*[[File:Wolf-parkinson-white.jpg|thumb|WPW Syndrome was given in 1930 by Wolf- Parkinson- white. [https://en.ecgpedia.org/index.php?title=File:Wolffparkinsonwhite.jpg]|alt=|254x254px]][[WPW syndrome]] was described in 1930 and named for the [[John Parkinson]], [[Paul Dudley White]], and [[Louis Wolff]].
*[[File:Wolf-parkinson-white.jpg|thumb|WPW Syndrome was given in 1930 by Wolf- Parkinson- white. [https://en.ecgpedia.org/index.php?title=File:Wolffparkinsonwhite.jpg]|alt=|254x254px]][[WPW syndrome]] was described in 1930 and named for the [[John Parkinson]], [[Paul Dudley White]], and [[Louis Wolff]].
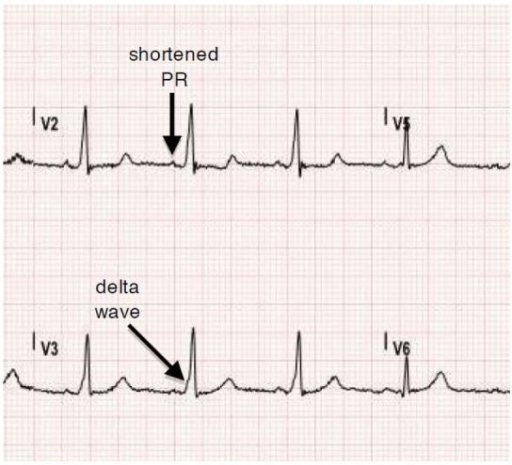
*They successfully interpreted a series of 11 [[healthy]] young [[patients]] who had repeated attacks of [[tachycardia]] in the presence of [[short PR interval]] and [[bundle branch block]] pattern on the [[ECG]] findings<ref>https://doi.org/10.1016/j.eupc.2004.09.005</ref>.
*They successfully interpreted a series of 11 [[healthy]] young [[patients]] who had repeated attacks of [[tachycardia]] in the presence of [[short PR interval]] and [[bundle branch block]] pattern on the [[ECG]] findings.
*British physiologist "Albert Frank Stanley Kent" (1863 - 1958), first described the lateral branches of [[AV grove]] of the [[monkey]] [[heart]], which was later named accessory [[bundle of Kent]].
*British physiologist "Albert Frank Stanley Kent" (1863 - 1958), first described the lateral branches of [[AV grove]] of the [[monkey]] [[heart]], which was later named accessory [[bundle of Kent]].
*In 1915, [[Frank Norman Wilson]] became the first to describe the [[condition]] which would later be referred to as [[Wolff–Parkinson–White syndrome]].
*In 1915, [[Frank Norman Wilson]] became the first to describe the [[condition]] which would later be referred to as [[Wolff–Parkinson–White syndrome]].
Line 22:
Line 22:
==Classification==
==Classification==
*Based on conduction pathway or fiber subtype [[ pre-excitation syndrome]] may be classified into sub-types<ref name="pmid1111564">{{cite journal |vauthors=Lowe KG, Emslie-Smith D, Ward C, Watson H |title=Classification of ventricular pre-excitation. Vectorcardiographic study |journal=Br Heart J |volume=37 |issue=1 |pages=9–19 |date=January 1975 |pmid=1111564 |pmc=484149 |doi=10.1136/hrt.37.1.9 |url=}}</ref>
*Based on conduction pathway or fiber subtype [[ pre-excitation syndrome]] may be classified into sub-types
{| class="wikitable"
{| class="wikitable"
Line 50:
Line 50:
|}<br />
|}<br />
*Based on their [[conduction]] properties, three types of [[Accessory pathways]] are there<ref name="pmid4561817">{{cite journal |vauthors=Kuramoto K, Matsushita S |title=[Classification and interpretation of WPW syndrome] |language=Japanese |journal=Nippon Rinsho |volume=30 |issue=8 |pages=1770–8 |date=August 1972 |pmid=4561817 |doi= |url=}}</ref>:
*Based on their [[conduction]] properties, three types of [[Accessory pathways]] are there:
*#[[Accessory pathway|Manifest Accessory Pathways]]: [[Conducts]] more rapidly as compared to [[AV nodal conduction]]. [[Delta waves]] will commonly be seen on [[ECG]].
*#[[Accessory pathway|Manifest Accessory Pathways]]: [[Conducts]] more rapidly as compared to [[AV nodal conduction]]. [[Delta waves]] will commonly be seen on [[ECG]].
*#[[Concealed]] [[Accessory Pathways]]: [[Conducts]] in the [[retrograde direction]]. As its name represents, the changes in [[ECG]] will be [[concealed]]. No [[delta waves]] will be seen.
*#[[Concealed]] [[Accessory Pathways]]: [[Conducts]] in the [[retrograde direction]]. As its name represents, the changes in [[ECG]] will be [[concealed]]. No [[delta waves]] will be seen.
Line 57:
Line 57:
==Pathophysiology==
==Pathophysiology==
[[File: Pathophysiology of WPW- Pre-excitation syndrome.jpg|thumb|Pathophysiology of WPW / Pre-excitation syndrome.[https://www.slideshare.net/smcmedicinedept/ecg-wpw-syndrome?next_slideshow=3]]]
[[File: Pathophysiology of WPW- Pre-excitation syndrome.jpg|thumb|Pathophysiology of WPW / Pre-excitation syndrome.[https://www.slideshare.net/smcmedicinedept/ecg-wpw-syndrome?next_slideshow=3]]]
Normally the [[electrical]] activity in the [[heart]] starts with [[SA node]]. The [[impulse]] generation usually happens in the right [[atrium]] near the [[entrance]] of [[superior vena cava]]<ref name="urlWolff-Parkinson-White pattern - Conditions - GTR - NCBI">{{cite web |url=https://www.ncbi.nlm.nih.gov/gtr/conditions/C0043202/ |title=Wolff-Parkinson-White pattern - Conditions - GTR - NCBI |format= |work= |accessdate=}}</ref>. The [[impulse]] from the [[SA node]] travels to the [[AV node]]. The [[AV node ]] modulates the rate and number of [impulses]] to be conducted to the [[ventricles]]. The [[AV node]] also modulates the speed of transmission from [[atria]] to [[ventricles]] represents the [[PR interval]] on ECG. From the [[AV node]], an [[electrical]] [[impulse]] is transmitted to the [[bundle of His]], to left and right branches extending to the [[ventricular]] [[myocardium]].
[[WPW]]<ref name="urlWhat is the pathophysiology of Wolff-Parkinson-White (WPW) syndrome?">{{cite web |url=https://www.medscape.com/answers/159222-53990/what-is-the-pathophysiology-of-wolff-parkinson-white-wpw-syndrome |title=What is the pathophysiology of Wolff-Parkinson-White (WPW) syndrome? |format= |work= |accessdate=}}</ref> is another word for [[pre-excitation]] of the [[ventricle]] through the [[accessory]] [[pathway]] instead of going through the usual pathway of [[AV node]] which usually slows down the [[speed]] of [[conduction]] of [[impulses]] transmitting to [[ventricles]]. The [[accessory]] pathway creates a channel directly to [[conduct]] the [[impulses]] to [[ventricles]] resulting in [[premature]] [[excitation]]. In "Type A [[Pre-excitation]]" [[accessory]] pathway lies between [[Left atria]] [[ventricles]] and in Type B [[pre-excitation]] fibers carry impulses between [[right atria]] and [[ventricles]]<ref name="urlAmerican Heart Association | To be a relentless force for a world of longer, healthier lives">{{cite web |url=https://www.heart.org/?identifier=563 |title=American Heart Association | To be a relentless force for a world of longer, healthier lives |format= |work= |accessdate=}}</ref><ref name="urlWolff-Parkinson-White (WPW) Syndrome ECG Review - Criteria and Examples | LearntheHeart.com">{{cite web |url=https://www.healio.com/cardiology/learn-the-heart/ecg-review/ecg-topic-reviews-and-criteria/wpw-review |title=Wolff-Parkinson-White (WPW) Syndrome ECG Review - Criteria and Examples | LearntheHeart.com |format= |work= |accessdate=}}</ref>.
* Normally the [[electrical]] activity in the [[heart]] starts from [[SA node]].
* The [[impulse]] generation usually happens in the right [[atrium]] near the [[entrance]] of [[superior vena cava]] and it travels from [[SA node]] to the [[AV node]].<ref name="urlWolff-Parkinson-White pattern - Conditions - GTR - NCBI">{{cite web |url=https://www.ncbi.nlm.nih.gov/gtr/conditions/C0043202/ |title=Wolff-Parkinson-White pattern - Conditions - GTR - NCBI |format= |work= |accessdate=}}</ref>
* The [[AV node ]] modulates the rate and number of [impulses]] to be conducted to the [[ventricles]]. The [[AV node]] also modulates the speed of transmission from [[atria]] to [[ventricles]] represents the [[PR interval]] on ECG. From the [[AV node]], an [[electrical]] [[impulse]] is transmitted to the [[bundle of His]], to left and right branches extending to the [[ventricular]] [[myocardium]].
[[WPW]] is another word for [[pre-excitation]] of the [[ventricle]] through the [[accessory]] [[pathway]] instead of going through the usual pathway of [[AV node]] which usually slows down the [[speed]] of [[conduction]] of [[impulses]] transmitting to [[ventricles]]. The [[accessory]] pathway creates a channel directly to [[conduct]] the [[impulses]] to [[ventricles]] resulting in [[premature]] [[excitation]]. In "Type A [[Pre-excitation]]" [[accessory]] pathway lies between [[Left atria]] [[ventricles]] and in Type B [[pre-excitation]] fibers carry impulses between [[right atria]] and [[ventricles]].
Basic concept of Pathophysiology in [[pre-excitation syndrome]] lies in the concept of bypassing the [[AV node]] [[conduction]] and letting the [[impulse conduct]] faster through [[atria]] to [[ventricles]] via [[accessory pathways]]. These [[accessory pathways]] Usually called [[Bundle of Kent]] in [[WPW syndrome]], [[James fiber]] in [[LGL syndrome]] and [[Mahaim fibers]] in Mahaim type [[pre-excitation syndrome]]. These conducts [[impulses]] in forward (not common), backward ( around 15-20%) and in both directions ( Most common type) as well.
Basic concept of Pathophysiology in [[pre-excitation syndrome]] lies in the concept of bypassing the [[AV node]] [[conduction]] and letting the [[impulse conduct]] faster through [[atria]] to [[ventricles]] via [[accessory pathways]]. These [[accessory pathways]] Usually called [[Bundle of Kent]] in [[WPW syndrome]], [[James fiber]] in [[LGL syndrome]] and [[Mahaim fibers]] in Mahaim type [[pre-excitation syndrome]]. These conducts [[impulses]] in forward (not common), backward ( around 15-20%) and in both directions ( Most common type) as well.
The [[accessory pathways]] mediate the occurrence of [[tachyarrhythmia]] by forming a [[re-entry]] circuit and commonly known as [[AVRT]]. The direct [[conduction]] of [[impulses]] from [[atria]] to [[ventricles]] can also result in the development of [[tachyarrhythmia's]] when there is a development of [[Atrial Fibrillation]] with [[RVR]]<ref name="pmid28328711">{{cite journal |vauthors=Moskowitz A, Chen KP, Cooper AZ, Chahin A, Ghassemi MM, Celi LA |title=Management of Atrial Fibrillation with Rapid Ventricular Response in the Intensive Care Unit: A Secondary Analysis of Electronic Health Record Data |journal=Shock |volume=48 |issue=4 |pages=436–440 |date=October 2017 |pmid=28328711 |pmc=5603354 |doi=10.1097/SHK.0000000000000869 |url=}}</ref>
The [[accessory pathways]] mediate the occurrence of [[tachyarrhythmia]] by forming a [[re-entry]] circuit and commonly known as [[AVRT]]. The direct [[conduction]] of [[impulses]] from [[atria]] to [[ventricles]] can also result in the development of [[tachyarrhythmia's]] when there is a development of [[Atrial Fibrillation]] with [[RVR]]
[[WPW syndrome]] is a combination of [[WPW]] pattern on [[ECG]] + [[Paroxysmal arrhythmias]]. The [[accessory pathways]] are usually named as [[Bundle of Kent]] or [[AV]] [[bypass tracts]]. [[Accessory pathways|The accessory pathways]] here are named as [[James fibers]], also known as [[Atrionodal fibers]] connecting the [[Atrium (heart)|atrium]] to the distal [[Atrioventricular node|AV node]]. These usually [[conduct]] the [[impulses]] from [[atria]] to the initial portion of the [[AV node]]. [[Accessory pathways|The accessory pathways]] named as [[Mahaim fibers]] connect the [[Atrium (heart)|Atrium]], [[AV node]], or [[bundle of His]] to the [[Purkinje fibers]] or [[ventricular myocardium]]. <br />
[[WPW syndrome]] is a combination of [[WPW]] pattern on [[ECG]] + [[Paroxysmal arrhythmias]]. The [[accessory pathways]] are usually named as [[Bundle of Kent]] or [[AV]] [[bypass tracts]]. [[Accessory pathways|The accessory pathways]] here are named as [[James fibers]], also known as [[Atrionodal fibers]] connecting the [[Atrium (heart)|atrium]] to the distal [[Atrioventricular node|AV node]]. These usually [[conduct]] the [[impulses]] from [[atria]] to the initial portion of the [[AV node]]. [[Accessory pathways|The accessory pathways]] named as [[Mahaim fibers]] connect the [[Atrium (heart)|Atrium]], [[AV node]], or [[bundle of His]] to the [[Purkinje fibers]] or [[ventricular myocardium]]. <br />
Line 81:
Line 84:
! style="background: #4479BA; width: 200px;" |{{fontcolor|#FFF|Co-existing Conditions}}
! style="background: #4479BA; width: 200px;" |{{fontcolor|#FFF|Co-existing Conditions}}
|-
|-
| style="padding: 5px 5px; background: #DCDCDC; font-weight: bold" |[[Atrial fibrillation|Atrial Fibrillation]]<ref name="pmid22518390">{{cite journal |vauthors=Harris K, Edwards D, Mant J |title=How can we best detect atrial fibrillation? |journal=J R Coll Physicians Edinb |volume=42 Suppl 18 |issue= |pages=5–22 |date=2012 |pmid=22518390 |doi=10.4997/JRCPE.2012.S02 |url=}}</ref><ref name="pmid24837984">{{cite journal |vauthors=Lankveld TA, Zeemering S, Crijns HJ, Schotten U |title=The ECG as a tool to determine atrial fibrillation complexity |journal=Heart |volume=100 |issue=14 |pages=1077–84 |date=July 2014 |pmid=24837984 |doi=10.1136/heartjnl-2013-305149 |url=}}</ref> (AFib)
*[[WPW]] is commonly found with an [[incidence]] of around 0.1-3.0 per thousand [[population]]<ref name="pmid22579340">{{cite journal |vauthors=Cohen MI, Triedman JK, Cannon BC, Davis AM, Drago F, Janousek J, Klein GJ, Law IH, Morady FJ, Paul T, Perry JC, Sanatani S, Tanel RE |title=PACES/HRS expert consensus statement on the management of the asymptomatic young patient with a Wolff-Parkinson-White (WPW, ventricular preexcitation) electrocardiographic pattern: developed in partnership between the Pediatric and Congenital Electrophysiology Society (PACES) and the Heart Rhythm Society (HRS). Endorsed by the governing bodies of PACES, HRS, the American College of Cardiology Foundation (ACCF), the American Heart Association (AHA), the American Academy of Pediatrics (AAP), and the Canadian Heart Rhythm Society (CHRS) |journal=Heart Rhythm |volume=9 |issue=6 |pages=1006–24 |date=June 2012 |pmid=22579340 |doi=10.1016/j.hrthm.2012.03.050 |url=}}</ref>.
*[[WPW]] is commonly found with an [[incidence]] of around 0.1-3.0 per thousand [[population]].
*More common in the [[male]] [[population]] as compared to [[females]]<ref>http://www.cardiology.sk/casopis/606/pdf/04.pdf</ref>.
*More common in the [[male]] [[population]] as compared to [[females]].
*[[Familial studies]] are done to found its association proved that around .55% more commonly found in first degree relatives.
*[[Familial studies]] are done to found its association proved that around .55% more commonly found in first degree relatives.
*More common in [[young]] and [[healthy]] [[individuals]] and as the [[age]] advances the [[prevalence]] of [[disease]] [[decreases]] because of loss of [[pre-excitation]].
*More common in [[young]] and [[healthy]] [[individuals]] and as the [[age]] advances the [[prevalence]] of [[disease]] [[decreases]] because of loss of [[pre-excitation]].
Line 323:
Line 326:
==Risk Factors==
==Risk Factors==
High-risk [[population]] for development of [[atrial fibrillation]] or [[sudden cardiac death]] include<ref name="pmid22532593">{{cite journal |vauthors=Obeyesekere MN, Leong-Sit P, Massel D, Manlucu J, Modi S, Krahn AD, Skanes AC, Yee R, Gula LJ, Klein GJ |title=Risk of arrhythmia and sudden death in patients with asymptomatic preexcitation: a meta-analysis |journal=Circulation |volume=125 |issue=19 |pages=2308–15 |date=May 2012 |pmid=22532593 |doi=10.1161/CIRCULATIONAHA.111.055350 |url=}}</ref>:
High-risk [[population]] for development of [[atrial fibrillation]] or [[sudden cardiac death]] include:
*[[Pilots]]
*[[Pilots]]
Line 342:
Line 345:
===Complications===
===Complications===
*Most common [[complications]] studied in patients having [[accessory pathway]] [[Conduction basics|conduction]] are [[Arrhythmias]] and [[Sudden cardiac death]]<ref>https://www.cancertherapyadvisor.com/home/decision-support-in-medicine/hospital-medicine/pre-excitation-syndrome-wpw/</ref>
*Most common [[complications]] studied in patients having [[accessory pathway]] [[Conduction basics|conduction]] are [[Arrhythmias]] and [[Sudden cardiac death]]
*[[Tachyarrhythmias]]:
*[[Tachyarrhythmias]]:
**If there is a development of [[atrial fibrillation]] or flutter then there is [[fast conduction]] across the [[tracts]] leads to an increased risk of dangerous [[ventricular arrhythmias]].
**If there is a development of [[atrial fibrillation]] or flutter then there is [[fast conduction]] across the [[tracts]] leads to an increased risk of dangerous [[ventricular arrhythmias]].
**[[AV nodal block|AV nodal]] blocking agents may also be the factor responsible for the [[increased]] [[Conduction System|conduction]] through [[accessory pathways]] causing life-threatening [[ventricular arrhythmias]] or [[hemodynamic]] instability resulting and with a worse [[prognosis]].
**[[AV nodal block|AV nodal]] blocking agents may also be the factor responsible for the [[increased]] [[Conduction System|conduction]] through [[accessory pathways]] causing life-threatening [[ventricular arrhythmias]] or [[hemodynamic]] instability resulting and with a worse [[prognosis]].
*[[Sudden cardiac death]]<ref name="urlWolff-Parkinson-White Syndrome. WPW syndrome info | Patient">{{cite web |url=https://patient.info/doctor/wolff-parkinson-white-syndrome-pro#:~:text=Wolff-Parkinson-White%20%28WPW%29%20syndrome%20is%20the%20most%20common%20of,result%20in%20serious%20cardiovascular%20complications%20and%20sudden%20death. |title=Wolff-Parkinson-White Syndrome. WPW syndrome info | Patient |format= |work= |accessdate=}}</ref>:
*[[Sudden cardiac death]]:
**[[Sudden cardiac death]] as a [[complication]] in patients with [[AP conduction]] is more common in a young [[male]] with age less than 35, history of [[arrhythmias]] in the past, [[Anatomical|anatomical location]] of [[accessory pathway]]- that is the [[septal]] location of the [[accessory pathway]], having multiple accessory pathways.
**[[Sudden cardiac death]] as a [[complication]] in patients with [[AP conduction]] is more common in a young [[male]] with age less than 35, history of [[arrhythmias]] in the past, [[Anatomical|anatomical location]] of [[accessory pathway]]- that is the [[septal]] location of the [[accessory pathway]], having multiple accessory pathways.
**The studies proved the risk of [[sudden cardiac death]] related to the [[pre-excitation syndrome]] is around 1.5% in childhood with the highest [[risk]] in the first two decades of life.
**The studies proved the risk of [[sudden cardiac death]] related to the [[pre-excitation syndrome]] is around 1.5% in childhood with the highest [[risk]] in the first two decades of life.
Line 363:
Line 366:
===WPW Syndrome===
===WPW Syndrome===
*[[WPW syndrome]] is a combination of [[WPW]] pattern on [[ECG]] + [[Paroxysmal arrhythmias]]. The [[accessory pathways]] are usually named as [[Bundle of Kent]] or [[AV]] [[bypass tracts]]<ref name="urlWolff-Parkinson-White (WPW) syndrome - Diagnosis and treatment - Mayo Clinic">{{cite web |url=https://www.mayoclinic.org/diseases-conditions/wolff-parkinson-white-syndrome/diagnosis-treatment/drc-20354630 |title=Wolff-Parkinson-White (WPW) syndrome - Diagnosis and treatment - Mayo Clinic |format= |work= |accessdate=}}</ref>.
*[[WPW syndrome]] is a combination of [[WPW]] pattern on [[ECG]] + [[Paroxysmal arrhythmias]]. The [[accessory pathways]] are usually named as [[Bundle of Kent]] or [[AV]] [[bypass tracts]].
===Mahaim-Type Pre-excitation<ref name="pmid15489095">{{cite journal |vauthors=Sternick EB, Timmermans C, Sosa E, Cruz FE, Rodriguez LM, Fagundes MA, Gerken LM, Wellens HJ |title=The electrocardiogram during sinus rhythm and tachycardia in patients with Mahaim fibers: the importance of an "rS" pattern in lead III |journal=J. Am. Coll. Cardiol. |volume=44 |issue=8 |pages=1626–35 |date=October 2004 |pmid=15489095 |doi=10.1016/j.jacc.2004.07.035 |url=}}</ref>===
===Mahaim-Type Pre-excitation===
*The [[accessory pathways]] named as [[Mahaim fibers]] connect the [[Atrium (heart)|Atrium]], [[AV node]], or [[bundle of His]] to the [[Purkinje fibers]] or [[ventricular myocardium]].
*The [[accessory pathways]] named as [[Mahaim fibers]] connect the [[Atrium (heart)|Atrium]], [[AV node]], or [[bundle of His]] to the [[Purkinje fibers]] or [[ventricular myocardium]].
Line 412:
Line 415:
[[HEMODYNAMICALLY]] STABLE [[PATIENTS]] -- THE FOLLOWING ALGORITHM CAN BE FOLLOWED
[[HEMODYNAMICALLY]] STABLE [[PATIENTS]] -- THE FOLLOWING ALGORITHM CAN BE FOLLOWED
<u>GENERAL PROTOCOL<ref name="pmid30056397">{{cite journal |vauthors=Stasiak A, Niewiadomska-Jarosik K, Kędziora P |title=Clinical course and treatment of children and adolescents with the preexcitation syndrome - own studies |journal=Dev Period Med |volume=22 |issue=2 |pages=113–122 |date=2018 |pmid=30056397 |doi= |url=}}</ref></u>
<u>GENERAL PROTOCOL</u>
*[[Antiarrhythmic drug]]
*[[Antiarrhythmic drug]]
Line 433:
Line 436:
**IV [[Verapamil]]- this is a [[calcium]] [[channel blocker]] and commonly used as 5-10 mg.
**IV [[Verapamil]]- this is a [[calcium]] [[channel blocker]] and commonly used as 5-10 mg.
<u>[[ATRIAL FLUTTER]]/[[FIBRILLATION]]<ref name="pmid23545139">{{cite journal |vauthors=Wann LS, Curtis AB, Ellenbogen KA, Estes NA, Ezekowitz MD, Jackman WM, January CT, Lowe JE, Page RL, Slotwiner DJ, Stevenson WG, Tracy CM, Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Le Heuzey J, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann LS |title=Management of patients with atrial fibrillation (compilation of 2006 ACCF/AHA/ESC and 2011 ACCF/AHA/HRS recommendations): a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines |journal=Circulation |volume=127 |issue=18 |pages=1916–26 |date=May 2013 |pmid=23545139 |doi=10.1161/CIR.0b013e318290826d |url=}}</ref></u>
<u>[[ATRIAL FLUTTER]]/[[FIBRILLATION]]</u>
*If [[wide complex]] [[tachycardia]] is present
*If [[wide complex]] [[tachycardia]] is present
Line 452:
Line 455:
Class 3 [[Antiarrhythmics]] and class IC drugs are used with [[AV nodal block|AV nodal]] blocking [[agents]] in patients with a history of [[atrial flutter]] or [[Atrial fibrillation|A.Fib]]. [[Sotalol]] and [[Flecainide]] would be the safe options to use in [[pregnancy]].
Class 3 [[Antiarrhythmics]] and class IC drugs are used with [[AV nodal block|AV nodal]] blocking [[agents]] in patients with a history of [[atrial flutter]] or [[Atrial fibrillation|A.Fib]]. [[Sotalol]] and [[Flecainide]] would be the safe options to use in [[pregnancy]].
===Surgical management<ref name="urlSurgical treatment of patients with Wolff-Parkinson-White syndrome and associated acquired valvular heart disease - ScienceDirect">{{cite web |url=https://www.sciencedirect.com/science/article/pii/S0022522394702209#:~:text=The%20surgical%20technique%20used%20for%20the%20treatment%20of,of%20the%20involved%20valve%20anulus%2C%20and%20%283%29%20cryoablation. |title=Surgical treatment of patients with Wolff-Parkinson-White syndrome and associated acquired valvular heart disease - ScienceDirect |format= |work= |accessdate=}}</ref>===
British physiologist "Albert Frank Stanley Kent" (1863 - 1958), first described the lateral branches of AV grove of the monkeyheart, which was later named accessory bundle of Kent.
Initial R wave in V1, initial r > 40 ms in V1/V2, notched S in V1, initial R in aVR, lead II R wave peak time ≥50 ms, no RS in V1-V6, and atrioventricular dissociation
WPW can be considered as a congenital anomaly in some cases where it is usually present since birth and in others and it is regarded as a developmental anomaly. Studies proved it's lowerprevalence in childrenaged between 6-13 than those in the age group of 14-15 years of age.
Catheter Ablation- Surgical Approach in WPW. Image showing catheter ablation of right free wall accessory pathway. The first successful ablation was performed by Morady and Scheinman. [3]
Patients who are not willing to undergo radiofrequencyablation can be managed on medical management with the use of Anti-arrhythmic. Though its role in the prevention of future episodes of arrhythmias is limited still this is the most commonly used modality of choice.
↑Obeyesekere MN, Leong-Sit P, Massel D, Manlucu J, Modi S, Krahn AD, Skanes AC, Yee R, Gula LJ, Klein GJ (May 2012). "Risk of arrhythmia and sudden death in patients with asymptomatic preexcitation: a meta-analysis". Circulation. 125 (19): 2308–15. doi:10.1161/CIRCULATIONAHA.111.055350. PMID22532593.
↑Cohen MI, Triedman JK, Cannon BC, Davis AM, Drago F, Janousek J, Klein GJ, Law IH, Morady FJ, Paul T, Perry JC, Sanatani S, Tanel RE (June 2012). "PACES/HRS expert consensus statement on the management of the asymptomatic young patient with a Wolff-Parkinson-White (WPW, ventricular preexcitation) electrocardiographic pattern: developed in partnership between the Pediatric and Congenital Electrophysiology Society (PACES) and the Heart Rhythm Society (HRS). Endorsed by the governing bodies of PACES, HRS, the American College of Cardiology Foundation (ACCF), the American Heart Association (AHA), the American Academy of Pediatrics (AAP), and the Canadian Heart Rhythm Society (CHRS)". Heart Rhythm. 9 (6): 1006–24. doi:10.1016/j.hrthm.2012.03.050. PMID22579340.
Cookies help us deliver our services. By using our services, you agree to our use of cookies.





![[1]](https://en.ecgpedia.org/index.php?title=File:Wolffparkinsonwhite.jpg){kind=link}

{kind=link}
