Teratoma
For patient information click here

|
Teratoma Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Teratoma On the Web |
|
American Roentgen Ray Society Images of Teratoma |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Michael Maddaleni, B.S.
Overview
Historical Perspective
Pathophysiology
Epidemiology & Demographics
Risk Factors
Screening
Causes
Differentiating Teratoma
Complications & Prognosis
Diagnosis
History and Symptoms | Physical Examination | Staging | Laboratory tests | Electrocardiogram | X Rays | CT | MRI Echocardiography or Ultrasound | Other images | Alternative diagnostics
Treatment
Medical therapy | Surgical options | Primary prevention | Secondary prevention | Financial costs | Future therapies
Initial diagnosis
Teratomas are thought to be present since birth, or even before birth, and therefore can be considered congenital tumors. However, many teratomas are not diagnosed until much later in childhood or in adulthood. Large tumors are more likely to be diagnosed early on. Sacrococcygeal and cervical teratomas are often detected by prenatal ultrasound. Additional diagnostic methods may include prenatal MRI. In rare circumstances, the tumor is so large that the fetus may be damaged or die. In the case of large sacrococcygeal teratomas, a significant portion of the fetus' blood flow is redirected toward the teratoma (a phenomenon called steal syndrome), causing heart failure, or hydrops, of the fetus. In certain cases, fetal surgery may be indicated.
Beyond the newborn period, symptoms of a teratoma depend on its location and organ of origin. Ovarian teratomas often present with abdominal or pelvic pain, caused by torsion of the ovary or irritation of its ligaments. Testicular teratomas present as a palpable mass in the testis; mediastinal teratomas often cause compression of the lungs or the airways and may present with chest pain and/or respiratory symptoms.
Some teratomas contain yolk sac elements, which secrete alpha-fetoprotein (AFP). Detection of AFP may help to confirm the diagnosis and is often used as a marker for recurrence or treatment efficacy, but is rarely the method of initial diagnosis. (Maternal serum alpha-fetoprotein, or MSAFP, is a useful screening test for other fetal conditions, including Down syndrome, spina bifida and abdominal wall defects such as gastroschisis).
-
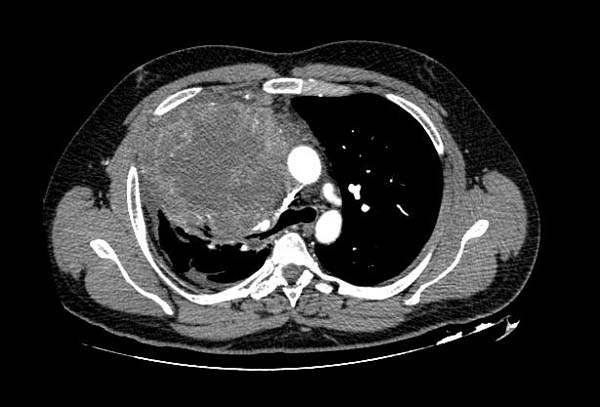
CT shows Mediastinal Teratoma

Time of presentation
Teratomas of germ cell origin usually are found (i.e., present) in adult men and women, but they may also be found in children and infants. Teratomas of embryonal origin are most often found in babies at birth, in young children, and, since the advent of ultrasound imaging, in fetuses.
The most commonly diagnosed fetal teratomas are sacrococcygeal teratoma (Altman types I, II, and III) and cervical (neck) teratoma. Because these teratomas project from the fetal body into the surrounding amniotic fluid, they can be seen during routine prenatal ultrasound exams. Teratomas within the fetal body are less easily seen with ultrasound; for these, MRI of the pregnant uterus is more informative.[1][2]
Complications
Teratomas are not dangerous for the fetus unless there is either a mass effect or a large amount of blood flow through the tumor (known as vascular steal). The mass effect frequently consists of obstruction of normal passage of fluids from surrounding organs. The vascular steal can place a strain on the growing heart of the fetus, even resulting in heart failure, and thus must be monitored by fetal echocardiography.
After surgery, there is a risk of regrowth in place, or in nearby organs.[3]
Treatment
Surgery
The treatment of choice is complete surgical removal (i.e., complete resection).[4][5] Teratomas normally are well encapsulated and non-invasive of surrounding tissues, hence they are relatively easy to resect from surrounding tissues. Exceptions include teratomas in the brain, and very large, complex teratomas that have pushed into and become interlaced with adjacent muscles and other structures.
Prevention of recurrence does not require en bloc resection of surrounding tissues.
Chemotherapy
For malignant teratomas, usually, surgery is followed by chemotherapy.
Teratomas that are in surgically inaccessible locations, or are very complex, or are likely to be malignant (due to late discovery and/or treatment) sometimes are treated first with chemotherapy.
Clinical trials
There are now (2007) two clinical trials in progress that address germ cell tumors, both of which include teratomas.[6][7]
Follow-up
Depending on which tissue(s) it contains, a teratoma may secrete a variety of chemicals with systemic effects. Some teratomas secrete the "pregnancy hormone" human chorionic gonadotropin (βhCG), which can be used in clinical practice to monitor the successful treatment or relapse in patients with a known HCG-secreting teratoma. This hormone is not recommended as a diagnostic marker, because most teratomas do not secrete it. Some teratomas secrete thyroxine, in some cases to such a degree that it can lead to clinical hyperthyroidism in the patient. Of special concern is the secretion of alpha-fetoprotein (AFP); under some circumstances AFP can be used as a diagnostic marker specific for the presence of yolk sac cells within the teratoma. These cells can develop into a frankly malignant tumor known as yolk sac tumor or endodermal sinus tumor.
Adequate follow-up requires close observation, involving repeated physical examination, scanning (ultrasound, MRI, or CT), and measurement of AFP and/or βhCG.[8][9]
Use in basic research
In light of the ethical issues surrounding the source of human stem cells, teratomas are being looked at as an alternative source for research since they lack the potential to grow into functional human beings.
References
- ↑ Diagnosis and characterization of fetal sacrococcygeal teratoma with prenatal MRI. Danzer E, Hubbard AM, Hedrick HL, Johnson MP, Wilson RD, Howell LJ, Flake AW, Adzick NS. AJR Am J Roentgenol. 2006 Oct;187(4):W350-6. PMID: 16985105 PubMed
- ↑ Pediatric presacral masses. Kocaoglu M, Frush DP. Radiographics. 2006 May-Jun;26(3):833-57. Review. PMID: 16702458 PubMed Free Text
- ↑ A recurred case of a mature ovarian teratoma presenting as a rectal mass (in Korean, abstract in English)
- ↑ Teratomas in infancy and childhood. A 54-year experience at the Children's Hospital Medical Center Tapper and Lack (1983) Ann Surg. 198(3): 398–410
- ↑ Germ-cell tumors in childhood and adolescence. GPOH MAKEI and the MAHO study groups Göbel et al (2000) Ann Oncol. 11(3): 263-271
- ↑ GCT1P1 Protocol / Clinical Study: Pilot study of Cisplatin, Etoposide, Bleomycin and Escalating Dose Cyclophosphamide Therapy for Children with High-Risk Malignant Germ Cell Tumors
- ↑ GCT132 Protocol / Clinical Study: A Phase III Study of Reduced Therapy in the Treatment of Children with Low and Intermediate Risk Extracranial Germ Cell Tumors (AGCT0132)
- ↑ Marina NM, Cushing B, Giller R, Cohen L, Lauer SJ, Ablin A, Weetman R, Cullen J, Rogers P, Vinocur C, Stolar C, Rescorla F, Hawkins E, Heifetz S, Rao PV, Krailo M, Castleberry RP (1999). "Complete surgical excision is effective treatment for children with immature teratomas with or without malignant elements: A Pediatric Oncology Group/Children's Cancer Group Intergroup Study". J. Clin. Oncol. 17 (7): 2137–43. PMID 10561269.
- ↑ Cushing B, Giller R, Ablin A, Cohen L, Cullen J, Hawkins E, Heifetz SA, Krailo M, Lauer SJ, Marina N, Rao PV, Rescorla F, Vinocur CD, Weetman RM, Castleberry RP (1999). "Surgical resection alone is effective treatment for ovarian immature teratoma in children and adolescents: a report of the pediatric oncology group and the children's cancer group". Am. J. Obstet. Gynecol. 181 (2): 353–8. PMID 10454682.
See also
Tumor pages for locations in which teratoma can occur:
Other conditions that may resemble a teratoma:
- Pilonidal cyst in humans
Technical information
- Orphanet page on teratoma
- EMedicine article on cystic teratoma (also search EMedicine for all articles containing the word teratoma)
- Monster Tumors Show Scientific Potential in War Against Cancer article in the New York Times
ar:ورم مسخي
bg:Тератом
de:Teratom
ko:기형종
it:Teratoma
he:טרטומה
nl:Teratoom
sv:Teratom