Hashimoto's thyroiditis
| Hashimoto's thyroiditis | |
| Histology | |
| ICD-10 | E06.3 |
| ICD-9 | 245.2 |
| OMIM | 140300 |
| DiseasesDB | 5649 |
| eMedicine | med/949 |
| MeSH | D050031 |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Phone:617-632-7753
Please Join in Editing This Page and Apply to be an Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [2] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Synonyms and Related Keywords: Hashimoto's thyroiditis; Chronic lymphocytic thyroiditis; Autoimmune thyroiditis
Overview
Hashimoto's thyroiditis or chronic lymphocytic thyroiditis is an autoimmune disease where the body's own antibodies attack the cells of the thyroid.
This disorder is believed to be the most common cause of primary hypothyroidism in North America. It occurs far more often in women than in men (10:1 to 20:1), and is most prevalent between 45 and 65 years of age.
In European countries an atrophic form of autoimmune thyroiditis (Ord's thyroiditis) is more common than Hashimoto's thyroiditis.
The disease begins slowly. It may take months or even years for the condition to be detected. Chronic thyroiditis is most common in women and people with a family history of thyroid disease. It affects between 0.1% and 5% of all adults in Western countries.
Hashimoto's disease may, in rare cases, be associated with other endocrine disorders caused by the immune system. Hashimoto's disease can occur with adrenal insufficiency and type 1 diabetes. In these cases, the condition is called type 2 polyglandular autoimmune syndrome (PGA II).
Less commonly, Hashimoto's disease occurs as part of a condition called type 1 polyglandular autoimmune syndrome (PGA I), along with:
- Adrenal insufficiency
- Fungal infections of the mouth and nails
- Hypoparathyroidism
Eponym

Also known as Hashimoto's disease, Hashimoto's thyroiditis is named after the Japanese physician Hashimoto Hakaru (1881−1934) of the medical school at Kyushu University,[1] who first described (He described four patients with a chronic disorder of the thyroid, which he termed struma lymphomatosa. The thyroid glands of these patients were characterized by diffuse lymphocytic infiltration, fibrosis, parenchymal atrophy, and an eosinophilic change in some of the acinar cells) the symptoms in 1912 in a German publication [2].
Pathophysiology
Hashimoto's thyroiditis is characterized by Iymphocytic infiltration of the thyroid gland and production of antibodies that recognize thyroid-specific antigens. It is currently thought that the disease is caused by abnormal suppressor T-lymphocyte function which results in a localized cell-mediated immune response directed toward the thyroid parenchymal cells. The pathogenesis is not completely understood (In contrast Graves' disease is caused by production of antibodies that mimic the action of thyroid-stimulating hormone, and nutritional goiter is caused by iodine deficiency).
The gland is usually diffusely enlarged, firm, and slightly lobular. The capsule is intact, and the cut surface is light tan and has a slight lobular pattern. Microscopically there is massive infiltration of the thyroid gland by lymphocytes and plasma cells. Germinal centers can often be seen in the gland. Thyroid follicles are usually absent and the few remaining follicles are devoid of colloid.
Causes
A family history of thyroid disorders is common, with the HLA-DR5 gene most strongly implicated conferring a relative risk of 3 in the UK.
The genes implicated vary in different ethnic groups and the incidence is increased in patients with chromosomal disorders, including Turner, Down's, and Klinefelter's syndromes.
The underlying specifics of the immune system destruction of thyroid cells is not clearly understood. Various autoantibodies may be present against thyroid peroxidase, thyroglobulin and TSH receptors, although a small percentage of patients may have none of these antibodies present. A percentage of the population may also have these antibodies without developing Hashimoto's thyroiditis.
Presentation
In many cases, Hashimoto's thyroiditis usually results in hypothyroidism, although in its acute phase, it can cause a transient hyperthyroidism thyrotoxic state known as hashitoxicosis.
Physiologically, antibodies against thyroid peroxidase and/or thyroglobulin cause gradual destruction of follicles in the thyroid gland. Accordingly, the disease can be detected clinically by looking for these antibodies in the blood. It is also characterised by invasion of the thyroid tissue by leukocytes, mainly T-lymphocytes. It is associated with non-Hodgkin lymphoma.
Possible Presentation forms of Hashimoto's Thyroiditis
- Adolescent goiter
- Alternating hypo- and hyperthyroidism
- Euthyroidism and goiter
- Hypothyroidism
- Painless thyroiditis or silent thyroiditis
- Postpartum painless thyrotoxicosis
- Primary thyroid failure
- Subclinical hypothyroidism and goiter
Symptoms of Hashimoto's Thyroiditis
(In alphabetical order) [3]
- Cold intolerance
- Constipation
- Depression
- Difficulty concentrating or thinking
- Dry skin
- Enlarged neck or presence of goiter
- Fast pulse
- Fatigue
- Hair loss
- Heavy and irregular periods
- High cholesterol
- Hyperthyroidism symptoms
- Hypothyroidism symptoms
- Infertility
- Lethargy
- Low pulse
- Mania
- Memory loss
- Migraines
- Myxedema
- Panic attacks
- Puffy face
- Reactive hypoglycemia
- Slowed reflexes
- Slowed speech
- Small or shrunken thyroid gland (late in the disease)
- Weight gain
- Weight loss
Other symptoms that can occur with this disease:
- Joint stiffness
- Swelling of the face
Treatment
Hypothyroidism caused by Hashimoto's Thyroiditis is treated with thyroid hormone replacement. A small pill taken once a day should be able to keep the thyroid hormone levels normal. This medicine will, in most cases, need to be taken for the rest of the patient's life.
Possible complications
If untreated for an extended period, Hashimoto's thyroiditis may lead to muscle failure, including possible heart failure.
Pathological Findings: A Case Example
Clinical Summary
A 49-year-old woman who complained during her yearly physical examination of tiredness and difficulty concentrating. She attributed these symptoms to stress at work. She had gained weight over the last year and despite warm weather, she felt chilled without a sweater.
Family history was significant for hypothyroidism in her mother and older sister.
On physical examination she had a pulse of 58 bpm and a blood pressure of 138/88 mm Hg. Examination of her neck disclosed a small thyroid gland with a palpable pyramidal lobe and a firm, bosselated texture. Serum taken at this time demonstrated a total T4 of 7.0 mcg/dL and a TSH of 22.0 mcIU/ml.
In addition, antithyroglobulin antibodies were positive at 1:640 and antimicrosomal antibodies were positive at 1:5120. These results supported the clinical impression of hypothyroidism; also, the texture of her thyroid gland and a positive family history suggested an autoimmune etiological factor.
She was referred to an endocrinologist for further evaluation; however, before beginning treatment she died suddenly from a ruptured berry aneurysm of the middle cerebral artery.
Autopsy Findings
At autopsy, significant subarachnoid hemorrhage from the ruptured berry aneurysm was documented. In addition, the thyroid gland was mildly enlarged and firm. On cut section the tissue was slightly pale.
Histopathological Findings
-

A gross photograph of thyroid gland taken at autopsy. The gland is only slightly enlarged and has a firm texture.
-
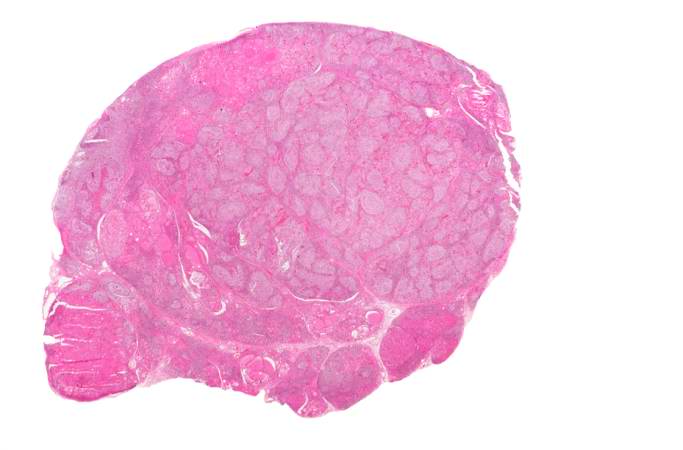
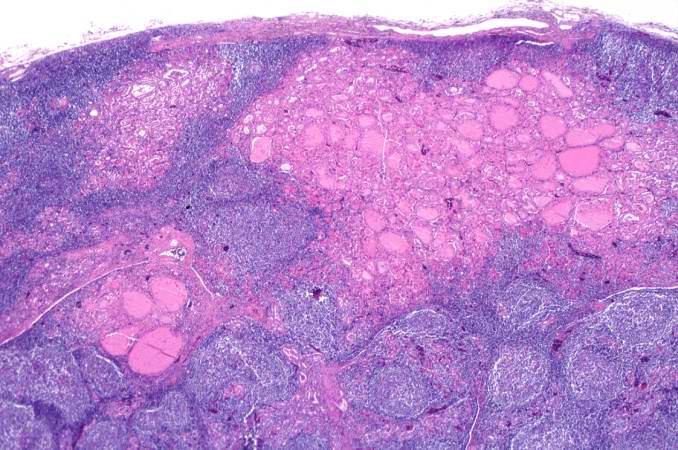
This is a low-power photomicrograph of thyroid from this case. Note that the tissue is more cellular than one would expect and there does not appear to be normal colloid-filled blue spaces in this gland.
-
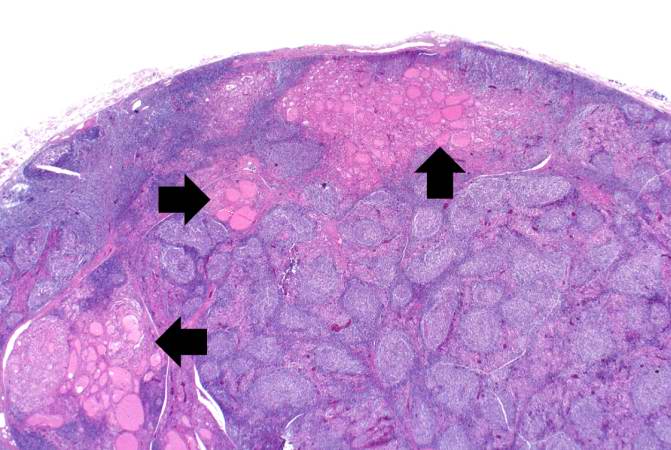
This is a higher-power photomicrograph of thyroid from this case. Note the large number of blue-staining inflammatory cells in this tissue. These cells appear to be forming germinal centers. Some residual thyroid gland tissue can be seen in this section (arrows).



-
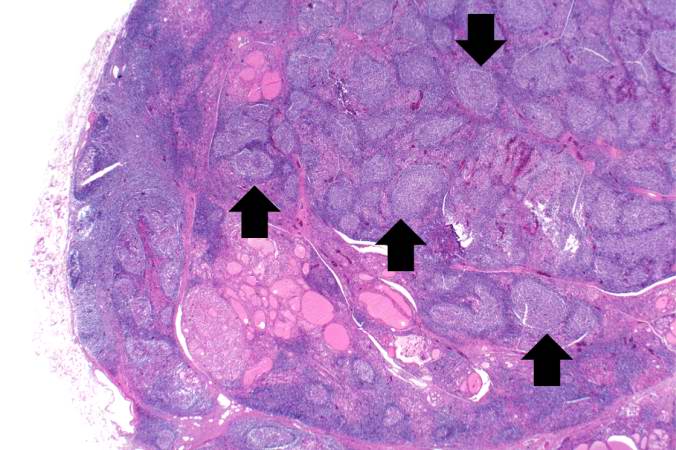
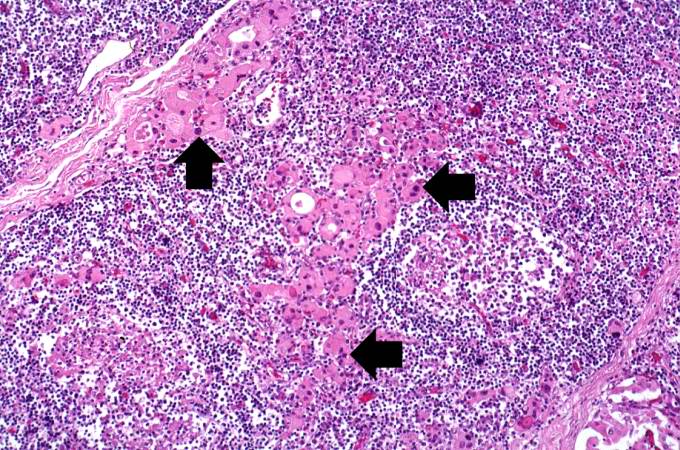
This is another view of thyroid gland filled with inflammatory cells forming germinal centers (arrows).
-
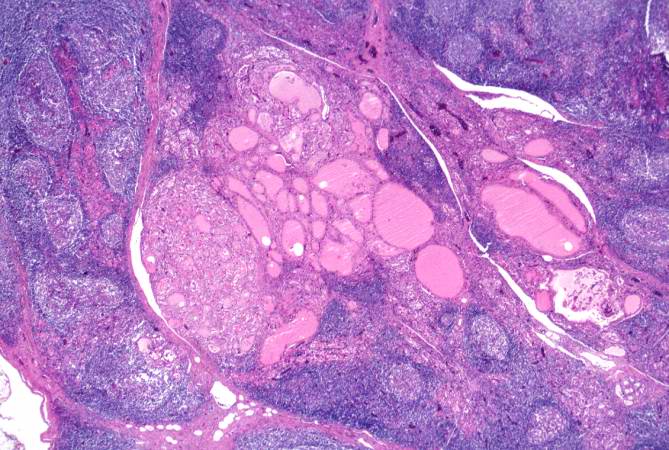
This is a higher-power photomicrograph of thyroid from this case showing the inflammatory cells and the residual thyroid tissue.
-
This is another higher-power photomicrograph of thyroid from this case showing the inflammatory cells and the residual thyroid tissue.



-
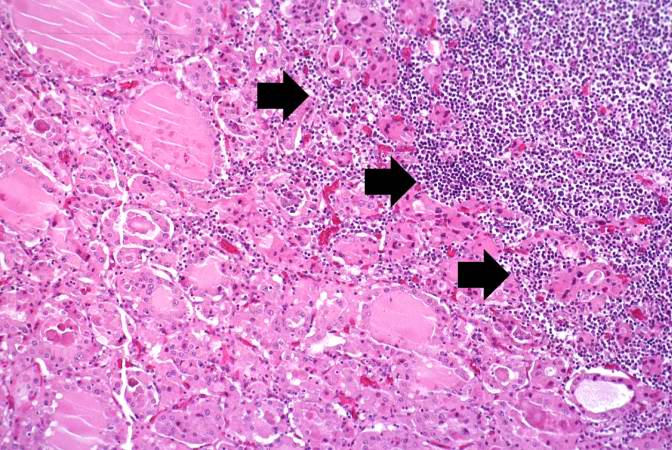
This is a high-power photomicrograph showing the inflammatory cells infiltrating into the residual thyroid tissue (arrows).
-
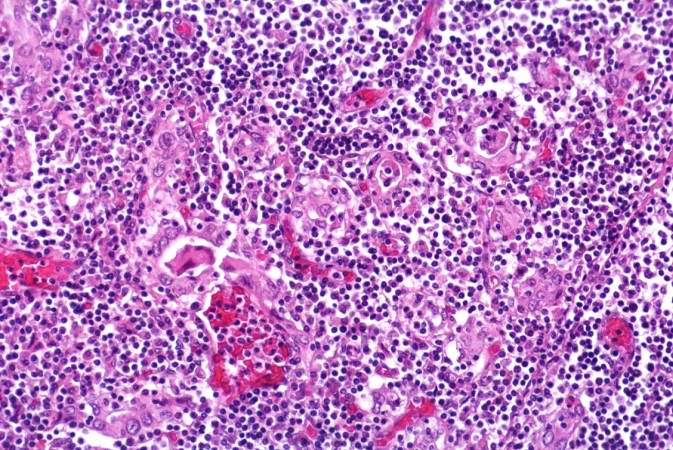
This is a high-power photomicrograph showing the lymphocytes and plasma cells surrounding the thyroid gland epithelium.
-
This high-power photomicrograph shows more clearly the lymphocytes and plasma cells surrounding the thyroid gland epithelium. Large, eosinophilic, degenerating thyroid gland cells (Hurthle cells) can be seen in this section (arrows).



References
- ↑ Template:WhoNamedIt
- ↑ H. Hashimoto: Zur Kenntnis der lymphomatösen Veränderung der Schilddrüse (Struma lymphomatosa). Archiv für klinische Chirurgie, Berlin, 1912, 97: 219−248.
- ↑ Ladenson P, Kim M. Thyroid. In: Goldman L and Ausiello D, eds. Goldman: Cecil Medicine. 23rd ed. Philadelphia, Pa:Saunders; 2007:chap 244.
External links
- Hashimoto's disease at the Mayo Clinic
- Hashimoto's Thyroiditis
- Alternative Health Solutions for Thyroid Autoimmunity
- Elaine Moore Graves' and Autoimmune Disease Education
Template:SIB de:Hashimoto-Thyreoiditis it:Tiroidite di Hashimoto he:השימוטו תירואידיטיס sv:Hashimotos sjukdom