Meningitis
Template:DiseaseDisorder infobox
|
WikiDoc Resources for Meningitis |
|
Articles |
|---|
|
Most recent articles on Meningitis |
|
Media |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Meningitis at Clinical Trials.gov Clinical Trials on Meningitis at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Meningitis
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Meningitis Discussion groups on Meningitis Patient Handouts on Meningitis Directions to Hospitals Treating Meningitis Risk calculators and risk factors for Meningitis
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Meningitis |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
Meningitis is the inflammation of the protective membranes covering the central nervous system, known collectively as the meninges (the leptomeninges and underlying subarachnoid cerebrospinal fluid). Meningitis may develop in response to a number of causes, including infectious agents (bacteria, viruses, fungi, or other organisms), physical injury, cancer, or certain drugs. While some forms of meningitis are mild and resolve on their own, meningitis is a potentially serious condition owing to the proximity of the inflammation to the brain and spinal cord. The potential for serious neurologic damage or even death necessitates prompt medical attention and evaluation. Infectious meningitis, the most common form, is typically treated with antibiotics and close observation. [1] [2] [3] [4] [5] [6]
History
Meningitis may have been described in the Middle Ages, but it was first accurately identified by the Swiss Vieusseux (a scientific-literary association) during an outbreak in Geneva, Switzerland in 1805.
In the 19th century, meningitis was a scourge of the Japanese imperial family, playing the largest role in the horrendous pre-maturity death rate the family endured. In the mid-1800s, only the Emperor Kōmei and two of his siblings reached maturity out of fifteen total children surviving birth. Kōmei's son, the Emperor Meiji, was one of two survivors out of Kōmei's six children, including an elder brother of Meiji who would have taken the throne had he lived to maturity. Five of Meiji's 15 children survived, including only his third son, Emperor Taishō, who was feeble-minded, perhaps as a result of having contracted meningitis himself. By Emperor Hirohito's generation the family was receiving modern medical attention. As the focal point of tradition in Japan, during the Tokugawa Shogunate the family was denied modern "Dutch" medical treatment then in use among the upper caste; despite extensive modernization during the Meiji Restoration the Emperor insisted on traditional medical care for his children.
Epidemiology

Meningitis refers to the inflammation arachnoid matter, the sub-arachnoid space and the cerebrospinal fluid (CSF, including the ventricles). Meningitis can affect anyone in any age group, from the newborn to the elderly.
From its recognition in 1805 until the early 20th century, bacterial meningitis was virtually uniformly fatal. Until recent years, up to 50% of patients who survived the acute infection would be left with permanent sequelae such as mental retardation and hearing loss. Over the past several years, there has been a striking shift in the demography of meningitis.
- In 1986, the median age of a patient with meningitis was 15 months, as compared with 25 years in 1995.
- Before the widespread use of the conjugated Haemophilus influenzae type B (HIB) vaccine in 1990, H. influenzae type b meningitis developed in nearly 1 in 200 children < 5 years old, and almost 70% of the cases of meningitis in children < 5 were due to H influenzae.
- It was necessary to conjugate the H. influenzae type b polysaccharide to a carrier protein in order to make a T-cell dependant antigen that could induce an immune response in infants.
- In the study by Schuchat et.al. in 1995, H. influenzae only accounted for 7% of cases.
- The case-fatality rate varied significantly amongst the different organisms, and the pathogenic organisms responsible for disease varied greatly with age.
- Group B Streptococcus agalactiae (S. agalactiae) was the main cause of meningitis in infants < 1 month with Listeria accounting for ~ 20% of cases.
- In infants 1 month – 23 month of age, Streptococcus pneumoniae (S. pneumoniae) and Neisseria meningitidis (N. meningitidis) caused 45% and 31% of the cases, respectively.
- In the 2 – 18 year old age group, N. meningitidis caused 59% of the cases, and in people 19 – 59 years old S. pneumoniae caused 62% of the cases.
- Nosocomial infections with Gram-negative bacilli are becoming increasingly important as well.
The "Meningitis Belt" is an area in sub-Saharan Africa which stretches from Senegal in the west to Ethiopia in the east in which large epidemics of meningococcal meningitis occur (this largely coincides with the Sahel region). It contains an estimated total population of 300 million people. The largest epidemic outbreak was in 1996, when over 250,000 cases occurred and 25,000 people died as a consequence of the disease.
Pathophysiology & Etiology
The clinical picture of meningitis largely arises from the host response to the inciting organism in the CSF.
- It seems that the subcapsular components (the cell wall and lipopolysaccharide) of bacteria are more important in determining inflammation than the surface components (pili and polysaccharide capsule).
- The primary site of breakdown of the blood-brain barrier is the cerebral microvascular endothelium.
- Electron microscope (EM) studies have shown complete separation of the intercellular tight junctions
- It appears that there is a final common pathway, mediated by TNF-alpha, IL-1 and IL-6, that results in meningeal inflammation and loss of the blood-brain barrier.
- One of the major roles of these cytokines is to facilitate the migration of neutrophils across the vascular endothelium into the CSF.
- A key initial step in this process is obviously adhesion of the PMN to the endothelial surface.
- This is mediated by the expression of specific transmembrane glycoproteins expressed on the endothelial surface that interact with specific counterparts on the neutrophils.
- These adhesion molecules fall into three large categories: the immunoglobin superfamily (including the antigen-specific T and B cell receptors, ICAM-1 and ICAM-2), the integrin family (beta-1, beta-2, and beta-3) and the selectin family (including ELAM-1).
- The interaction of beta-2 integrin (CD18) and ICAM-1 is largely responsible for PMN diapedesis.
- Additionally, patients get cerebral edema that is mediated by an increase in capillary permeability, the inflammatory response from the neutrophils, and CSF outflow resistance.
- The above pathophysiologic processes are not only important in producing the symptoms associated with meningitis, but the understanding of the underlying disease process is necessary to guide therapy (see below).
Mechanism
- In order to gain access to the CNS, the pathogen needs to colonize mucosal epithelium, invade and survive in the intravascular space, cross the blood-brain barrier and survive in the CSF.
- Colonization of the nasopharynx is usually asymptomatic, and during peak seasons, approximately 20% of the population are colonized with N. meningitidis.
Causes
Most cases of meningitis are caused by microorganisms, such as viruses, bacteria, fungi, or parasites, that spread into the blood and into the cerebrospinal fluid (CSF).[7] Non-infectious causes include cancers, systemic lupus erythematosus and certain drugs. The most common cause of meningitis is viral, and often runs its course within a few days. Bacterial meningitis is the second most frequent type and can be serious and life-threatening. Numerous microorganisms may cause bacterial meningitis, but Neisseria meningitidis ("meningococcus") and Streptococcus pneumoniae ("pneumococcus") are the most common pathogens in patients without immune deficiency, with meningococcal disease being more common in children. Staphylococcus aureus may complicate neurosurgical operations, and Listeria monocytogenes is associated with poor nutritional state and alcoholicism. Haemophilus influenzae (type B) incidence has been much reduced by immunization in many countries. Mycobacterium tuberculosis (the causative agent of tuberculosis) rarely causes meningitis in Western countries but is common and feared in countries where tuberculosis is endemic.
Diagnosis
History and Symptoms
In the study by Durand et.al., only 2/3 of patients had the classic triad of fever, nuchal rigidity and change in mental status.
- All patients, however, had at least one of these findings.
- 95% had fever >100 degrees Fahrenheit, with a mean duration of 4 days.
- Neck stiffness was present in 88%, and contrary to other reports, was not significantly lower amongst the elderly.
- Kernig's sign: inability to allow full extension of the knee when the hip is flexed 90 degrees.
- Brudzinski’s sign: spontaneous flexion of the hips during attempted passive neck flexion.
- 11% of patients had a rash, and of these cases 73% of them were due to Neisseria meningitidis (most commonly petechiae and purpura)
- 78% of patients had an abnormal mental status, primarily lethargy and confusion.
- 23% of the patients had focal seizures.
In general:
Headache is the most common symptom of meningitis (87%) followed by nuchal rigidity ("neck stiffness", 83%). The classic triad of diagnostic signs consists of nuchal rigidity (being unable to flex the neck forward), fever and altered mental status. All three features are present in only 44% of all cases of infectious meningitis.[8] Other symptoms commonly associated with meningitis are photophobia (inability to tolerate bright light), phonophobia (inability to tolerate loud noises), irritability and delirium (in small children) and seizures (in 20-40% of cases). In infants (0-6 months), swelling of the fontanelle (soft spot) may be present. Vomiting may be present.
Physical Examination
The suspicion of meningitis is generally based on the nature of the symptoms and findings on physical examination. Meningitis is a medical emergency, and referral to hospital is indicated. If meningitis is suspected based on clinical examination, early administration of antibiotics is recommended, as the condition may deteriorate rapidly. In the hospital setting, initial management consists of stabilization (e.g. securing the airway in a depressed level of consciousness, administration of intravenous fluids in hypotension or shock), followed by antibiotics if not already administered.
Nuchal rigidity is typically assessed with the patient lying supine, and both hips and knees flexed. If pain is elicited when the knees are passively extended (Kernig's sign), this indicates nuchal rigidity and meningitis. In infants, forward flexion of the neck may cause involuntary knee and hip flexion (Brudzinski's sign). Although commonly tested, the sensitivity and specificity of Kernig's and Brudzinski's tests are uncertain.[9]
In "meningococcal" meningitis (i.e. meningitis caused by the bacteria Neisseria meningitidis), a rapidly-spreading petechial rash is typical, and may precede other symptoms. The rash consists of numerous small, irregular purple or red spots on the trunk, lower extremities, mucous membranes, conjunctiva, and occasionally on the palms of hands and soles of feet.
Laboratory Evaluations
Investigations include blood tests (electrolytes, liver and kidney function, inflammatory markers and a complete blood count) and usually X-ray examination of the chest. The most important test in identifying or ruling out meningitis is analysis of the cerebrospinal fluid (fluid that envelops the brain and the spinal cord) through lumbar puncture (LP). However, if the patient is at risk for a cerebral mass lesion or elevated intracranial pressure (recent head injury, a known immune system problem, localizing neurological signs, or evidence on examination of a raised ICP), a lumbar puncture may be contraindicated because of the possibility of fatal brain herniation. In such cases a CT or MRI scan is generally performed prior to the lumbar puncture to exclude this possibility. Otherwise, the CT or MRI should be performed after the LP, with MRI preferred over CT due to its superiority in demonstrating areas of cerebral edema, ischemia, and meningeal inflammation.
During the lumbar puncture procedure, the opening pressure is measured. A pressure of over 180 mmH2O is indicative of bacterial meningitis.
The CSF sample is examined for white blood cells (and which subtypes), red blood cells, protein content and glucose level. Gram staining of the sample may demonstrate bacteria in bacterial meningitis, but absence of bacteria does not exclude bacterial meningitis; microbiological culture of the sample may still yield a causative organism. The type of white blood cell predominantly present predicts whether meningitis is due to bacterial or viral infection. Other tests performed on the CSF sample include latex agglutination test, limulus lysates, or polymerase chain reaction (PCR) for bacterial or viral DNA. If the patient is immunocompromised, testing the CSF for toxoplasmosis, Epstein-Barr virus, cytomegalovirus, JC virus and fungal infection may be performed.

| Condition | Glucose | Protein | Cells |
|---|---|---|---|
| Acute bacterial meningitis | Low | high | high, often > 300/mm³ |
| Acute viral meningitis | Normal | normal or high | mononuclear, < 300/mm³ |
| Tuberculous meningitis | Low | high | pleocytosis, mixed < 300/mm³ |
| Fungal meningitis | Low | high | < 300/mm³ |
| Malignant meningitis | Low | high | usually mononuclear |
| Subarachnoid haemorrhage | Normal | normal, or high | Erythrocytes |
| Cerebrospinal Fluid | |||||
| Normal Levels | Acute Bacterial M. | Acute Viral M. | TB M. | Neuroborreliosis | |
| Cells/ul | < 5 | In the 1000s | In the 100s | In the 100s | Some 100 |
| Cells | Lymph:Monos 7:3 | Gran. > Lymph. | Lymph. > Gran. | Various leukos | Lymph. monocytic |
| Total Protein (mg/dl) | 45-60 | Typically 100-500 | Typically normal | Typically 100-200 | Typically up to 350 |
| Glucose Ratio (CSF/plasma) | Typically > 0.5 | < 0.3 | > 0.6 | < 0.5 | Normal |
| Lactate (mmol/l) | < 2.1 | > 2.1 | < 2.1 | > 2.1 | - |
| Others | ICP: 6-22 (cm H2O) | PCR of HSV-DNA | PCR of TBC-DNA | IgG/IgM CSF/Serum Ratio |
In bacterial meningitis, the CSF glucose to serum glucose ratio is < 0.4. The Gram stain is positive in >60% of cases, and culture in >80%. Latex agglutination may be positive in meningitis due to Streptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae, Escherichia coli, Group B Streptococci. Limulus lysates may be positive in Gram-negative meningitis.
CSF Cultures
Cultures are often negative if CSF is taken after the administration of antibiotics. In these patients, PCR can be helpful in arriving at a diagnosis. It has been suggested that CSF cortisol measurement may be helpful.[11]
Prediction rules
The Bacterial Meningitis Score predicts reliably whether a child (older than two months) may have infectious meningitis. In children with at least 1 risk factor (positive CSF Gram stain, CSF absolute neutrophil count ≥ 1000 cell/µL, CSF protein ≥ 80 mg/dL, peripheral blood absolute neutrophil count ≥ 10,000 cell/µL, history of seizure before or at presentation time) it had a sensitivity of 100%, specificity of 63.5%, and negative predictive value of 100%.[12]
Computed Tomography
- The role of the head CT is controversial. It should obviously be preformed in all patients with suspected elevations in intracranial pressure (ICP), however this is often a difficult clinical diagnosis.
- Approximately 50% of the patients in Durand’s study with focal neuro findings had CT abnormalities, whereas CT findings were seen in only 17% of patients without focal findings on exam (p < 0.01).
- Quagliarello and Scheld recommend getting CTs only in patients who are comatose, have papilledema or who have focal neuro deficits.
Histopathology: Acute Bacterial Meningitis
<youtube v=L9jpjxTSLws/>
Complete Differential Diagnosis of Underlying Causes of Meningitis
In alphabetical order. [13] [14]
Common Causes
- Escherichia coli
- Gram-negative bacilli
- Group B streptococci
- Haemophilus influenzae
- Klebsiella pneumoniae
- Listeria monocytogenes
- Neisseria Meningitis
- Non-Group B streptococci
- Staphylococci
- Streptococcus agalactiae
- Streptococcus pneumoniae
Infectious Causes
- Abscess
- Adenovirus
- Arboviruses
- Aspergillosis
- Borrelia
- Candidiasis
- Chlamydia psittaci
- Coccidioidomycosis
- Coxsackie viruses
- Cryptococcosis
- Cysticercosis
- Cytomegalovirus
- ECHO viruses (Entero Cytopathogenic Human Orphan)
- Epstein-Barr Virus
- Escherichia coli
- Haemophilus influenzae
- Herpes Simplex Virus
- Histoplasmosis
- HIV
- Influenza
- Klebsiella pneumoniae
- Leptospira
- Listeria monocytogenes
- Malaria
- Measles
- Mumps
- Mycobacteria
- Mycoplasma pneumoniae
- Neisseria Meningitidis
- Otitis
- Pertussis
- Polio
- Proteus
- Pseudomonas
- Rabies
- Rickettsia
- Rubella
- Sarcoidosis
- Schistosomiasis
- Sinusitis
- Smallpox
- Staphylococcus aureus
- Staphylococcus epidermidis
- Streptococci
- Streptococcus agalactiae
- Streptococcus pneumoniae
- Syphilis
- Toxoplasmosis
- Tuberculosis
- Varicella-Zoster Virus
- Whipple's Disease
Noninfectious Causes
- Behcet's Syndrome
- Brain tumor
- Cerebrovascular accident
- Drugs
- Meningeal carcinomatosis
- Meningeal leukemia
- Multiple Sclerosis
- Vaccine reaction
- Triquinine
Treatment
Bacterial meningitis
Bacterial meningitis is a medical emergency and has a high mortality rate if untreated.[15] All suspected cases, however mild, need emergency medical attention. Empiric antibiotics must be started immediately, even before the results of the lumbar puncture and CSF analysis are known. Antibiotics started within 4 hours of lumbar puncture will not significantly affect lab results. Adjuvant treatment with corticosteroids reduces rates of mortality, severe hearing loss and neurological sequelae.[16]
| Age group | Causes |
|---|---|
| Neonates | Group B Streptococci, Escherichia coli, Listeria monocytogenes |
| Infants | Neisseria meningitidis, Haemophilus influenzae, Streptococcus pneumoniae |
| Children | N. meningitidis, S. pneumoniae |
| Adults | S. pneumoniae, N. meningitidis, Mycobacteria, Cryptococci |
The choice of antibiotic depends on local advice. In most of the developed world, the most common organisms involved are Streptococcus pneumoniae and Neisseria meningitidis: first line treatment in the UK is a third-generation cephalosporin (such as ceftriaxone or cefotaxime). In those under 3 years of age, over 50 years of age, or immunocompromised, ampicillin should be added to cover Listeria monocytogenes. In the U.S. and other countries with high levels of penicillin resistance, the first line choice of antibiotics is vancomycin and a carbapenem (such as meropenem). In sub-Saharan Africa, oily chloramphenicol or ceftriaxone are often used because only a single dose is needed in most cases.
Staphylococci and gram-negative bacilli are common infective agents in patients who have just had a neurosurgical procedure. Again, the choice of antibiotic depends on local patterns of infection: cefotaxime and ceftriaxone remain good choices in many situations, but ceftazidime is used when Pseudomonas aeruginosa is a problem, and intraventricular vancomycin is used for those patients with intraventricular shunts because of high rates of staphylococcal infection. In patients with intracerebral prosthetic material (metal plates, electrodes or implants, etc.) then sometimes chloramphenicol is the only antibiotic that will adequately cover infection by Staphylococcus aureus (cephalosporins and carbapenems are inadequate under these circumstances).
Once the results of the CSF analysis are known along with the Gram-stain and culture, empiric therapy may be switched to therapy targeted to the specific causative organism and its sensitivities.
- Neisseria meningitidis (Meningococcus) can usually be treated with a 7-day course of IV antibiotics:
- Penicillin-sensitive -- penicillin G or ampicillin
- Penicillin-resistant -- ceftriaxone or cefotaxime
- Prophylaxis for close contacts (contact with oral secretions) -- rifampin 600 mg bid for 2 days (adults) or 10 mg/kg bid (children). Rifampin is not recommended in pregnancy and as such, these patients should be treated with single doses of ciprofloxacin, azithromycin, or ceftriaxone
- Streptococcus pneumoniae (Pneumococcus) can usually be treated with a 2-week course of IV antibiotics:
- Penicillin-sensitive -- penicillin G
- Penicillin-intermediate -- ceftriaxone or cefotaxime
- Penicillin-resistant -- ceftriaxone or cefotaxime + vancomycin
- Listeria monocytogenes is treated with a 3-week course of IV ampicillin + gentamicin.
- Gram negative bacilli -- ceftriaxone or cefotaxime
- Pseudomonas aeruginosa -- ceftazidime
- Staphylococcus aureus
- Methicillin-sensitive -- nafcillin
- Methicillin-resistant -- vancomycin
- Streptococcus agalactiae -- penicillin G or ampicillin
- Haemophilus influenzae -- ceftriaxone or cefotaxime
Viral meningitis
Unlike bacteria, viruses cannot be killed by antibiotics. Patients with very mild viral meningitis may only have to spend a few hours in a hospital, while those who have a more serious infection may be hospitalised for many more days for supportive care. Patients with mild cases, which often cause only flu-like symptoms, may be treated with fluids, bed rest (preferably in a quiet, dark room), and analgesics for pain and fever. Serious cases, especially in the case of young children or neonates, may require the use of antiviral drugs, such as acyclovir. The physician may also prescribe anticonvulsants such as phenytoin to prevent seizures and corticosteroids to reduce brain inflammation. If inflammation is severe, pain medicine and sedatives may be prescribed to make the patient more comfortable.
Fungal meningitis
This form of meningitis is rare in otherwise healthy people, but is a higher risk in those who have AIDS, other forms of immunodeficiency (an immune system that does not respond adequately to infections) and immunosuppression (immune system malfunction as a result of medical treatment). In AIDS, Cryptococcus neoformans is the most common cause of fungal meningitis; it requires Indian ink staining of the CSF sample for identification of this capsulated yeast. Fungal meningitis is treated with long courses of highly dosed antifungals.[17]
Complications
In children there are several potential disabilities which result from damage to the nervous system. These include sensorineural hearing loss, epilepsy, diffuse brain swelling, hydrocephalus, cerebral vein thrombosis, intra cerebral bleeding and cerebral palsy.[18] Acute neurological complications may lead to adverse consequences. In childhood acute bacterial meningitis deafness is the most common serious complication. Sensorineural hearing loss often develops during first few days of the illness as a result of inner ear dysfunction, but permanent deafness is rare and can be prevented by prompt treatment of meningitis.[19]
Those contract the disease during neonatal period and those infected by S pneumoniae and gram negative bacilli are in greater risk of developing neurological, auditory, or intellectual impairments or functionally important behaviour or learning disorders which can manifest as poor school performance.[20]
In adults central nervous system complications include cerebrovascular disease, brain swelling, hydrocephalus, intrcerebral bleeding; systemic complications are dominated by septic shock, adult respiratory distress syndrome and disseminated intravascular coagulation.[21] Those who have underlying predisposing conditions e.g. head injury may develop recurrent meningitis.[22] The case-fatality ratio is highest for gram-negative etiology and lowest for meningitis caused by H influenzae (also a gram negative bacili). Fatal outcome in patients over 60 years of age are more likely to be from systemic complications e.g. pneumonia, sepsis, cardio-respiratory failure; however in younger individuals it is usually associated with neurological complications.[22] Age more than 60, low glasgow coma scale at presentation and seizure within 24 hours increase the risk of death among community acquired meningitis.[23]
Risk Stratification and Prognosis
The overall mortality rate in Durand’s study was 25%
- Three factors were associated with a significantly higher mortality:
- Age > 60 (37% vs. 17%, p < 0.001, RR 2.1).
- Obtunded mental status on admission (49% vs. 16%, p < 0.001, RR 3.0).
- Onset of seizures within 48 hours of admission (72% vs. 18%, p < 0.001, RR 4.0).
- 98% of the patients in this study who died had at least one of these three risk factors.
Prevention
Immunization
All current vaccines target only bacterial meningitis.
Vaccinations against Haemophilus influenzae (Hib) have decreased early childhood meningitis significantly.[24]
Vaccines against type A and C Neisseria meningitidis, the kind that causes most disease in preschool children and teenagers in the United States, have also been around for a while. Type A is also prevalent in sub-Sahara Africa and W135 outbreaks have affected those on the Hajj pilgrimage to Mecca.
A vaccine called MeNZB for a specific strain of type B Neisseria meningitidis prevalent in New Zealand has completed trials and is being given to many people in the country under the age of 20. There is also a vaccine, MenBVac, for the specific strain of type B meningoccocal disease prevalent in Norway, and another specific vaccine for the strain prevalent in Cuba.
Pneumococcal polysaccharide vaccine against Streptococcus pneumoniae is recommended for all people 65 years of age or older. Pneumococcal conjugate vaccine is recommended for all newborns starting at 6 weeks - 2 months, according to American Association of Pediatrics (AAP) recommendations.
Prophylaxis
In cases of meningococcal meningitis, prophylactic treatment of close relatives with antibiotics (e.g. rifampicin, ciprofloxacin or ceftriaxone) may reduce the risk of further cases.[25]
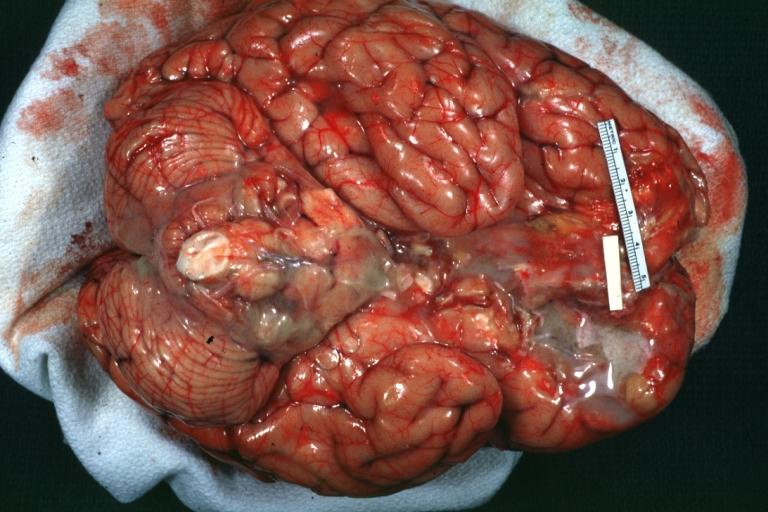
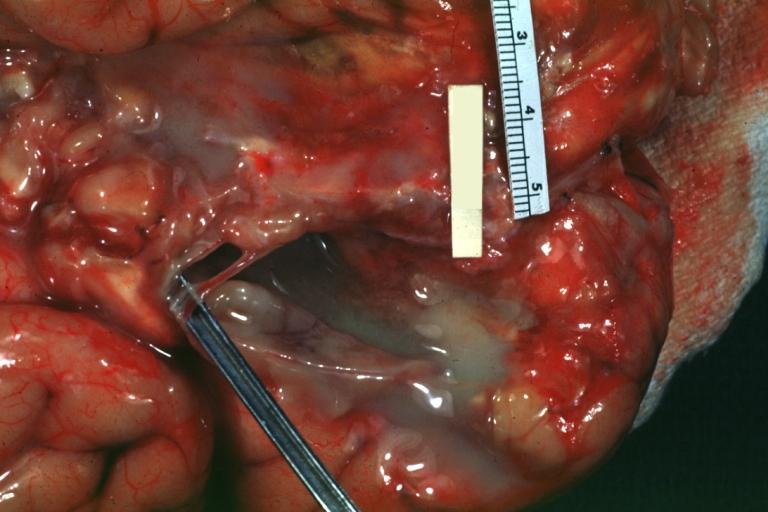
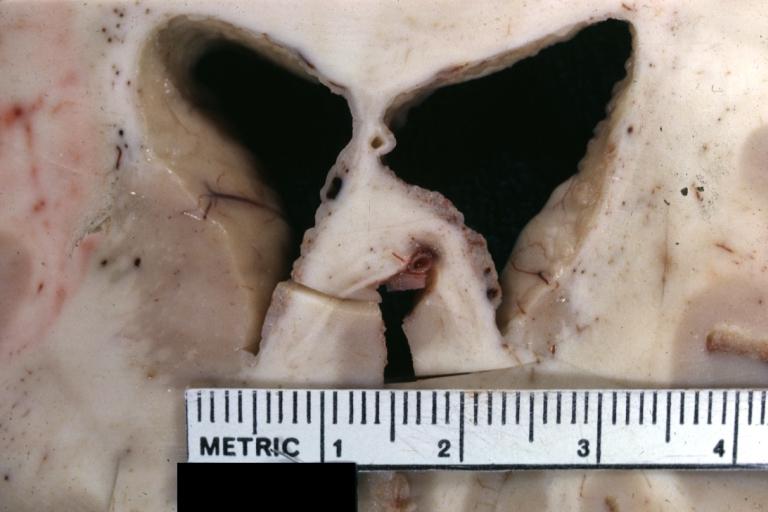
Pathological Findings
Images shown below are courtesy of Professor Peter Anderson DVM PhD and published with permission. © PEIR, University of Alabama at Birmingham, Department of Pathology
-

Meningitis: Gross, purulent leptomeningitis due to pneumococcus infection, an excellent example.
-
Bacterial Meningitis: Gross, basilar view


-
Bacterial Meningitis: Gross close-up
-

Meningitis: Gross base of frontal lobes well shown meningitis burn case with Pseudomonas sepsis


-

Meningitis: Gross natural color excellent demonstration of greenish pus in subarachnoid space
-
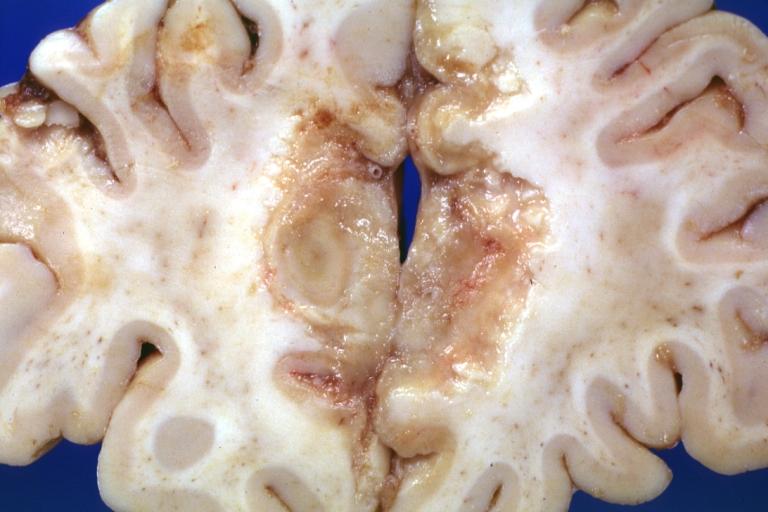
Tuberculous Meningitis: Gross fixed tissue close-up of large areas of necrosis in frontal parasagittal cortex secondary to tuberculous vasculitis. An excellent example


-
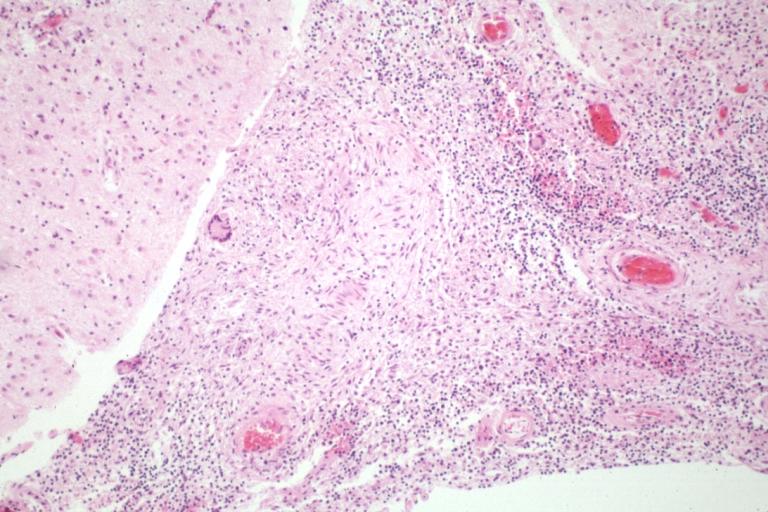
Tuberculous Meningitis: Micro low mag H&E. An excellent example with giant cells.
-

Purulent Meningitis: Gross natural color excellent photo lateral aspect of brain with easily seen purulent exudate due to Pneumococcus infection.


-
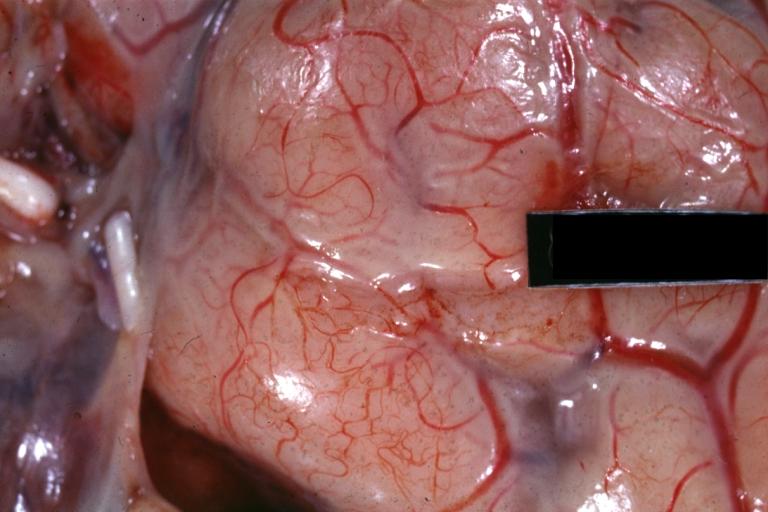
Purulent Meningitis: Gross natural color close-up view outstanding example of purulent exudate adjacent to blood vessels
-

Purulent Meningitis: Gross natural color Staphylococcal meningitis.


-
Ependymitis Granular Neoplastic: Gross fixed tissue close-up view and a spectacular one of this lesion case also has carcinomatous meningitis primary is lung oat cell.
-

Purulent Meningitis: Gross natural color brain in situ with removed calvarium very good illustration of exudate in meninges over convexities pneumococcus.


Acute pyogenic (bacterial) meningitis
<youtube v=L9jpjxTSLws/>
See also
References
- ↑ Durand, M.L., et.al., Acute bacterial meningitis: a review of 493 episodes, NEJM 1993; 328: 21-28. PMID 8416268
- ↑ Fekete, T., Clinical features of acute bacterial meningitis, in UpToDate, October 5, 1997.
- ↑ Quagliarello, V., Scheld, W.M., Bacterial meningitis: pathogenesis, pathophysiology, and progress, NEJM 1992; 327: 864-872. PMID 1508247
- ↑ Quagliarello, V., Scheld, W.M., Treatment of bacterial meningitis, NEJM 1997; 336: 708-716. PMID 9041103
- ↑ Schuchat, A., et.al., Bacterial meningitis in the United States in 1995, NEJM 1997; 337: 970-976. PMID 9395430
- ↑ Townsend, G.C., Scheld, W.M., The use of corticosteroids in the management of bacterial meningitis in adults, J Antimicrobial Chemotherapy 1996; 37: 1061-1061. PMID 8836809
- ↑ Ryan KJ, Ray CG (editors) (2004). Sherris Medical Microbiology (4th ed. ed.). McGraw Hill. pp. 876&ndash, 9. ISBN 0838585299.
- ↑ van de Beek D, de Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M (2004). "Clinical features and prognostic factors in adults with bacterial meningitis". N. Engl. J. Med. 351 (18): 1849–59. doi:10.1056/NEJMoa040845. PMID 15509818.
- ↑ Thomas KE, Hasbun R, Jekel J, Quagliarello VJ (2002). "The diagnostic accuracy of Kernig's sign, Brudzinski's sign, and nuchal rigidity in adults with suspected meningitis". Clin. Infect. Dis. 35 (1): 46–52. PMID 12060874.
- ↑ Provan, Drew (2005). Oxford Handbook of clinical and laboratory investigation. Oxford: Oxford university press. ISBN 0198566638. Unknown parameter
|coauthors=ignored (help) - ↑ Holub M, Beran O, Dzupova O; et al. (2007). "Cortisol levels in cerebrospinal fluid correlate with severity and bacterial origin of meningitis". Critical Care. 11: R41. doi:10.1186/cc5729.
- ↑ Nigrovic LE, Kuppermann N, Macias CG; et al. (2007). "Clinical prediction rule for identifying children with cerebrospinal fluid pleocytosis at very low risk of bacterial meningitis". JAMA. 297 (1): 52–60. doi:10.1001/jama.297.1.52. PMID 17200475.
- ↑ Sailer, Christian, Wasner, Susanne. Differential Diagnosis Pocket. Hermosa Beach, CA: Borm Bruckmeir Publishing LLC, 2002:77 ISBN 1591032016
- ↑ Kahan, Scott, Smith, Ellen G. In A Page: Signs and Symptoms. Malden, Massachusetts: Blackwell Publishing, 2004:68 ISBN 140510368X
- ↑ Beckham J, Tyler K (2006). "Initial Management of Acute Bacterial Meningitis in Adults: Summary of IDSA Guidelines". Rev Neurol Dis. 3 (2): 57–60. PMID 16819421.
- ↑ van de Beek D, de Gans J, McIntyre P, Prasad K (2007). "Corticosteroids for acute bacterial meningitis". Cochrane database of systematic reviews (Online) (1): CD004405. doi:10.1002/14651858.CD004405.pub2. PMID 17253505.
- ↑ Gottfredsson M, Perfect JR (2000). "Fungal meningitis". Seminars in neurology. 20 (3): 307–22. PMID 11051295.
- ↑ Vasallo, G (Jan 2004). "Neurological complications of pneumococcal meningitis". Developmental Medicine and Child Neurology. Vol. 46: pg. 11. Unknown parameter
|coauthors=ignored (help);|access-date=requires|url=(help) - ↑ Richardson MP, Reid A, Tarlow MJ, Rudd PT (1997). "Hearing loss during bacterial meningitis". Arch. Dis. Child. 76 (2): 134–8. PMID 9068303.
- ↑ Grimwood K (2001). "Legacy of bacterial meningitis in infancy. Many children continue to suffer functionally important deficits". BMJ. 323 (7312): 523–4. PMID 11546680.
- ↑ Pfister HW, Feiden W, Einhäupl KM (1993). "Spectrum of complications during bacterial meningitis in adults. Results of a prospective clinical study". Arch. Neurol. 50 (6): 575–81. PMID 8503793.
- ↑ 22.0 22.1 Adriani KS, van de Beek D, Brouwer MC, Spanjaard L, de Gans J (2007). "Community-acquired recurrent bacterial meningitis in adults". Clin. Infect. Dis. 45 (5): e46–51. doi:10.1086/520682. PMID 17682979.
- ↑ Durand ML, Calderwood SB, Weber DJ; et al. (1993). "Acute bacterial meningitis in adults. A review of 493 episodes". N. Engl. J. Med. 328 (1): 21–8. PMID 8416268.
- ↑ Peltola H (2000). "Worldwide Haemophilus influenzae type b disease at the beginning of the 21st century: global analysis of the disease burden 25 years after the use of the polysaccharide vaccine and a decade after the advent of conjugates". Clin. Microbiol. Rev. 13 (2): 302–17. PMID 10756001. Retrieved 2007-09-03.
- ↑ Fraser A, Gafter-Gvili A, Paul M, Leibovici L (2006). "Antibiotics for preventing meningococcal infections". Cochrane database of systematic reviews (Online) (4): CD004785. doi:10.1002/14651858.CD004785.pub3. PMID 17054214.
External links
- Template:Dmoz
- WHO: Meningococcal meningitis
- Merck Manual: Central nervous system infections
- Vaccination information from the NHS, UK
- CDC: Meningococcal disease
- CNN Health Library, Meningitis
- Information on Meningitis UK and the charity's search for a vaccine
- Information from the Meningitis Trust
- Information from the Meningitis Trust in New Zealand
Template:Diseases of the nervous system Template:SIB
af:Meningitis cs:Meningitida da:Meningitis de:Meningitis eo:Meningito eu:Meningitis fa:مننژیت gl:Meninxite ko:수막염 hr:Meningitis id:Meningitis is:Heilahimnubólga it:Meningite he:דלקת קרום המוח kk:Миқұрт la:Meningitis lt:Meningitas hu:Agyhártyagyulladás ms:Meningitis nl:Hersenvliesontsteking no:Meningitt qu:Ñutqu p'istuq llika unquy sq:Meningjiti simple:Meningitis sl:Meningitis fi:Aivokalvontulehdus sv:Hjärnhinneinflammation
- CS1 maint: Extra text: authors list
- CS1 maint: Extra text
- CS1 maint: Multiple names: authors list
- Pages with citations using unsupported parameters
- CS1 maint: Explicit use of et al.
- Pages using citations with accessdate and no URL
- Diseases involving the fasciae
- Inflammations
- Medical emergencies
- Neurological disorders
- Infectious Diseases
- Neurology