Stress cardiomyopathy criteria
|
Stress cardiomyopathy Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Unstable angina/non ST elevation myocardial infarction in Stress (Takotsubo) Cardiomyopathy |
|
Case Studies |
|
Stress cardiomyopathy criteria On the Web |
|
American Roentgen Ray Society Images of Stress cardiomyopathy criteria |
|
Risk calculators and risk factors for Stress cardiomyopathy criteria |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Dima Nimri, M.D. [2]
Overview
Mayo Clinic Criteria
In 2004, researchers at the Mayo Clinic proposed a criteria for the diagnosis of stress cardiomyopathy. All 4 points of the criteria must be fulfilled:[1][2]
- Transient hypokinesis, akinesis, or dyskinesis of the left ventricular mid segments with or without apical involvement; the regional wall motion abnormalities extend beyond a single epicardial vascular distribution; a stressful trigger is often, but not always present.
- Absence of obstructive coronary disease or angiographic evidence of acute plaque rupture.
- New electrocardiographic abnormalities (either ST-segment elevation and/or T-wave inversion) or modest elevation in cardiac troponin.
- Absence of pheochromocytoma and myocarditis.
The Various Patterns of Wall Motion Abnormalities
It should be that the wall motion abnormalities are not always anteroapical.
-
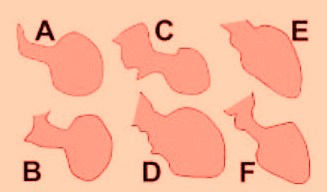
Different end-systolic left ventricular (LV) silhouettes.

A, [3]; B, [4]; C, [5]; D, [6]; E, [7]; and F, [8]. There is wide heterogeneity among the different patterns, varying from a relatively small akinetic apical area in C to a wide global akinesia in D and E. [9]
References
- ↑ Prasad A, Lerman A, Rihal CS (2008). "Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction". Am. Heart J. 155 (3): 408–17. doi:10.1016/j.ahj.2007.11.008. PMID 18294473.
- ↑ Akashi YJ, Goldstein DS, Barbaro G, Ueyama T (2008). "Takotsubo cardiomyopathy: a new form of acute, reversible heart failure". Circulation. 118 (25): 2754–62. doi:10.1161/CIRCULATIONAHA.108.767012. PMC 4893309. PMID 19106400.
- ↑ Abe Y, Kondo M, Matsuoka R, Araki M, Dohyama K, Tanio H. Assessment of clinical features in transient left ventricular apical ballooning. J Am Coll Cardiol. 2003;41:737-742.
- ↑ San Roman Sanchez D, Medina O, Jimenez F, Rodriguez JC, Nieto V. Dynamic intraventricular obstruction in acute myocardial infarction. Echocardiography. 2001;18:515-518.
- ↑ Wittstein IS, Thiemann DR, Lima JA, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med. 2005;352:539-548.
- ↑ Rivera JM, Locketz AJ, Fritz KD, et al. “Broken heart syndrome” after separation (from OxyContin). Mayo Clin Proc. 2006;81:825-828.
- ↑ Desmet WJ, Adriaenssens BF, Dens JA. Apical ballooning of the left ventricle: first series in white patients. Heart. 2003;89:1027-1031.
- ↑ Reyburn AM, Vaglio JC Jr. Transient left ventricular apical ballooning syndrome. Mayo Clin Proc. 2006;81:824.
- ↑ Ibanez B. Takotsubo Syndrome: A Bayesian Approach to Interpreting Its Pathogenesis Mayo Clin Proc. 2006; 81: 732-735