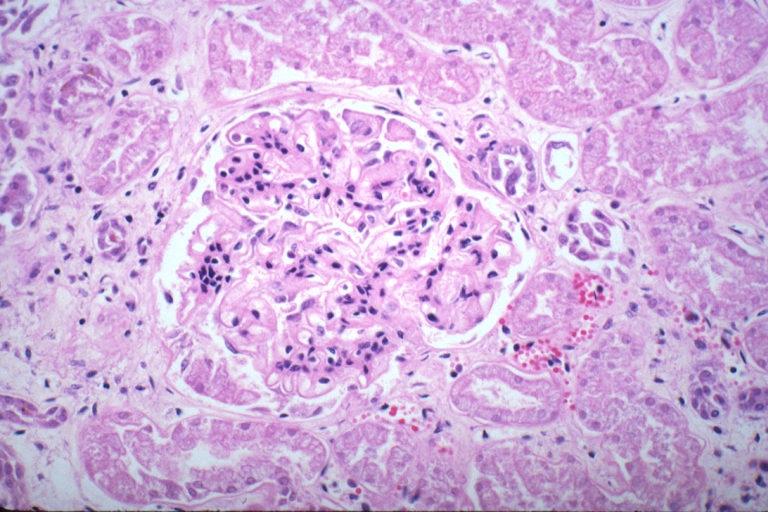
Kidney: Lupus Erythematosus: Micro high mag H&E two glomeruli showing mesangial thickening and focal wire loop type lesions 19yo female with renal failure and embolic brain disease from Libman Sacks lesion on mitral valve
-
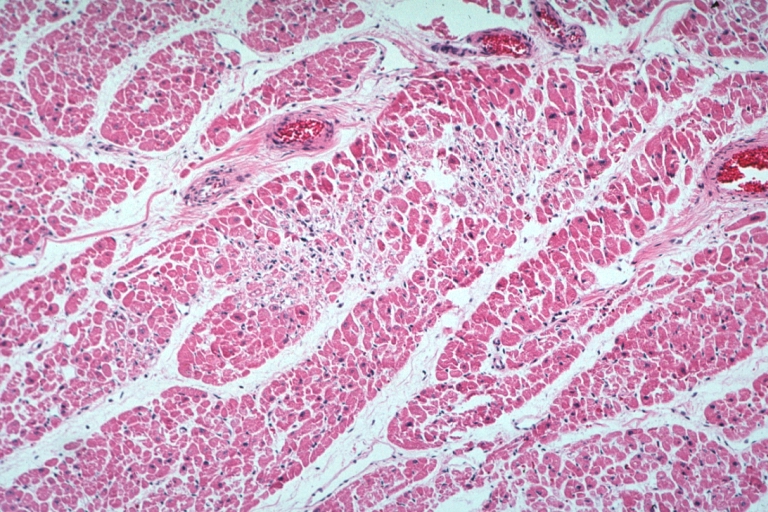
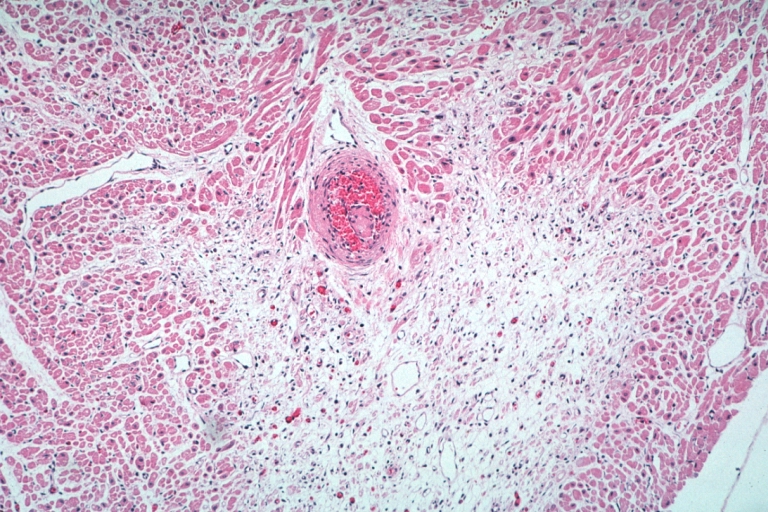
Lupus Erythematosus Myocardial Necrosis Due To Libman Sacks: Micro low mag H&E focal myocardial necrosis due to embolism from Libman Sacks lesion on mitral valve 19yo female with TIAs due to mitral lesion
-
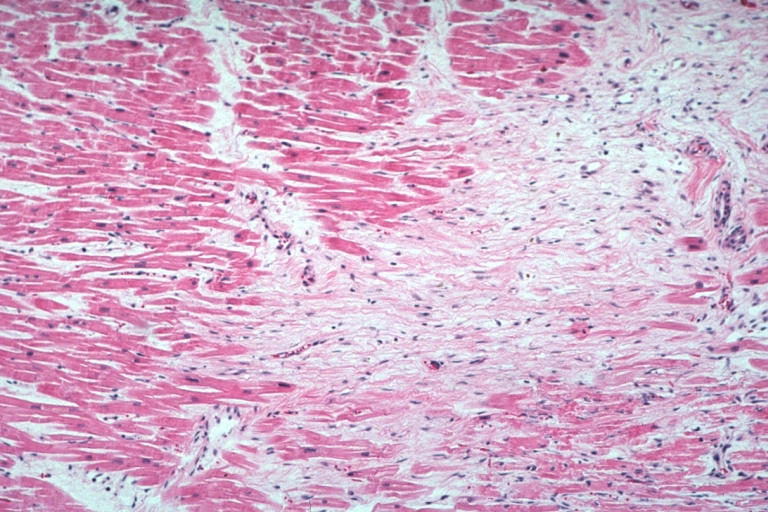
Lupus Erythematosus Focal Myocardial Scar Due To Libman Sacks Embolism: Micro low mag H&E focal scar in myocardium due to embolism
-
Lupus Erythematosus Myocardial Scar Due To Libman Sacks Embolism: Micro low mag H&E scar with portion of embolus in small artery
-
Lupus Erythematosus Myocardial Necrosis Due To Libman Sacks: Micro low mag H&E well shown focal myocardial necrosis due to embolism from mitral Libman Sacks lesion
-
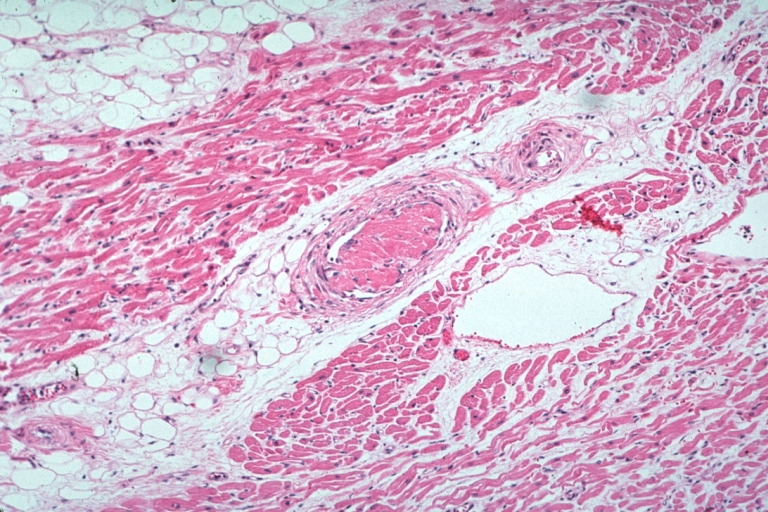
Lupus Erythematosus Embolus From Libman Sacks Lesion: Micro med mag H&E well shown embolus in small artery
-
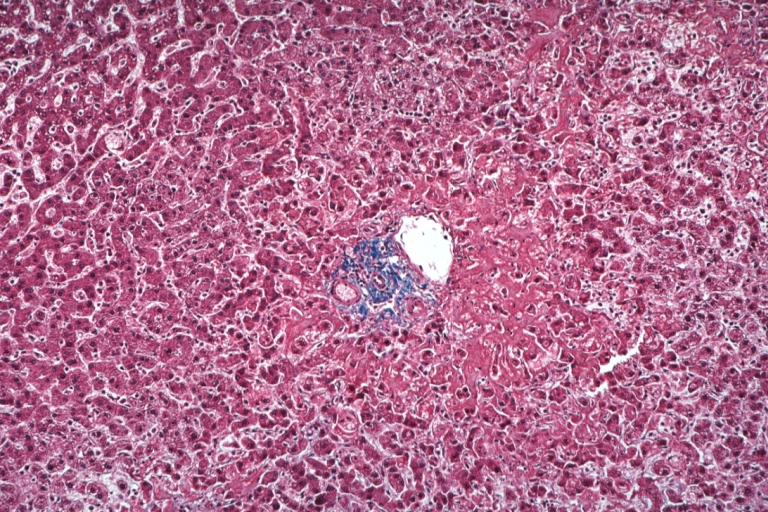
Lupus Erythematosus Hepatitis: Micro low mag trichrome stain periportal liver cell necrosis and sinus thrombosis with no inflammatory reaction cause unknown 19yo female with lupus erythematosus
-
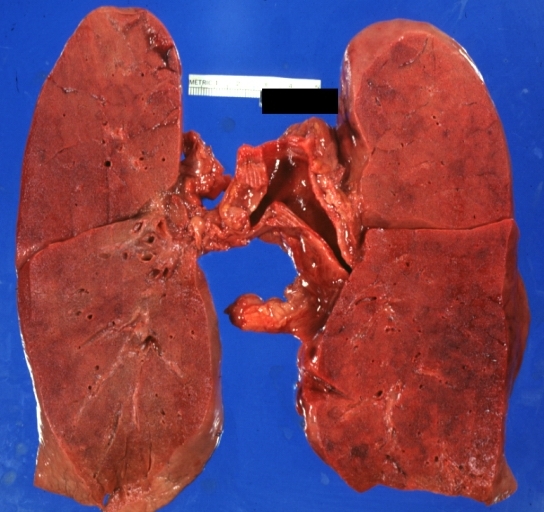
Lung: Diffuse Alveolar Damage: Gross natural color section of both lungs with frank meaty appearance case of lupus erythematosus in 19yo female
-
Kidney: Lupus Erythematosus: Micro high mag H&E increased mesangial tissue and wire loops 10yo female with renal failure and TIAs due to Libman Sacks endocarditis
-
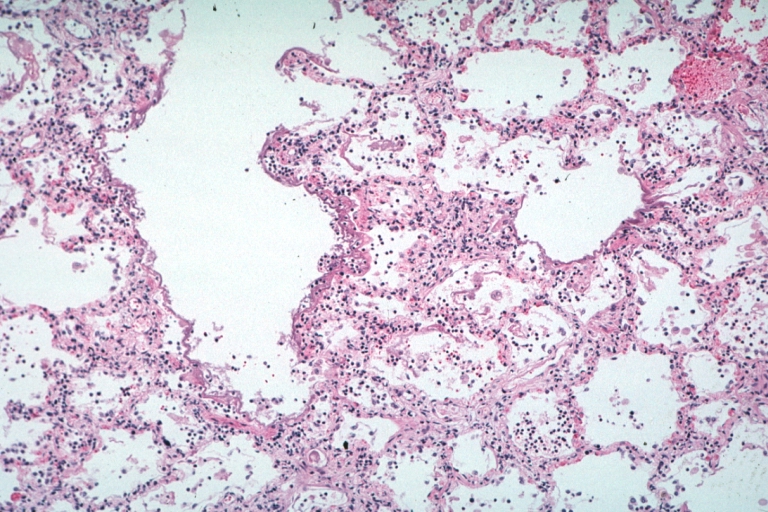
Lung: Necrotizing Bronchiolitis: Micro low mag H&E well shown lesion in lung that grossly looked like diffuse alveolar damage which indeed has lesions of this type additionally 19yo female with lupus erythematosus
-
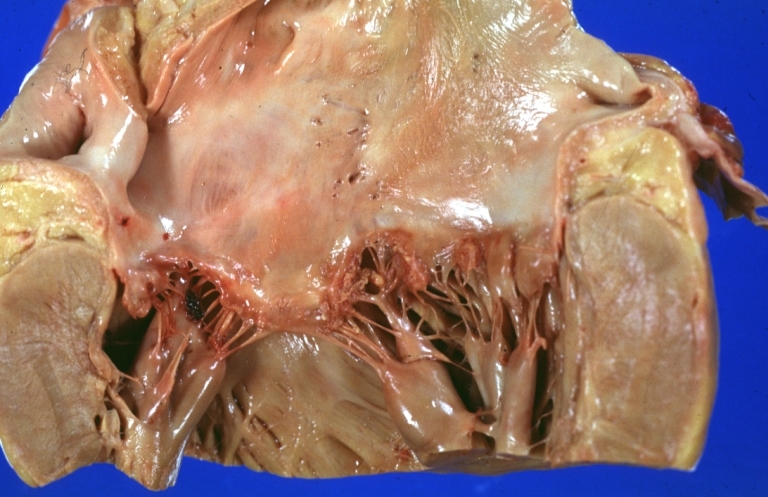
Lupus Erythematosus Libman Sacks Endocarditis: Gross natural color mitral valve small lesions but cause much trouble in form of TIAs and terminally multiple hemorrhagic brain infarcts
-
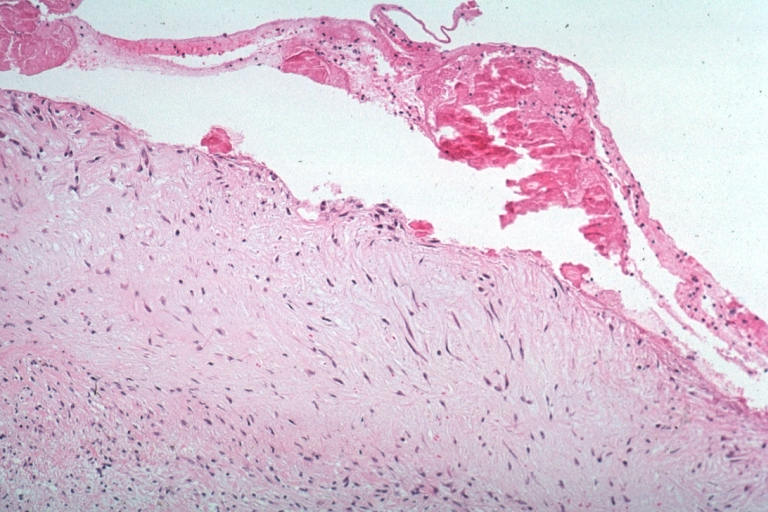
Lupus Erythematosus Libman Sacks Endocarditis: Micro high mag H&E atrial surface of mitral valve with small fibrin thrombus representing Libman Sacks lesion 10yo female
-
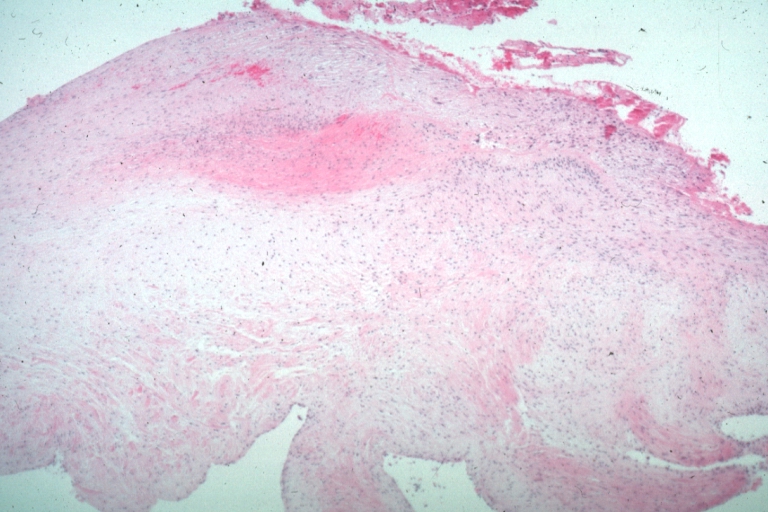
Lupus Erythematosus Libman Sacks Endocarditis: Micro low mag H&E mitral valve lesion with easily seen mural thrombi and focal necrobiosis of collagen in thickened valve leaflet 19yo female
-
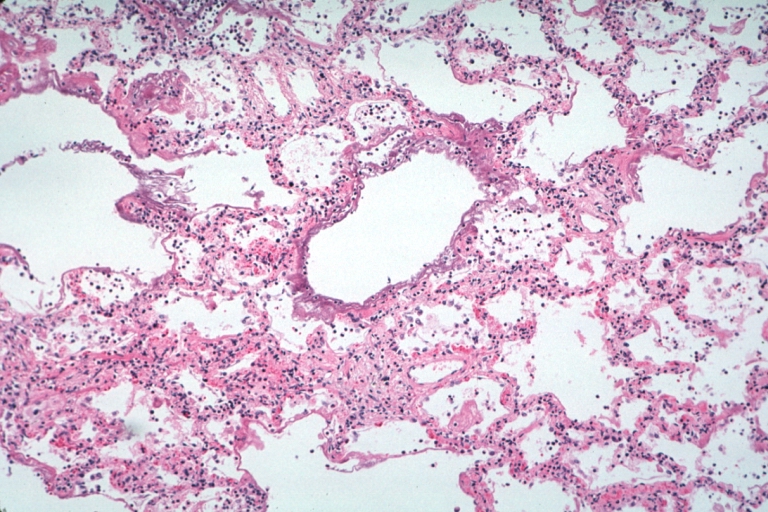
Lung: Necrotizing Bronchiolitis: Micro low mag H&E well shown necrotizing bronchiolitis and surrounding lesions of diffuse alveolar damage 19yo female with lupus erythematosus
-
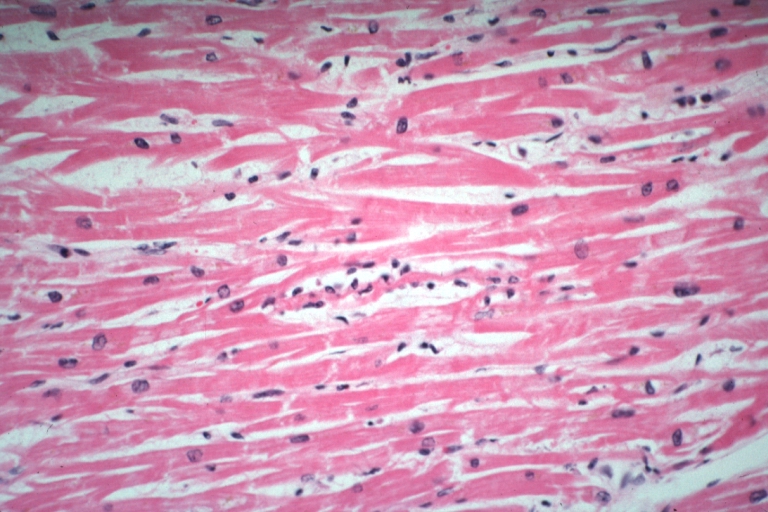
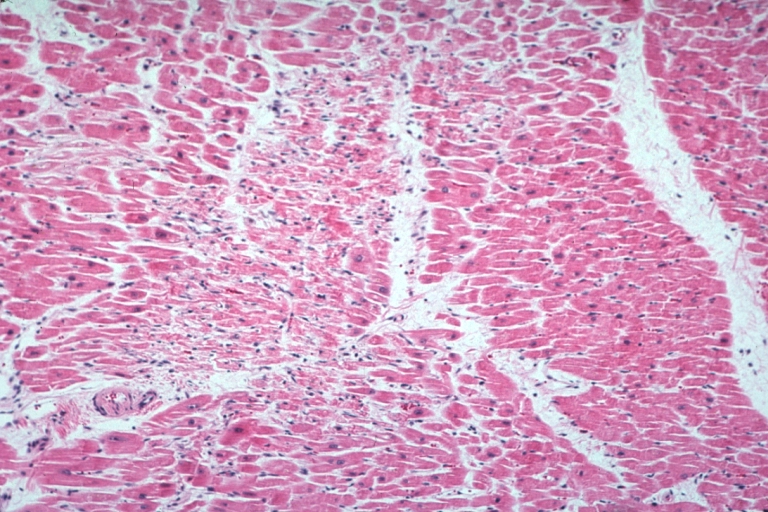
Myocarditis: Micro high mag H&E focal myofiber necrosis typical for this diagnosis but this is case of lupus erythematosus with Libman Sacks lesion and brain emboli and heart emboli did she also have viral myocarditis? This lesion is typical for the diagnosis
-
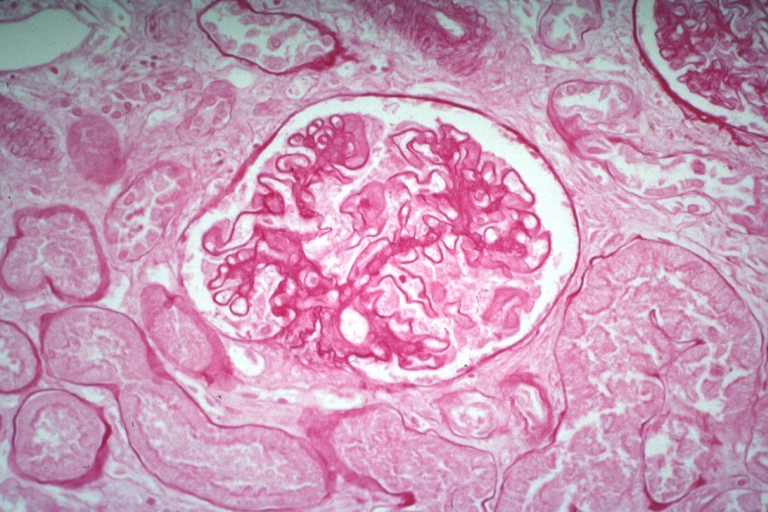
Kidney: Lupus Erythematosus: Micro high mag PAS stain thickened mesangium and capillary basement membranes 19yo female with renal failure and proved lupus
-
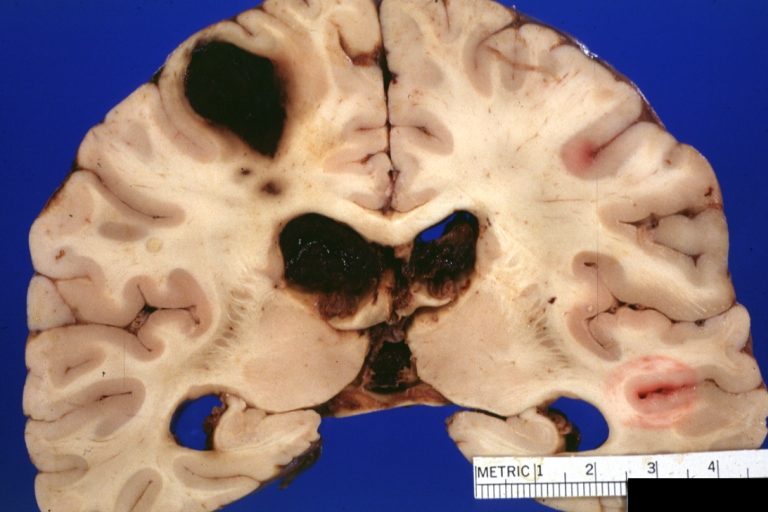
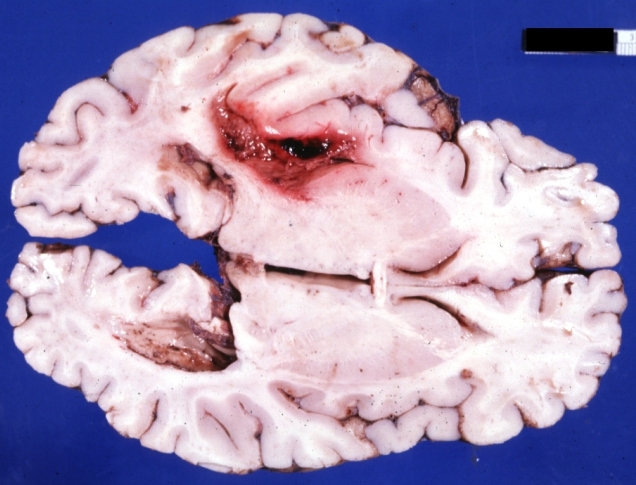
Brain: Lupus Erythematosus Libman Sacks Embolism: Gross fixed tissue one large and two small hemorrhages 19yo female with history of TIAs
-
Brain: Lupus Erythematosus Libman Sacks Embolism: Gross fixed tissue large hemorrhagic infarcts due to embolism 19yo female with known lupus and history of TIAs
-
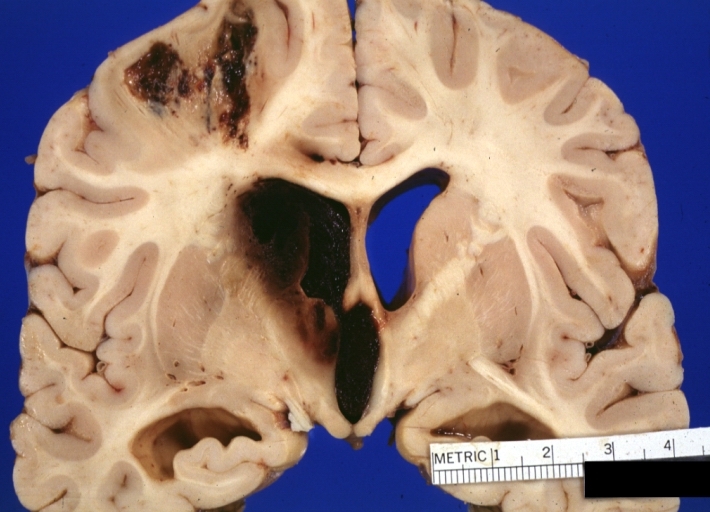
Brain: Lupus Erythematosus Libman Sacks Embolism: Gross large hemorrhagic infarcts 19 yo female with history of TIAs proved case lupus with renal failure
-
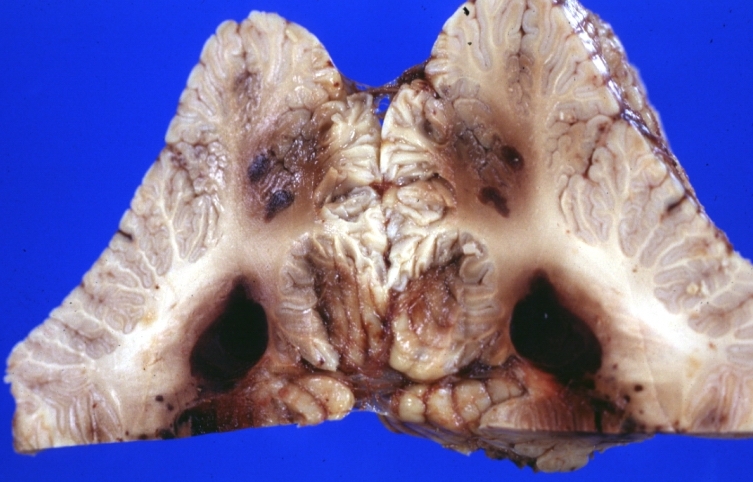
Brain: Lupus Erythematosus Libman Sacks Embolism: Gross fixed tissue cerebellar hemorrhagic infarcts 19yo female with history of TIAs known lupus case with renal failure
-
Brain: Purulent Meningitis: Gross fixed tissue excellent example Pneumococcus case of young girl with lupus
-
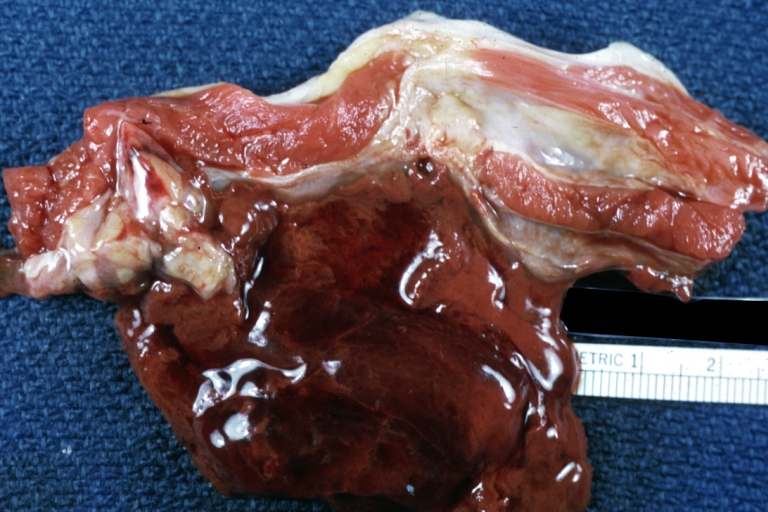
Skeletal muscle: Hematoma: Gross natural color flank muscle hematoma old showing typical chocolate appearance of blood coagulum young female with lupus and thrombocytopenia
-
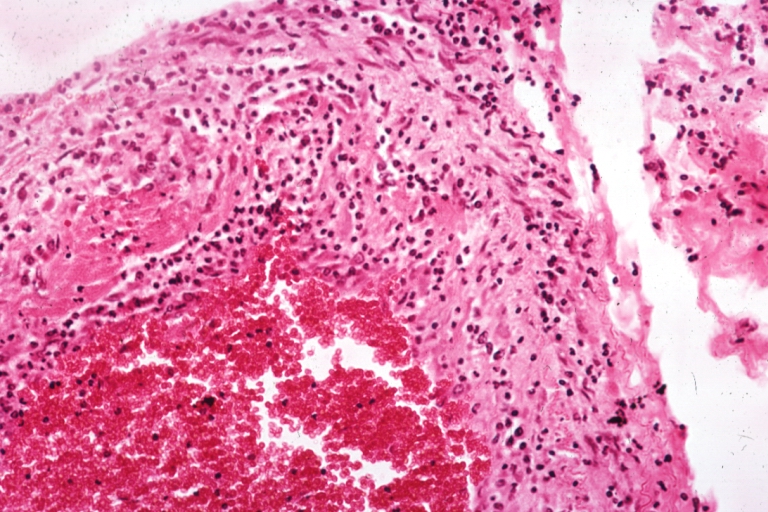
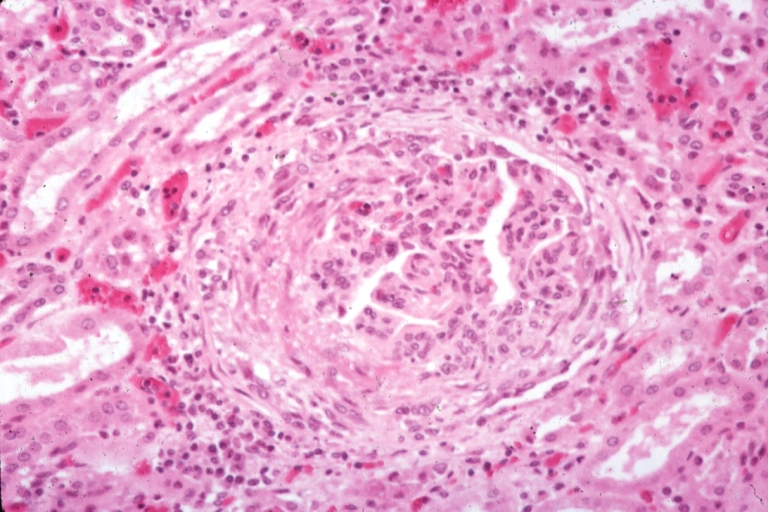
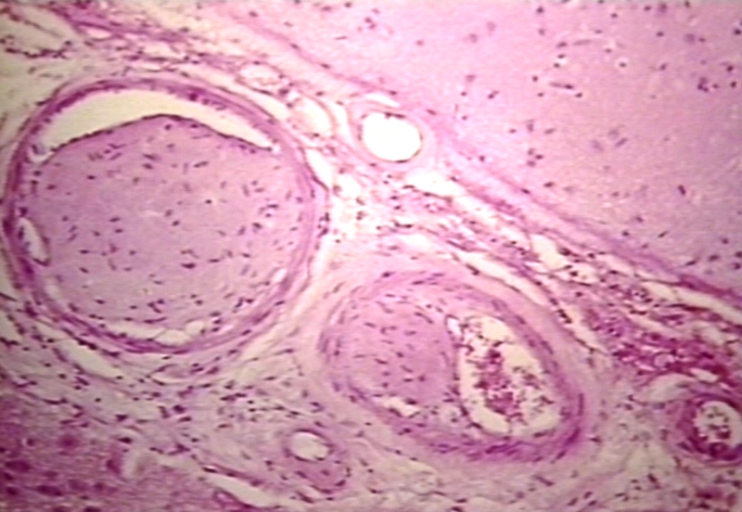
Artery: Arteritis in Lupus Erythematosus: Micro med mag H&E. A good example of vasculitis
-
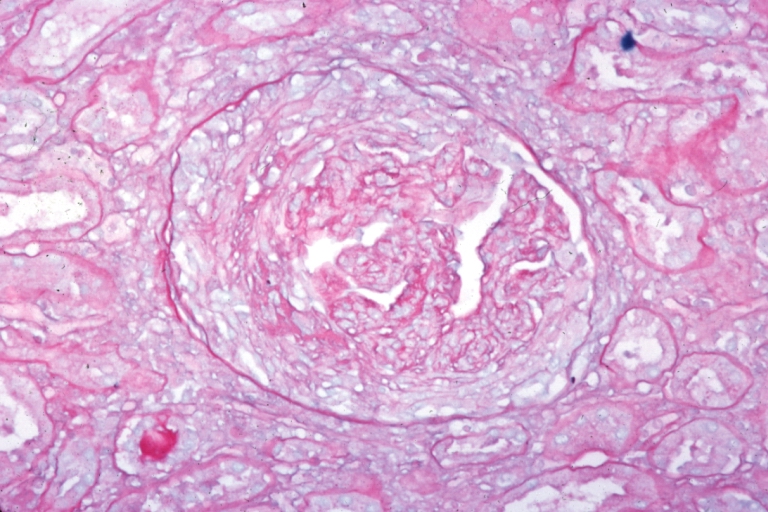
Kidney: Lupus Erythematosus: Micro high mag PASH typical glomerulonephritis lesion with crescent
-
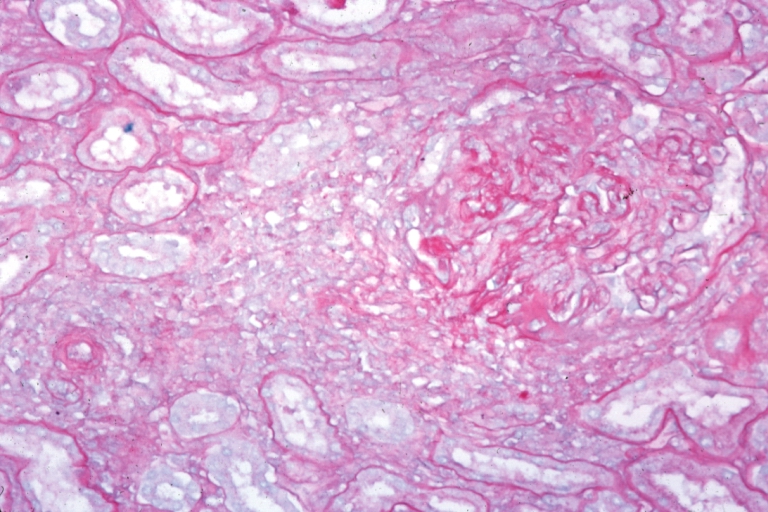
Kidney: Lupus Erythematosus: Micro med mag PASH glomerulonephritis
-
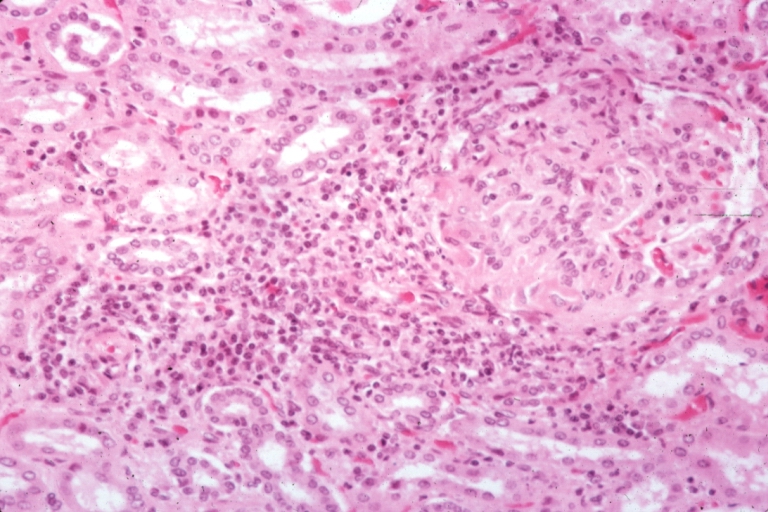
Kidney: Lupus Erythematosus: Micro med mag H&E typical glomerulonephritis lesion
-
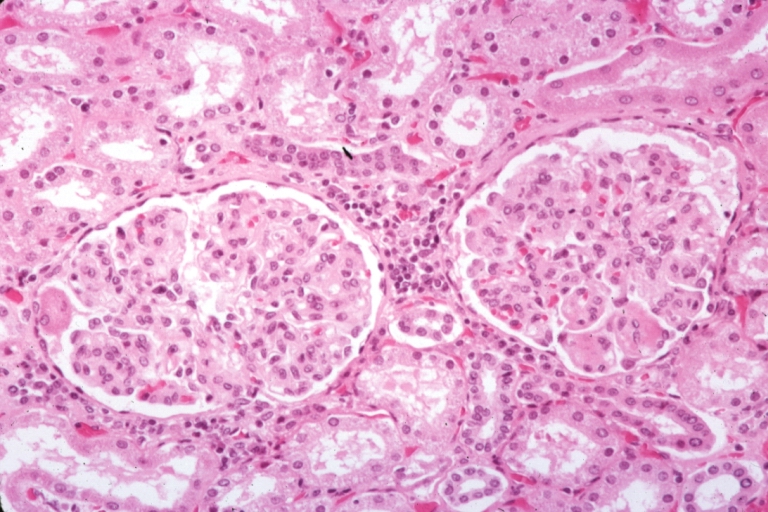
Kidney: Lupus Erythematosus: Micro med mag H&E two glomeruli showing lobular glomerulonephritis lesion
-
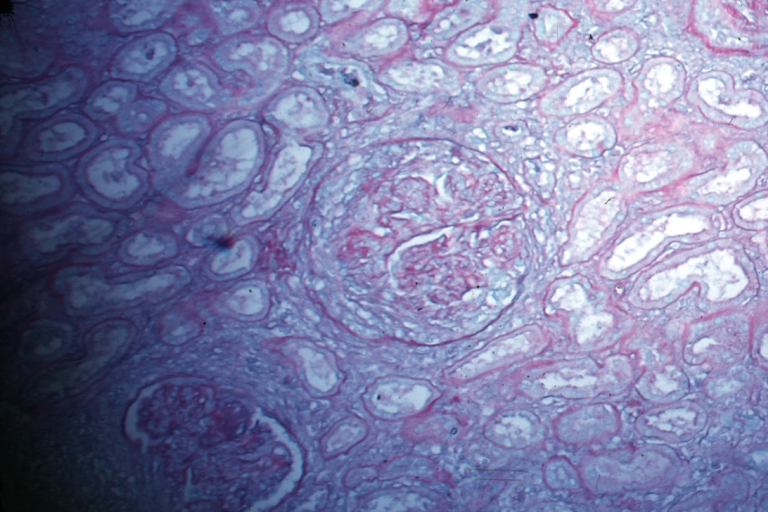
Kidney: Lupus Erythematosus: Micro med mag PASH typical chronic glomerulonephritis lesion with crescent
-
Kidney: Lupus Erythematosus: Micro high mag H&E. A nice example of a lesion of chronic glomerulonephritis with lobular scarring. A fibrous type crescent.
-
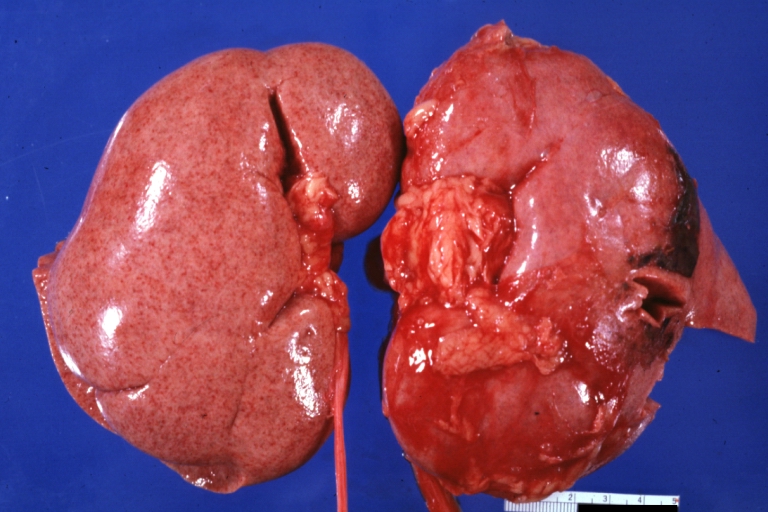
Kidney: Lupus Nephritis: Gross natural color external view of flea bitten kidneys quite good advanced proliferative type glomerulonephritis of lupus in a 16yo female
-
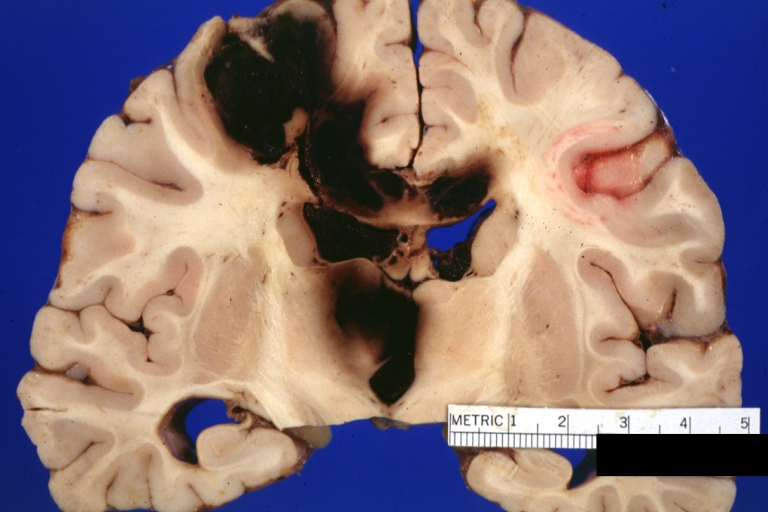
Brain: Hemorrhage Massive With Lupus Erythematosus: Gross apparently fresh tissue large left frontoparietal hemorrhagic infarct in a 16yo female with advanced lupus nephritis and sepsis
-
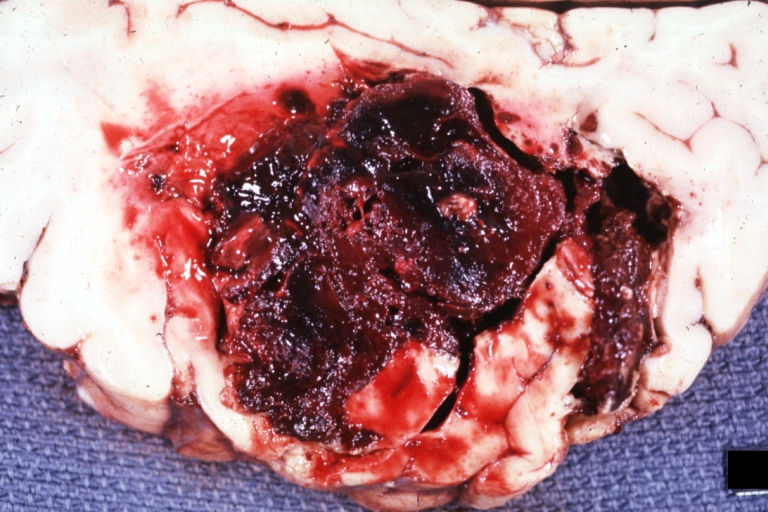
Brain: Hemorrhage Massive With Lupus Erythematosus: Gross natural color not the best exposure but OK large left frontoparietal hemorrhage in 16yo female with advanced lupus nephritis and sepsis
-
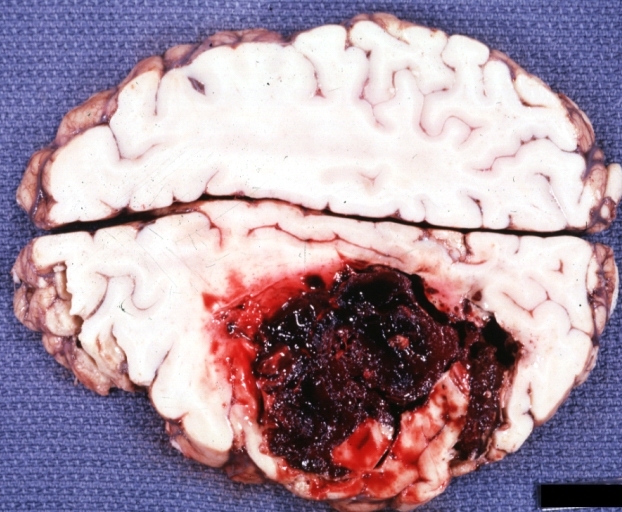
Brain: Hemorrhage Massive With Lupus Erythematosus: Gross natural color but not best exposure large left frontoparietal hemorrhage in 16yo female with advanced lupus nephritis and sepsis
-
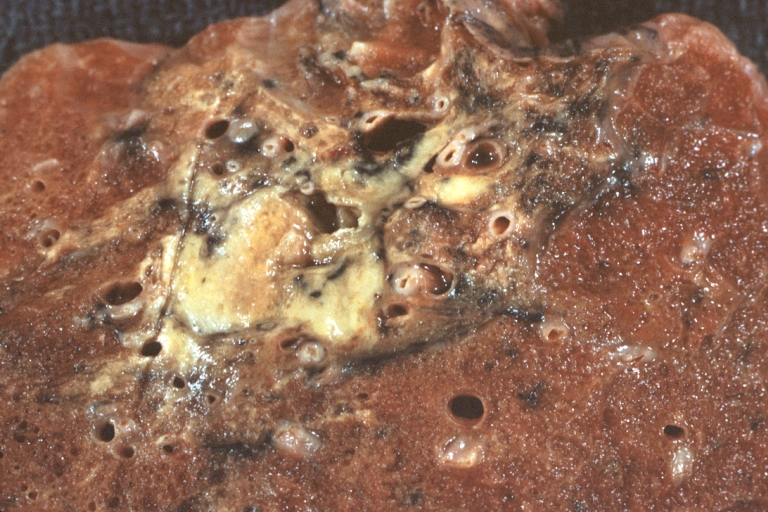
Lung: Tuberculosis Reactivation: Gross fixed tissue close-up of lung hilum with node and parenchyma lesions case of lupus erythematosus treated with prednisone for many years
-

Lung: Tuberculosis Reactivation: Gross fixed tissue close-up of lung showing lesions in nodes and parenchyma case of lupus erythematosus treated for long period with prednisone
-
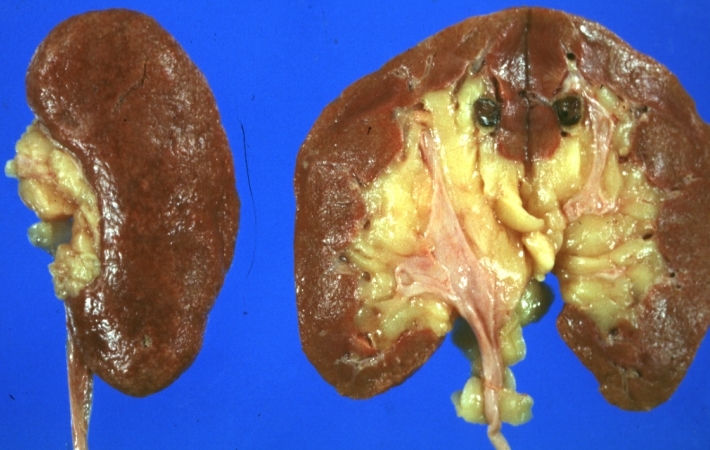
Kidney: Lupus Erythematosus: Gross natural color nice external and cut surface view of uniformly scarred and moderately shrunken kidneys
-

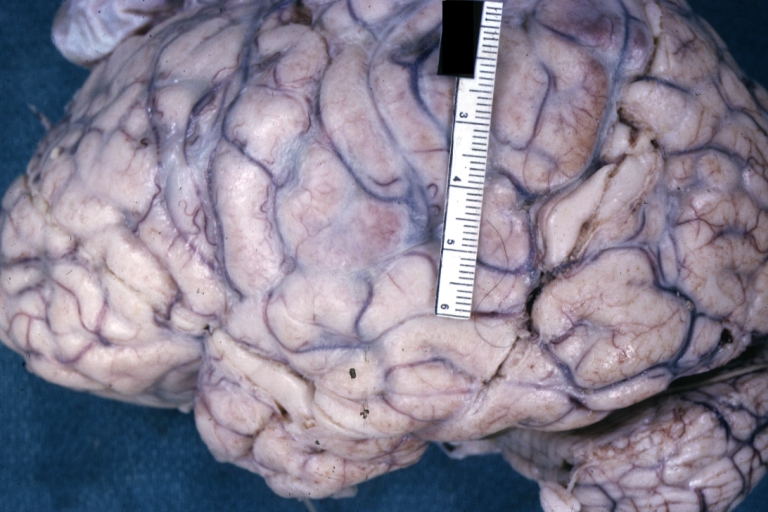
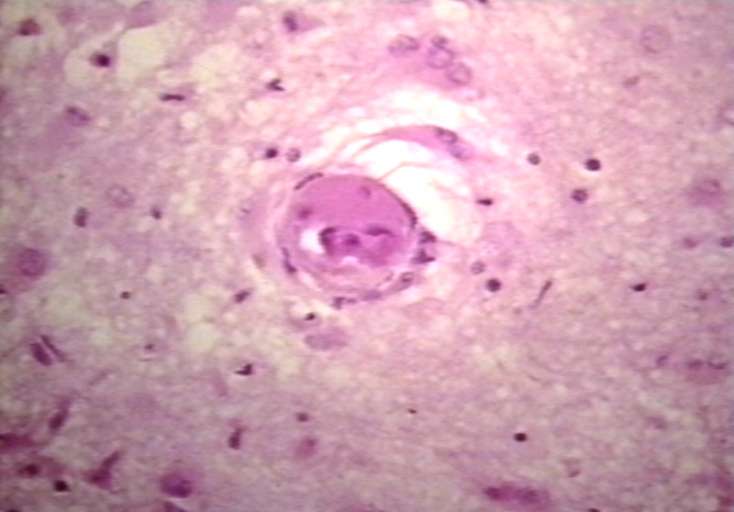
Brain: Lupus Erythematosus, Systemic; Microinfarct in Cerebral Cortex
-
Vessel: lupus, systemic erythematosus; Thrombus in capillary
-
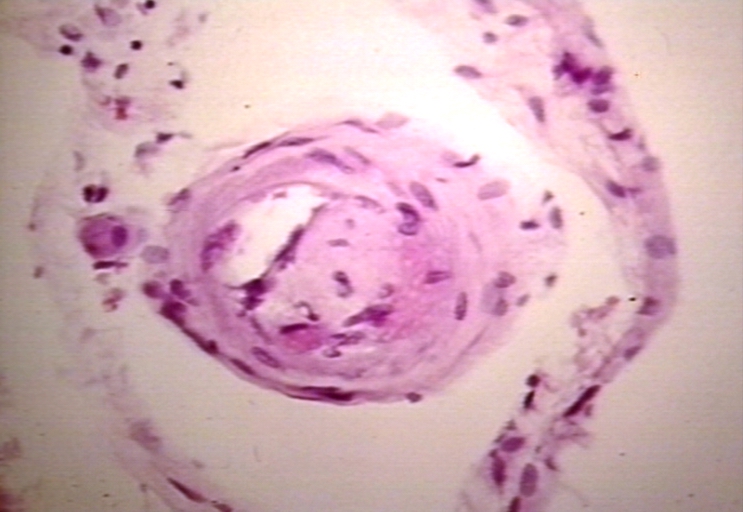
Vessel: lupus, systemic erythematosus; Thrombus in capillary
-
Vessel: lupus, systemic erythematosus; Thrombus in arteriole and vein
-
Vessel: lupus, systemic erythematosus; Thrombus in pial vessel
-

Skin: Lupus, systemic erythematosus; Discoid skin lesion in patient with SLE
-

Skin: ulcer, necrotic; lupus anticoagulant in thigh
-
Skin: lupus, erythematosus, subacute; Papulosquamous diseases
-

Skin: lupus, erythematosus; Papulosquamous diseases
-

Skin: lupus, erythematosus; papulosquamous diseases
-
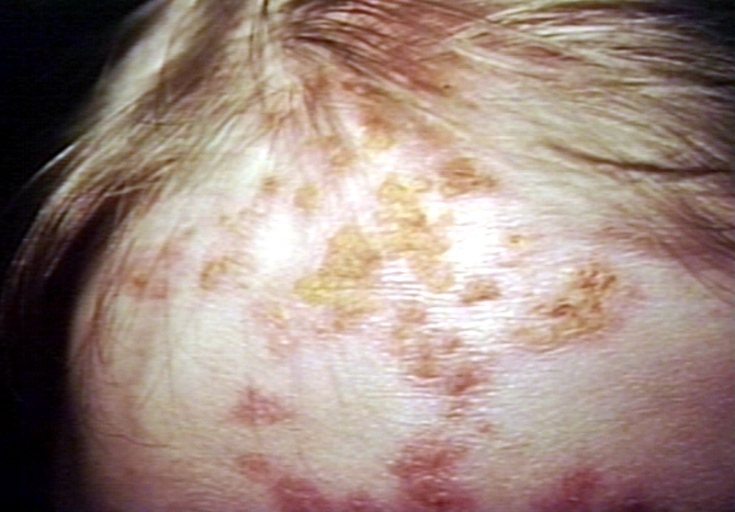
Skin: alopecia, secondary lupus erythematosus; hair loss
-

Skin: discoid lupus, face


























































Videos
<youtube v=Tw07BFaDEo0/>
See also
- Abzyme
- Anti-nuclear antibody
- Discoid lupus erythematosus in dogs
- Lupus Canada
- Lupus Foundation of America
References
- ↑ "LUPUS FOUNDATION OF AMERICA". Retrieved 2007-07-04.
- ↑ "LUPUS FOUNDATION OF AMERICA". Retrieved 2007-07-04.
- ↑ "LUPUS FOUNDATION OF AMERICA". Retrieved 2007-07-04.
- ↑ Lupus and African-American women
- ↑ 5.0 5.1 5.2 DiGeronimo, Theresa. New Hope for People with Lupus. Prima Publishing. 2002.
- ↑ James, William; Berger, Timothy; Elston, Dirk (2005). Andrews' Diseases of the Skin: Clinical Dermatology. (10th ed.). Saunders. Chapter 8. ISBN 0721629210.
- ↑ Discoid Lupus Erythematosus
- ↑ 8.0 8.1 8.2 8.3 8.4 "Handout on Health: Systemic Lupus Erythematosus". The National Institute of Arthritis and Musculoskeletal and Skin Diseases. National Institutes of Health. 2003. Retrieved 2007-11-23. Unknown parameter
|month=ignored (help) - ↑ University of South Carolina lecture on immunology
- ↑ 10.0 10.1 10.2 Anisur Rahman and David A. Isenberg (February 28, 2008). "Review Article: Systemic Lupus Erythematosus". N Engl J Med. 358 (9): 929–939. doi:10.1056/NEJMra071297. PMID 18305268.
- ↑ Mary K. Crow (February 28, 2008). "Collaboration, Genetic Associations, and Lupus Erythematosus". N Engl J Med. 358 (9): 956–961. doi:10.1056/NEJMe0800096. PMID 18204099.
- ↑ Geoffrey Hom, Robert R. Graham, Barmak Modrek; et al. (February 28, 2008). "Association of Systemic Lupus Erythematosus with C8orf13–BLK and ITGAM–ITGAX". N Engl J Med. 358 (9): 900–909. doi:10.1056/NEJMoa0707865. PMID 18204098.
- ↑ University of South Carolina School of Medicine lecture notes, Immunology, Hypersensitivity reactions. General discussion of hypersensitivity, not specific to SLE.
- ↑ Gaipl, U S; Kuhn, A; Sheriff, A; Munoz, L E; Franz, S; Voll, R E; Kalden, J R; Herrmann, M (2006). "Clearance of apoptotic cells in human SLE". Current directions in autoimmunity. 9: 173–87. PMID: 1639466 Abstract (full text requires registration).
- ↑ Poole BD, Schneider RI, Guthridge JM; et al. (2009). "Early targets of nuclear RNP humoral autoimmunity in human systemic lupus erythematosus". Arthritis Rheum. 60 (3): 848–859. doi:10.1002/art.24306. PMID 19248110. Unknown parameter
|month=ignored (help) - ↑ Pan HF, Wu GC, Li WP, Li XP, Ye DQ (2009). "High Mobility Group Box 1: a potential therapeutic target for systemic lupus erythematosus". Mol. Biol. Rep. doi:10.1007/s11033-009-9485-7. PMID 19247800. Unknown parameter
|month=ignored (help) - ↑ Lupus: The Great Imitator
- ↑ Yu Asanuma, M.D., Ph.D., Annette Oeser, B.S., Ayumi K. Shintani, Ph.D., M.P.H., Elizabeth Turner, M.D., Nancy Olsen, M.D., Sergio Fazio, M.D., Ph.D., MacRae F. Linton, M.D., Paolo Raggi, M.D., and C. Michael Stein, M.D. (2003). "Premature coronary-artery atherosclerosis in systemic lupus erythematosus". New England Journal of Medicine. 349 (Dec. 18): 2407–2414. PMID 14681506 Abstract (full text requires registration).
- ↑ Bevra Hannahs Hahn, M.D. (2003). "Systemic lupus erythematosus and accelerated atherosclerosis". New England Journal of Medicine. 349 (Dec. 18): 2379–2380. PMID 14681501 Extract (full text requires registration).
- ↑ Mary J. Roman, M.D., Beth-Ann Shanker, A.B., Adrienne Davis, A.B., Michael D. Lockshin, M.D., Lisa Sammaritano, M.D., Ronit Simantov, M.D., Mary K. Crow, M.D., Joseph E. Schwartz, Ph.D., Stephen A. Paget, M.D., Richard B. Devereux, M.D., and Jane E. Salmon, M.D. (2003). "Prevalence and correlates of accelerated atherosclerosis in systemic lupus erythematosus". New England Journal of Medicine. 349 (Dec. 18): 2399–2406. PMID 14681505 Abstract (full text requires registration).
- ↑ "General Pathology Images for Immunopathology". Retrieved 2007-07-24.
- ↑ Buyon JP, Clancy RM (2003). "Maternal autoantibodies and congenital heart block: mediators, markers, and therapeutic approach". Semin. Arthritis Rheum. 33 (3): 140–54. PMID 14671725. Unknown parameter
|month=ignored (help) - ↑ Iizuka N, Okamoto K, Hirohata S, Kato T (2009). "[Analysis of autoantigens in patients with systemic lupus erythematosus by using proteomic approach]". Nihon Rinsho Meneki Gakkai Kaishi (in Japanese). 32 (1): 43–7. PMID 19252377. Unknown parameter
|month=ignored (help) - ↑ NIM encyclopedic article on the LE cell test
- ↑ NIM encyclopedic article on the LE cell test
- ↑ Rheumatology.org article on the classification of rheumatic diseases
- ↑ Revision of Rheumatology.org's diagnostic criteria
- ↑ 28.00 28.01 28.02 28.03 28.04 28.05 28.06 28.07 28.08 28.09 28.10 Edworthy SM, Zatarain E, McShane DJ, Bloch DA (1988). "Analysis of the 1982 ARA lupus criteria data set by recursive partitioning methodology: new insights into the relative merit of individual criteria". J. Rheumatol. 15 (10): 1493–8. PMID 3060613.
- ↑ UpToDate Patient information article on DNA antibodies
- ↑ Asherson RA, Cervera R, de Groot PG; et al. (2003). "Catastrophic antiphospholipid syndrome: international consensus statement on classification criteria and treatment guidelines". Lupus. 12 (7): 530–4. PMID 12892393.
- ↑ Sangle S, D'Cruz DP, Hughes GR (2005). "Livedo reticularis and pregnancy morbidity in patients negative for antiphospholipid antibodies". Ann. Rheum. Dis. 64 (1): 147–8. doi:10.1136/ard.2004.020743. PMID 15608315.
- ↑ Hughes GR, Khamashta MA (2003). "Seronegative antiphospholipid syndrome". Ann. Rheum. Dis. 62 (12): 1127. PMID 14644846.
- ↑ Hughes GR (1998). "Is it lupus? The St. Thomas' Hospital "alternative" criteria". Clin. Exp. Rheumatol. 16 (3): 250–2. PMID 9631744.
- ↑ Merck manual discussion of Lupus
- ↑ Review of different alternative treatments for lupus
- ↑ Hospital for Special Surgery article on acupuncture and lupus
- ↑ "Light therapy (with UVA-1) for SLE patients: is it a good or bad idea? -- Pavel 45 (6): 653 -- Rheumatology". Retrieved 2007-07-04.
- ↑ Cochat P, Fargue S, Mestrallet G; et al. (2009). "Disease recurrence in paediatric renal transplantation". Pediatr. Nephrol. doi:10.1007/s00467-009-1137-6. PMID 19247694. Unknown parameter
|month=ignored (help) - ↑ Lead Discovery article on treatment of Lupus
- ↑ Foocharoen C, Nanagara R, Salang L, Suwannaroj S, Mahakkanukrauh A (2009). "Pregnancy and disease outcome in patients with systemic lupus erythematosus (SLE): a study at Srinagarind Hospital". J Med Assoc Thai. 92 (2): 167–74. PMID 19253790. Unknown parameter
|month=ignored (help) - ↑ Poor prognostic factors,Sudheer, SLE document
- ↑ [Early steroids may prevent relapses in lupus, P Jarman (Published in Journal Watch (General) July 18, 1995)
External links
Template:Diseases of the musculoskeletal system and connective tissue Template:Vesiculobullous disease
bg:Лупус ca:Lupus eritematós sistèmic da:Systemisk Lupus Erythematosus de:Lupus erythematodes fa:لوپوس منتشر id:Lupus eritematosus sistemik it:Lupus eritematoso sistemico he:זאבת ms:Lupus eritematosus sistemik nl:Lupus erythematodes simple:Lupus erythematosus fi:Sle sv:Systemisk lupus erythematosus th:โรคลูปัส