Ventricular arrhythmias: Difference between revisions
| Line 157: | Line 157: | ||
=== Exercise Testing Recommendations === | === Exercise Testing Recommendations === | ||
Class I | |||
1. Exercise testing is recommended in adult patients | |||
with ventricular arrhythmias who have an intermediate | |||
or greater probability of having CHD by age, | |||
gender, and symptoms* to provoke ischemic changes | |||
or ventricular arrhythmias. (Level of Evidence: B) *See | |||
Table 4 in the ACC/AHA 2002 Guideline Update for | |||
Exercise Testing (141) for further explanation of CHD | |||
probability. | |||
2. Exercise testing, regardless of age, is useful in patients | |||
with known or suspected exercise-induced ventricular | |||
arrhythmias, including catecholaminergic | |||
VT, to provoke the arrhythmia, achieve a diagnosis, | |||
and determine the patient’s response to tachycardia. | |||
(Level of Evidence: B) | |||
==Resources== | ==Resources== | ||
Revision as of 17:04, 1 October 2012
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor: Cafer Zorkun, M.D., Ph.D. [2]
Causes of Ventricular Arrhythmias
Cardiac causes
Acute and chronic ischemic heart disease
Noncardiac causes
Stimulants: caffeine, cocaine, alcohol
Metabolic abnormalities: acidosis, hypoxemia, hyperkalemia, hypokalemia, hypomagnesemia
Drugs: digoxin (Lanoxin), theophylline, antipsychotics, tricyclic antidepressants, antiarrhythmics with proarrhythmic potential [e.g., flecainide (Tambocor), dofetilide (Tikosyn), sotalol (Betapace) and quinidine)
| example | regularity | atrial frequency | ventricular frequency | origin (SVT/VT) | p-wave | effect of adenosine | |
|---|---|---|---|---|---|---|---|
| Wide complex (QRS>0.12) | |||||||
| Ventricular Tachycardia | regular (mostly) | 60-100 bpm | 110-250 bpm | ventricle (VT) | AV-dissociation | no rate reduction (sometimes accelerates) | |
| Ventricular Fibrillation | irregular | 60-100 bpm | 400-600 bpm | ventricle (VT) | AV-dissociation | none | |
| Ventricular Flutter | regular | 60-100 bpm | 150-300 bpm | ventricle (VT) | AV-dissociation | none | |
| Accelerated Idioventricular Rhythm | regular (mostly) | 60-100 bpm | 50-110 bpm | ventricle (VT) | AV-dissociation | no rate reduction (sometimes accelerates) | |
| Torsade de Pointes | regular | 150-300 bpm | ventricle (VT) | AV-dissociation | no rate reduction (sometimes accelerates) | ||
| Bundle-branch re-entrant tachycardia* | regular | 60-100 bpm | 150-300 bpm | ventricles (VT) | AV-dissociation | no rate reduction | |
| (*) Bundle-branch re-entrant tachycardia is extremely rare | |||||||
{kind=link}
Premature Ventricular Complexes (PVCs)
A premature ventricular complex is characterized by the premature occurrence of a QRS complex that is bizarre in shape and lasts longer than 120 msec. The T wave is large and usually of opposite polarity to the QRS complex.
A premature ventricular complex is usually followed by a full compensatory pause. The term “ventricular bigeminy” refers to alternating normal sinus and premature ventricular complexes. Three or more successive premature ventricular complexes are arbitrarily defined as ventricular tachycardia. Premature ventricular complexes become more prevalent with increasing age and occur in association with a variety of stimuli.
It is important to determine whether underlying structural heart disease is present and left ventricular function is impaired.Other common causes include electrolyte abnormalities, stimulants, and some medications.
Management
Patients Without Heart Disease
In the absence of heart disease, PVCs are associated with little or no increased risk of developing a dangerous arrhythmia. In this situation, the risk-to-benefit ratio of antiarrhythmic drug therapy does not support routine treatment.[1] It is important to review medications, determine if stimulants are being used, and correct electrolyte abnormalities. If no underlying cause is found, the optimal approach is patient reassurance. Patients should be made aware of the potential dangers of antiarrhythmic drug therapy as determined in the Cardiac Arrhythmia Suppression Trials (CAST and CAST II).[2] [3]
CAST showed that the risk of dying increased, rather than decreased, with successful long-term suppression of premature ventricular complexes after myocardial infarction in older patients. At best, CAST II showed no impact on long-term survival from drug treatment that successfully suppressed premature ventricular complexes. If patients with multiple premature ventricular complexes have severe, disabling symptoms, beta blockers are the safest initial choice.Referral to a cardiologist is indicated if beta-blocker therapy is not effective. In this situation, the next agents to be tried would be class I antiarrhythmic drugs, such as flecainide (Tambocor) and amiodarone (Cordarone), although radiofrequency ablation of an ectopic focus may also be an appropriate treatment.
Patients with Structural Heart Disease
The occurrence of premature ventricular complexes in patients with structural heart disease has been shown to significantly increase the risk of subsequent morbidity and mortality. Coronary heart disease, cardiomyopathy, and congestive heart failure are the major cardiac diseases associated with unfavorable outcomes in patients with premature ventricular complexes.
Ventricular Tachycardia
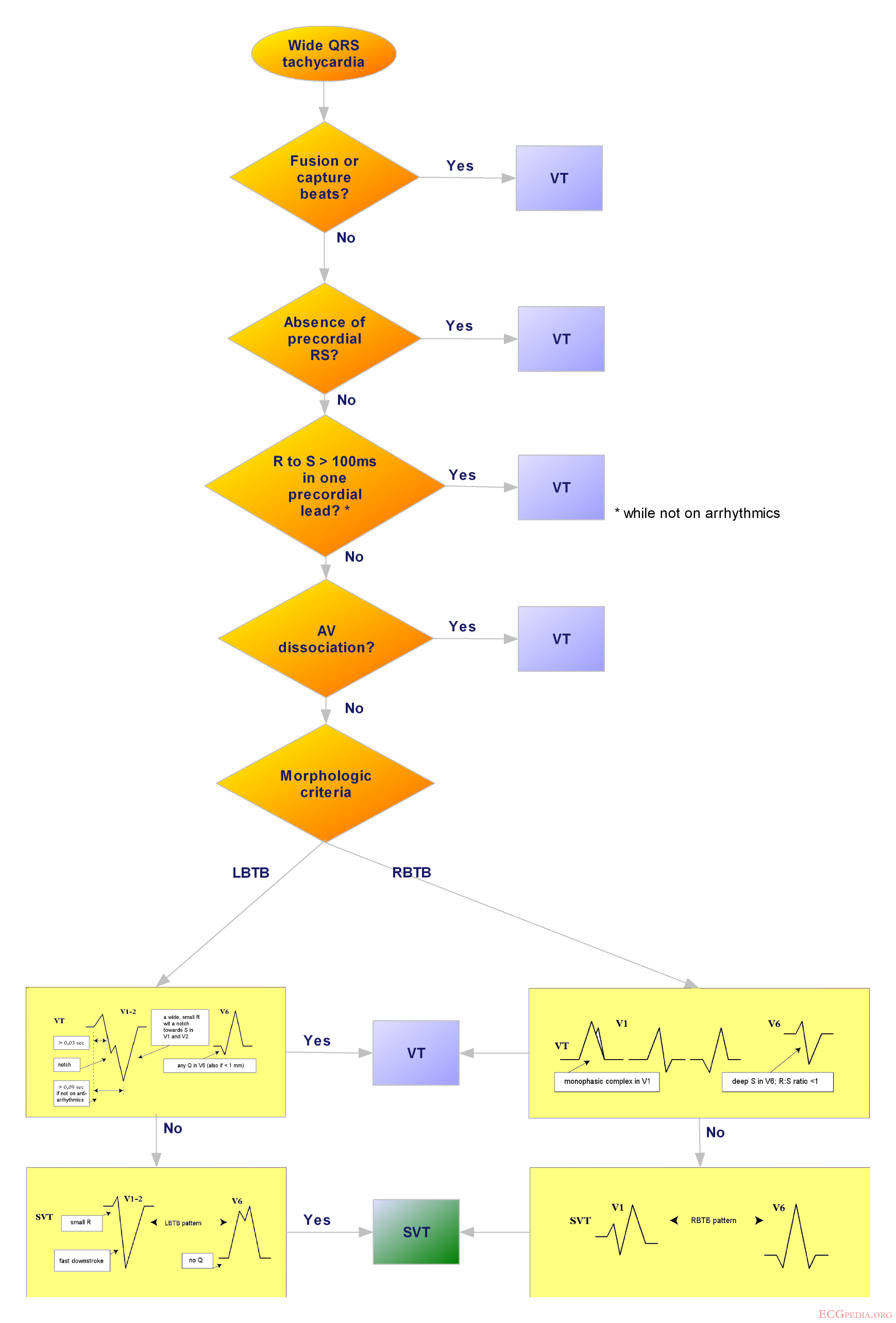
Ventricular tachycardia refers to a rhythm originating from a ventricular ectopic focus at a rate >100 bpm. The electrocardiogram shows a wide complex tachycardia with no associated P waves.
In patients with bundle branch block,Wolff-Parkinson-White syndrome, or aberrant conduction, supraventricular tachycardia can resemble ventricular tachycardia. Because of the morbidity and mortality associated with untreated ventricular tachycardia, any wide-complex tachycardia should be assumed to be ventricular tachycardia until proved otherwise. Physicians should keep in mind that patients with ventricular tachycardia can have minimal symptoms.
Management of Ventricular Tachycardia
The mortality rate within two years is reported to be higher than 30% in patients with non sustained ventricular tachycardia on Holter monitoring and impaired left ventricular function.[4] Two large multicenter trials [5] [6] showed a clear advantage for automatic cardioverter defibrillator implantation over drug therapy in patients who had a malignant ventricular arrhythmia or who had been resuscitated from sudden cardiac death. The selection of high-risk patients for defibrillator implantation should be based on left ventricular function and the findings of electrophysiologic studies.
Implantable defibrillators appear to be most beneficial in patients with a low ejection fraction who are noted to have frequent premature ventricular complexes, non sustained ventricular tachycardia on Holter monitoring, and a history of syncope or nearsyncope. It is critical to rule out coronary heart disease and to optimize the treatment of congestive heart failure in these patients. When ventricular tachycardia is diagnosed in relatively asymptomatic patients, medical treatment should be attempted. New recommendations from the American Heart Association [7] emphasize the initial use of 300 mg of iv. administered amiodarone, followed by repeated 150 mg iv. doses every 8-10 minutes, in patients with pulseless VT.
Patients with stable ventricular tachycardia should be given 150 mg of amiodarone intravenously over 10 minutes, followed by an infusion at 1 mg/minute for 6 hours and then at 0.5 mg/minute until the VT converts to sinus rhythm or another less dangerous rhythm. The alternative treatment is intravenously administered lidocaine (Xylocaine), given first in a 100 mg bolus (or 1 mg/kg) and then in an infusion at 1-4 mg/minute.
In hemodynamically unstable patients, electrical cardioversion should be attempted in accordance with the recently revised advanced cardiac life support (ACLS) protocols.
Automatic implantable cardioverter defibrillators (ICD) are considered the most effective treatment for patients with life-threatening VT or VF. According to expert recommendations, implantation of an automatic cardioverter defibrillator should be considered in these situations[8]:
1. Cardiac arrest resulting from ventricular fibrillation or tachycardia not caused by a transient or reversible cause
2. Spontaneous, sustained ventricular tachycardia
3. Syncope of undetermined origin and sustained VT or ventricular fibrillation (VF) induced during electrophysiologic studies
4. Non sustained VT with coronary artery disease and LV dysfunction if VT or VF is induced during electrophysiologic studies.
ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias (DO NOT EDIT)[9]
Resting Electrocardiogram Recommendations
| “ |
Class IResting 12-lead ECG is indicated in all patients who are evaluated for ventricular arrhythmias. (Level of Evidence: A). |
” |
Exercise Testing Recommendations
Class I 1. Exercise testing is recommended in adult patients with ventricular arrhythmias who have an intermediate or greater probability of having CHD by age, gender, and symptoms* to provoke ischemic changes or ventricular arrhythmias. (Level of Evidence: B) *See Table 4 in the ACC/AHA 2002 Guideline Update for Exercise Testing (141) for further explanation of CHD probability. 2. Exercise testing, regardless of age, is useful in patients with known or suspected exercise-induced ventricular arrhythmias, including catecholaminergic VT, to provoke the arrhythmia, achieve a diagnosis, and determine the patient’s response to tachycardia. (Level of Evidence: B)
Resources
1. Zipes DP, Camm AJ, Borggrefe M, et al., ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death A Report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death)Circulation 2006;114;e385-e484
2. Kesh Hebbar A, Hueston WJ, Management of Common Arrhythmias: Part II.Ventricular Arrhythmias and Arrhythmias in Special Populations Am Fam Physician 2002;65:2491-6.
References
- ↑ Kennedy HL, Whitlock JA, Sprague MK, Kennedy LJ, Buckingham TA, Goldberg RJ. Long-term follow-up of asymptomatic healthy subjects with frequent and complex ventricular ectopy. N Engl J Med 1985;312:193-7.
- ↑ Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH, et al. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. N Engl J Med 1991;324:781-8
- ↑ Effect of the antiarrhythmic agent moricizine on survival after myocardial infarction. The Cardiac Arrhythmia Suppression Trial II Investigators. N Engl J Med 1992;327:227-33.
- ↑ Wilber DJ, Garan H, Finkelstein D, Kelly E, Newell J, McGovern B, et al. Out-of-hospital cardiac arrest. Use of electrophysiologic testing in the prediction of long-term outcome. N Engl J Med 1988;318:19-24.
- ↑ Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators. N Engl J Med 1996;335:1933-40.
- ↑ A comparison of antiarrhythmic drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. The Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. N Engl J Med 1997;337:1576-83.
- ↑ Gazmuri RJ, Nadkarni VM, Nolan JP et al., Scientific Knowledge Gaps and Clinical Research Priorities for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Identified During the 2005 International Consensus Conference on E and CPR Science With Treatment Recommendations A Consensus Statement From the International Liaison Committee on Resuscitation (American Heart Association, Australian Resuscitation Council, European Resuscitation Council, Heart and Stroke Foundation of Canada, Inter American Heart Foundation, Resuscitation Council of Southern Africa, and the New Zealand Resuscitation Council); the American Heart Association Emergency Cardiovascular Care Committee; the Stroke Council; and the Cardiovascular Nursing Council. Circulation 2007 http://circ.ahajournals.org/cgi/content/full/116/21/2501
- ↑ Gregoratos G, Cheitlin MD, Conill A, Epstein AE, Fellows C, Ferguson TB Jr, et al. ACC/AHA guidelines for implantation of cardiac pacemakers and antiarrhythmia devices: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Pacemaker Implantation). Circulation 1998;97:1325-35.
- ↑ Zipes DP, Camm AJ, Borggrefe M, Buxton AE, Chaitman B, Fromer M; et al. (2006). "ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society". Circulation. 114 (10): e385–484. doi:10.1161/CIRCULATIONAHA.106.178233. PMID 16935995.