Atypical AV nodal reentrant tachycardia
Jump to navigation
Jump to search
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
- Main article: AVNRT
Criteria
- VA > 100 in HRA
- Earliest a is concentric and must have one or more
- AV block during tachycardia
- AV dissociation with rapid ventricular pacing at 200-250 ms during tachycardia
- Delta AH Interval > 40 ms
- Delta HA Interval > -10 ms
- Ventricular Overdrive Maneuver]] results in PPI-TCL > 115 for Atypical AVNRT
- Stimulus to A Maneuver SA - VA interval > 85 for Atypical AVNRT
- Same atrial activation during tachycardia and during pacing
- May have continuation of Tachycardia during AV block
- Advancement of the His with advancement or delay in the a is AVNRT
Characteristics
- Typically do not see a jump because of concealed conduction into the slow pathway.
- VPDs can induce as frequently as APDs
- Evidence of dual AVN conduction
- No evidence of an AP
Location of Earliest Atrial Activation
- Earliest retrograde atrial activation traditionally has been reported at the base of the triangle of Koch, near the CS ostium. However, mapping of retrograde atrial activation in several series of patients has produced variable results.
- In a series of 46 patients with atypical AVNRT reported by Hwang et al earliest atrial activation at the CS (ostial or lateral electrodes) was seen in 34% patients.
- In a series reported by Chen et al only 14.3% of patients with atypical AVNRT had earliest activation at the CS electrodes.
- In a series of 12 patients, Nawata et al identified six patients with earliest atrial activation at the CS ostium, three patients with earlier activation at the low right atrial septum, and three patients with simultaneous activation of the CS and right atrial septum.
- Nam et al observed eccentric atrial activation, 10 to 20 mm distal to the CS ostium, in 8 of 10 patients with fast-slow AVNRT. The CS ostium was the site of earliest atrial activation in only two patients.
- In the slow-slow form, earliest atrial activation usually occurs at the CS ostium, but variants of left lateral retrograde activation have been reported.
Maneuvers
- Use Ventricular Overdrive Maneuver or Stimulus to a maneuver to differentiate between atypical AVNRT and septal bypass tract
- Calculate Delta AH Interval
- Give Adenosine during Ventricular pacing to check for VA conduction
Differential of Atypical AVNRT from AVRT
Approximately 6% of cases of AVNRT are associated with eccentric atrial activation, with the shortest VA > 60 msec. The keys to diagnosis of an atypical AVNRT are:
- Inability to advance the atrium without a PVC on His Maneuver
- The ability to dissociate the atrium from the ventricle during Tachycardia
- Demonstration of only decremental VA conduction
- Demonstration of Dual AV Nodal Physiology
- The Ability to induce typical AVNRT with concentric or variable patterns of retrograde atrial activation
- Absence of VA conduction without Isuprel
EKG Findings
-
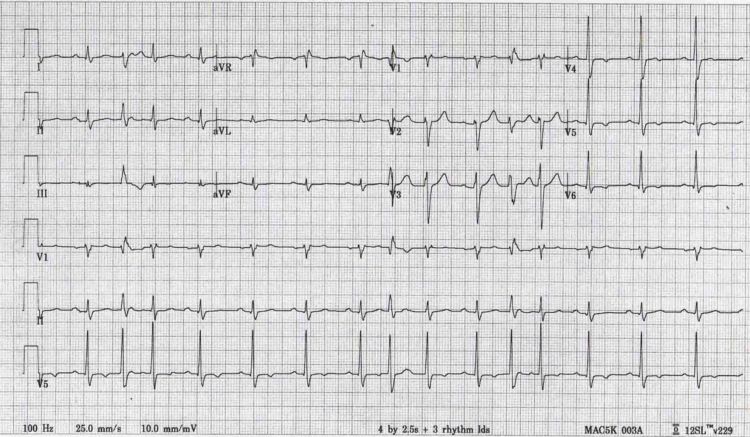 This is an extremely rare tachycardia which occurs when a single sinus impulse conducts down an AV node with both a slow and fast pathway. When most impulses reach the AV node they conduct down both the slow and fast pathway. Since conduction is faster down the fast pathway it beats out the slow pathway conduction and depolarizes the ventricle. The impulse traveling down the slow pathway either collides with the impulse from the fast pathway that is now traveling back up the slow or the impulse traveling down the slow pathway reaches the ventricle and finds the ventricle refractory. In the above EKG the sinus impulse represented by the P wave in the beginning of the rhythm strip conducts down the fast pathway resulting in the first QRS complex; the impulse from the slow pathway also depolarizes the ventricle seen as the second QRS complex. You will notice that there is no p wave between the first and second QRS complexes. Therefore the first sinus beat results in a doubling of the ventricular sinus rate. This sequence is repeated again in the 7th and 8th QRS complex. It is an extremely rare tachycardia and is resistant to multiple antiarrhythmic medications. The above patient underwent ablation of their slow pathway and no further episodes were observed.
This is an extremely rare tachycardia which occurs when a single sinus impulse conducts down an AV node with both a slow and fast pathway. When most impulses reach the AV node they conduct down both the slow and fast pathway. Since conduction is faster down the fast pathway it beats out the slow pathway conduction and depolarizes the ventricle. The impulse traveling down the slow pathway either collides with the impulse from the fast pathway that is now traveling back up the slow or the impulse traveling down the slow pathway reaches the ventricle and finds the ventricle refractory. In the above EKG the sinus impulse represented by the P wave in the beginning of the rhythm strip conducts down the fast pathway resulting in the first QRS complex; the impulse from the slow pathway also depolarizes the ventricle seen as the second QRS complex. You will notice that there is no p wave between the first and second QRS complexes. Therefore the first sinus beat results in a doubling of the ventricular sinus rate. This sequence is repeated again in the 7th and 8th QRS complex. It is an extremely rare tachycardia and is resistant to multiple antiarrhythmic medications. The above patient underwent ablation of their slow pathway and no further episodes were observed.

References
- Nam G-B, Rhee K-S, Kim J, Choi K-J, Kim Y-H. Left atrionodal connections in typical and atypical atrioventricular nodal re-entrant tachycardias: activation sequence in the coronary sinus and results of radiofrequency catheter ablation. J Cardiovasc Electrophysiol 2006;17:1–7.
- Hwang C, Martin DJ, Goodman JS, Gang ES, Mandel WJ, Swerdlow CD, Peter CT, Chen PS. Atypical atrioventricular node reciprocating tachycardia masquerading as tachycardia using a left-sided accessory pathway. J Am Coll Cardiol 1997;30:218 –225.
- Nawata H, Yamamoto N, Hirao K, Miyasaka N, Kawara T, Hiejima K, Harada T, Suzuki F. Heterogeneity of anterograde fast-pathway and retrograde slowpathway conduction patterns in patients with the fast-slow form of atrioventricular nodal reentrant tachycardia: electrophysiologic and electrocardiographic considerations. J Am Coll Cardiol 1998;32:1731–1740.
- Goldberger J, Brooks R, Kadish A. Physiology of “atypical” atrioventricular junctional reentrant tachycardia occurring following radiofrequency catheter modification of the atrioventricular node. Pacing Clin Electrophysiol 1992;15:2270–2282.
- Owada S, Iwasa A, Sasaki S, Higuma T, Kimura M, Kobayashi T, Ashikaga K, Okumura K. “V-H-A pattern” as a criterion for the differential diagnosis of atypical AV nodal reentrant tachycardia from AV reciprocating tachycardia. Pacing Clin Electrophysiol 2005;28:667– 674.
- McGuire MA, Yip AS, Lau KC, Lo CW, Richards DA, Uther JB, Ross DL. Posterior (“atypical”) atrioventricular junctional reentrant tachycardia. Am J Cardiol 1994;73:469–477.
- Sakabe K, Wakatsuki T, Fujinaga H, Oishi Y, Ikata J, Toyoshima T, Hiura N, Nishikado A, Oki T, Ito S. Patient with atrioventricular node reentrant tachycardia with eccentric retrograde left-sided activation: treatment with radiofrequency catheter ablation. Jpn Heart J 2000;41:227–234.
- Vijayaraman P, Kok LC, Rhee B, Ellenbogen KA. Unusual variant of atrioventricular nodal re-entrant tachycardia. Heart Rhythm 2004;2:100 –102.