Cluster headache
Template:DiseaseDisorder infobox
|
Cluster Headache Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Cluster headache On the Web |
|
American Roentgen Ray Society Images of Cluster headache |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Synonyms and keywords: Horton syndrome; Bing-Horton neuralgia
Overview
Cluster headaches are rare, extremely painful and debilitating headaches that occur in groups or clusters. Often appearing during seasonal changes. They may also be described as suicide headaches, a reference to the excruciating pain and resulting desperation that has culminated in actual suicide.[1]
Classification of Cluster headache
International Headache Society’s classification of cluster headache:[2]
- Headache is associated with at least one of the following signs that have to be present on the pain side:
- Miosis
- Eyelid edema
- Conjunctival injection (red eyes with lacrimation)
- Rhinorrhea
- Forehead and facial sweating
- Nasal congestion
- Ptosis
- Lacrimation
- Severe unilateral, orbital, supraorbital and/or temporal pain lasting 15 to 180 min if untreated
- Frequency of attacks: from one every other day to eight in a day
- At least five attacks fulfilling number 2 and 3
Signs and symptoms
Cluster headache sufferers typically experience very severe headaches of a piercing quality near one eye or temple that last for fifteen minutes to three hours with some lasting days (rarely more than three days). The headaches are typically unilateral and rarely change sides during the same cycle (see episodic).
Pain
Persons who have experienced both cluster headaches and other painful conditions (childbirth, migraines) report that the pain of cluster headaches is far worse, significantly more severe than a migraine.[3] The pain has been described as akin to having an ice pick piercing the eye slowly but in a constant manner. Acid being poured in the head through a hole in the ear may be a better description.[4] A hot poker inserted in the eye, although gruesome, may well be the best description.[5] It has been described in medical journals as one of the most severe pain syndromes suffered by human beings.[6]
Other symptoms
A person experiencing a cluster headache may find problems sitting still and may pace or even become severely agitated.
Cluster headaches are frequently associated with Horner's syndrome:[7] ptosis (drooping eyelids), conjunctival injection (which results in red, watery eyes), lacrimation (tearing), miosis (constricted pupil), eyelid edema, nasal congestion, rhinorrhea (runny nose), and sweating on the affected side of the face. The neck is often stiff or tender in association with cluster headaches afterwards, and jaw and teeth pain are sometimes reported.
Sensitivity to light is more typical of a migraine, as is vomiting, but both can be present in some sufferers of cluster headache, although rare.
Cyclical recurrence and regular timing
Cluster headaches are occasionally referred to as "alarm clock headaches", because of the regularity of its timing and its ability to wake a person from sleep. Thus it has been known to strike at the same time each night or at a certain period after falling asleep, or at precisely the same time during the day a week later. This has prompted researchers to speculate an involvement of the brain's "biological clock" or circadian rhythm. In some cases, cluster headaches remain "steady" without cyclical ups and downs for days.
Episodic or chronic
In episodic cluster headache, these attacks occur once or more daily, often at the same times each day, for a period of several weeks, followed by a headache-free period lasting weeks, months, or years. Approximately 10–15% of cluster headache sufferers are chronic; they can experience multiple headaches every day for years.
Cluster headaches occurring in two or more cluster periods lasting from 7 to 365 days with a pain-free remission of one month or longer between the clusters are considered episodic. If the attacks occur for more than a year without a pain-free remission of at least one month, the condition is considered chronic.[8] Chronic clusters run continuously without any "remission" periods between cycles.[9] The condition may change from chronic to episodic and from episodic to chronic. Remission periods lasting for decades before the resumption of clusters have been known to occur.
Other names
Cluster headaches have been called by several other names in the past including Erythroprosopalgia of Bing, Ciliary neuralgia, Migrainous neuralgia, Erythromelagia of the head, Horton's headache (named after Bayard T. Horton, an American neurologist who was the first to accurately describe the headache in 1939[10]), Histaminic cephalalgia, Petrosal neuralgia, sphenopalatine neuralgia, Vidian neuralgia, Sluder's neuralgia, and Hemicrania angioparalyticia.[11] Sluder's neuralgia(syndrome) and cluster pain can often be temporarily stopped with nasal lidocaine spray. If successful, outpatient nasal septoplasty and splinting can resolve the condition.[12]
-

Robert Bing (1878 - 1956)
-

Bayard T. Horton (1895 - 1980)


Prevalence
While migraines are diagnosed more often in women, cluster headaches are diagnosed more often in men. The male-to-female ratio in cluster headache ranges from 4:1 to 7:1. It primarily occurs between the ages of 20 to 50 years. [3]This gap between the sexes has narrowed over the past few decades, and it is not clear whether cluster headaches are becoming more frequent in women, or whether they are merely being better diagnosed. Limited epidemiological studies have suggested prevalence rates of between 56 and 326 people per 100,000.[13]
Latitude plays a role in the occurrence of cluster headaches, which are more common as one moves away from the equator towards the poles. It is believed that greater changes in day length are responsible for the increase.
Pathophysiology
Cluster headaches are classified as vascular headaches. The intense pain is caused by the dilation of blood vessels which creates pressure on the trigeminal nerve. While this process is the immediate cause of the pain, the etiology (underlying cause or causes) is not fully understood.
-
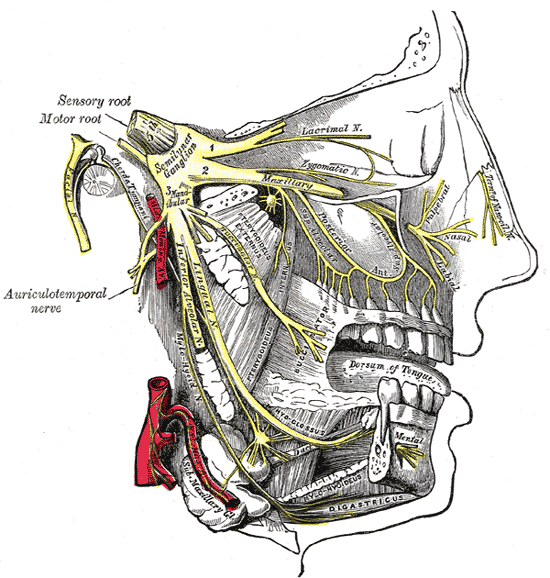
Trigeminal nerve is shown in yellow.
-
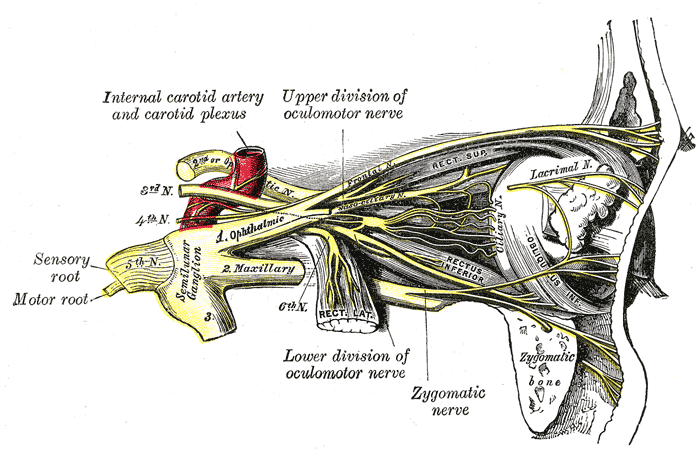
Detailed view of ophthalmic nerve, shown in yellow.


Hypothalamus
Among the most widely accepted theories is that cluster headaches are due to an abnormality in the hypothalamus; a British specialist of the disease, Dr. Goadsby has developed this theory. This can explain why cluster headaches frequently strike around the same time each day, and during a particular season, since one of the functions the hypothalamus performs is regulation of the biological clock. Metabolic abnormalities have also been reported in patients.
The hypothalamus is responsive to light—daylength and photoperiod; olfactory stimuli, including pheromones; steroids, including sex steroids and corticosteroids; neurally transmitted information arising in particular from the heart, the stomach, and the reproductive system; autonomic inputs; blood-borne stimuli, including leptin, ghrelin, angiotensin, insulin, pituitary hormones, cytokines, blood plasma concentrations of glucose and osmolarity, etc.; and stress. These particular sensitivities may underlay the causes, triggers, and methods of treatment of cluster headache.
- Neuroimaging
-

-

-

-

-

-







top row: Positron Emission Tomography (PET) shows brain areas being activated during pain
bottom row: Voxel-based morphometry (VBM) shows brain area structural differences
The above Positron emission tomography pictures indicate the brain areas which are activated during pain only, compared to the pain free periods. These pictures show brain areas which are always active during pain in yellow/orange colour (called "pain matrix"). The area in the centre (in all three views) is specifically activated during cluster headache only. The bottom row Voxel-based morphometry (VBM) pictures show structural brain differences between cluster headache patients and people without headaches. Only one area is different: This area is identical with the area of CH specific pain. This area is the hypothalamus.[14][15]
Genetics
There is a genetic component to cluster headaches, although no single gene has been identified as the cause. First-degree relatives of sufferers are more likely to have the condition than the population at large.[16] However, genetics appears to play a much smaller role in cluster headache than in some other types of headaches.
Triggers
Nitroglycerin (glyceryl trinitrate) can sometimes induce cluster headaches in sufferers in a manner similar to spontaneous attacks. Ingestion of alcohol is recognized as a common trigger of cluster headaches when a person is in cycle or susceptible. Exposure to hydrocarbons (petroleum solvents, perfume) is also recognized as a trigger for cluster headaches. Some patients have a decreased tolerance to heat, and becoming overheated may act as a trigger. Napping causes a headache for some sufferers. The role of diet and specific foods in triggering cluster headaches is controversial and not well understood.
Differential Diagnosis of Cluster headache
| Cardiovascular | • Acute hypertension • Cerebral venous thrombosis • Interior carotid artery dissection • |
| Chemical / poisoning | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | No underlying causes |
| Ear Nose Throat | • Sinusitis • |
| Endocrine | • Pheochromocytoma • |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | No underlying causes |
| Hematologic | No underlying causes |
| Iatrogenic | No underlying causes |
| Infectious Disease | • Herpes Zoster • |
| Musculoskeletal / Ortho | No underlying causes |
| Neurologic | • Chronic paroxysmal hemicrania (CPH) • Subarachnoid hemorrhage • Trigeminal Neuralgia • Cyclical migraine • Hemicrania continua • Intermittent hydrocephalus • Sleep apnea • |
| Nutritional / Metabolic | No underlying causes |
| Obstetrics and Gynecology | • Preeclampsia • |
| Oncologic | • Intracranial neoplasm • |
| Opthalmologic | • Acute optic neuritis • Acute glaucoma • |
| Overdose / Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal / Electrolyte | No underlying causes |
| Rheum / Immune / Allergy | • Temporal Arteritis • Allergen exposure • Connective tissue disorder (e.g., systemic lupus erythematosus SLE) • |
| Trauma | • Cranial trauma • |
| Miscellaneous | No underlying causes |
Treatment
Cluster headaches often go undiagnosed for many years, being confused with migraine or other causes of headache.[17]
Medically, cluster headaches are considered benign, but because of the extreme and often debilitating pain associated with them, a severe attack is nevertheless treated as a medical emergency by doctors who are familiar with the condition. Because of the relative rareness of the condition and ambiguity of the symptoms, some sufferers may not receive treatment in the emergency room and patients may even be mistaken as exhibiting drug-seeking behavior.
Over-the-counter pain medications (such as aspirin, paracetamol, and ibuprofen) typically have no effect on the pain from a cluster headache. Unlike other headaches such as migraines and tension headaches, cluster headaches do not respond to biofeedback.
Some have reported partial relief from narcotic pain killers. Percocet (Oxycodone with paracetamol) has had widespread success amongst some cluster headache patients, especially males. Anecdotal evidence indicates that cluster headaches can be so excruciating that even morphine does little to ease the pain. However, some newer medications like fentanyl (and Percocet) have shown promise in early studies and use.
Medications to treat cluster headaches are classified as either abortives or prophylactics (preventatives). In addition, short-term transitional medications (such as steroids) may be used while prophylactic treatment is instituted and adjusted. With abortive treatments often only decreasing the duration of the headache and preventing it from reaching its peak rather than eliminating it entirely, preventive treatment is always indicated for cluster headaches, to be started at the first sign of a new cluster cycle.
In many cases, some doctors have tried the use of beta blockers as a treatment.
Abortive treatment
During the onset of a cluster headache, the most rapid abortive treatment is the inhalation of pure oxygen (12-15 litres per minute in a non-rebreathing apparatus).[18] When used at the onset this can abort the attack in as little as 5 minutes. Once an attack is at its peak, oxygen therapy appears to have little effect. Alternative first-line treatment is subcutaneous administration of triptan drugs, like sumatriptan and zolmitriptan.[18] Because of the rapid onset of an attack, the triptan drugs are usually taken by subcutaneous injection rather than by mouth. While available as a nasal spray, these are seldom effective to sufferers of cluster headaches due to the swelling of the nasal passages during an attack.
Lidocaine and other topical anesthetics sprayed into the nasal cavity may relieve or stop the pain,[19] normally in a few minutes, but long term use is not suggested due to the side effects and possible damage to the nasal cavities.
Previously, vaso-constrictors such as ergot compounds were also used, and sufferers report a similar relief by taking strong cups of coffee immediately at the onset of an attack.
Sometimes, lying in a dark room will help a person if the pain is a side effect of Horner's Syndrome.
Cool showers have helped about 15% of people who try them; while not aborting the attack, they allow the body to cool and thus help to reduce the level of pain. Other abortive remedies that work for some include ice, hot showers, breathing cold air, caffeine, and drinking large amounts of water in the early stages of an attack. Vigorous exercise has been shown in some cases to be very effective in relieving and aborting an acute attack by increasing the levels of oxygen within the body. This could also be due to an increase in adrenaline and changes in blood pressure. Some people report that sexual intercourse and specifically orgasm may terminate an attack possibly by acutely modulating hypothalamic function.[20][21][22]
Prophylactic treatment
A wide variety of prophylactic medicines are in use, and patient response to these is highly variable. Current European guidelines suggest the use of the calcium channel blocker verapamil at a dose of at least 240 mg daily. Steroids, such as prednisolone, are also effective, with a high dose given for the first five days before tapering down. Methysergide, lithium and the anticonvulsant topiramate are recommended as alternative treatments.[18]
Muscle relaxants and atypical anti-psychotics have also been used.
Magnesium supplements have been shown to be of some benefit in about 40% of patients. Melatonin has also been reported to help some.
Non-established and research approaches
There is substantial anecdotal evidence that serotonergic psychedelics such as psilocybin (mushrooms) and LSD and LSA d-Lysergic acid amide (Rivea corymbosa seeds) abort cluster periods and extend remission periods.[23][24] Melatonin, psilocybin, serotonin, and the triptan abortive drugs are closely-related tryptamines.
Dr. Andrew Sewell and Dr. John Halpern at McLean Hospital in Boston have investigated the ability of low doses of psilocybin ("magic mushrooms") to treat cluster headaches. Dr. Sewell examined medical records of 53 patients who had taken hallucinogenic mushrooms and reported in Neurology that the majority of them found partial or complete relief from cluster attacks.[25] A clinical study of these treatments under the auspices of MAPS is being developed by researchers at Harvard Medical School, McLean Hospital.[26]
Within the United States, the Controlled Substances Act (CSA) of 1970 makes it illegal to possess hallucinogens (including psilocybin and LSD), classifying them as Schedule I drugs with no legitimate medical use. Patients who use psilocybin to treat their symptoms face legal prosecution, although there are no known convictions.
Other types of headache
- Chronic Paroxysmal Hemicrania (CPH) is a condition similar to cluster headache, but CPH responds well to treatment with the anti-inflammatory drug indomethacin and the attacks are very much shorter, often lasting only seconds.[27]
- Some people with extreme headaches of this nature (especially if they are not unilateral) may actually have an ictal headache. Anticonvulsant medications can significantly improve this condition so sufferers should consult a physician about this possibility.[28]
- It is also possible to have two or more different types of headaches, complicating diagnosis and treatment.
See also
- Headache
- Tension headache
- Migraine
- Rebound headache
- Hemicrania continua
- Trigeminal neuralgia
- Chronic Paroxysmal Hemicrania
- Organization for Understanding Cluster Headaches
References
- ↑ Torelli P, Manzoni G (2003). "Pain and behaviour in cluster headache. A prospective study and review of the literature". Funct Neurol. 18 (4): 205–10. PMID 15055745. Unknown parameter
|month=ignored (help) - ↑ Headache Classification Committee of the International Headache Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia 1988; 8 (Suppl 7):1–96
- ↑ Charlotte E. Grayson and The Cleveland Clinic Neuroscience Center (October 2004). "Cluster Headaches". WebMD. Retrieved 2006-09-22.
- ↑ Brian D. Loftus (2005). "Cluster Headache and Chronic Paroxysmal Hemicrania Overview". Retrieved 2006-09-22.
- ↑ Goldstein, Michael. "Cluster Headache". New Atlantean Press. 1999.
- ↑ Arne May, Anish Bahra, Christian Büchel, Richard S J Frackowiak, Peter J Goadsby; University Department of Clinical Neurology (May, Bahra, Goadsby), and Wellcome Department of Cognitive Neurology (Büchel, Frackowiak), Institute of Neurology, National Hospital for Neurology and Neurosurgery, Queen Square, London UK (1998 July 25;352(9124):275-8). "Hypothalamic activation in cluster headache attacks". The Lancet. Check date values in:
|date=(help) - ↑ Graff JM, Lee AG (February 21, 2005). "Horner's Syndrome (due to Cluster Headache): 46 y.o. man presenting with headache and ptosis". Ophthalmology Grand Rounds. The University of Iowa. Retrieved 2006-09-22.
- ↑ http://www.w-h-a.org/wha2/Newsite/resultsnav.asp?color=C2D9F2&idContentNews=751
- ↑ http://www.paralumun.com/headachecluster.htm
- ↑ http://www.mayoclinicproceedings.com/inside.asp?AID=3032&UID=
- ↑ Stephen D. Silberstein, Richard B. Lipton. Peter J. Goadsgy. "Headache in Clinical Practice." Second edition. Taylor & Francis. 2002.
- ↑ IHS ICHD2: Mucosal contact point headache
- ↑ Torelli P, Castellini P, Cucurachi L, Devetak M, Lambru G, Manzoni G (2006). "Cluster headache prevalence: methodological considerations. A review of the literature". Acta Biomed Ateneo Parmense. 77 (1): 4–9. PMID 16856701.
- ↑ May et al.: PET and MRA findings in cluster headache and MRA in experimental pain Neurology 2000;55:1328-1335, PMID 11087776.
- ↑ Dasilva AF, Goadsby PJ, Borsook D: Cluster headache: a review of neuroimaging findings. Curr Pain Headache Rep. 2007;11(2):131-6. PMID 17367592.
- ↑ Pinessi L, Rainero I, Rivoiro C, Rubino E, Gallone S (2005). "Genetics of cluster headache: an update". J Headache Pain. 6 (4): 234–6. PMID 16362673. Unknown parameter
|month=ignored (help) - ↑ "Vast Majority of Cluster Headache Patients Are Initially Misdiagnosed, Dutch Researchers Report". World Headache Alliance. 21/8/2003. Retrieved 2006-10-08. Check date values in:
|date=(help) - ↑ 18.0 18.1 18.2 May A, Leone M, Afra J, Linde M, Sándor P, Evers S, Goadsby P (2006). "EFNS guidelines on the treatment of cluster headache and other trigeminal-autonomic cephalalgias". Eur J Neurol. 13 (10): 1066–77. doi:10.1111/j.1468-1331.2006.01566.x. PMID 16987158. Unknown parameter
|month=ignored (help) Free Full Text (PDF) - ↑ Mills T, Scoggin J (1997). "Intranasal lidocaine for migraine and cluster headaches". Ann Pharmacother. 31 (7–8): 914–5. PMID 9220056. Unknown parameter
|month=ignored (help) - ↑ Ekbom K, Lindahl J (1970). "Effect of induced rise of blood pressure on pain in cluster headache". Acta Neurol Scand. 46 (4): 585–600. PMID 4994083.
- ↑ Atkinson R (1977). "Physical fitness and headache". Headache. 17 (5): 189–91. PMID 924787. Unknown parameter
|month=ignored (help) - ↑ Gotkine M, Steiner I, Biran I. (2006). "Now dear, I have a headache! Immediate improvement of cluster headaches after sexual activity". J Neurol Neurosurg Psychiatry. 77 (11): 1296. PMID 17043304. Unknown parameter
|month=ignored (help)- Abstract - ↑ "Hallucinogenic Differential Diagnosis of Cluster headache {{subst:Ddxtable_noh}} Treatment of Neuro-Vascular Headaches". ClusterBusters. Retrieved 2006-09-22. line feed character in
|title=at position 58 (help) - ↑ Mark Honigsbaum (August 2, 2005). "Headache sufferers flout new drug law - Calls for clinical trials and rethink of legislation as patients claim that magic mushrooms can relieve excruciating condition". The Guardian. Retrieved 2006-09-22. [reprint by Multidisciplinary Association for Psychedelic Studies]
- ↑ Sewell R, Halpern J, Pope H (2006). "Response of cluster headache to psilocybin and LSD". Neurology. 66 (12): 1920–2. PMID 16801660. Unknown parameter
|month=ignored (help) - a Brief Communications, also presented as:
Sewell, R. Andrew, M.D.; Halpern, John M., M.D. "The Effects Of Psilocybin And LSD On Cluster Headache: A Series Of 53 Cases." Abstract. Presented to the National Headache Foundation’s Annual Headache Research Summit. February, 2006. - ↑ "Research into psilocybin and LSD as potential treatments for people with cluster headaches". LSD and Psilocybin Research. Multidisciplinary Association for Psychedelic Studies. Retrieved 2006-09-22.
- ↑ NEURO/67 at eMedicine
- ↑ "Seizures and Headaches: They Don't Have to Go Together". Epilepsy.com. 16 September 2003. Retrieved 2006-09-22.
External links
- Algorithm for diagnosis and treatment from National Guideline Clearinghouse (DHHS)
- Clusterheadaches.com, the largest online support group for people with cluster headaches
- Organization for Understanding Cluster Headaches, a non-profit education and advocacy group
- National Headache Foundation
- American Council for Headache Education
- Cluster Busters
- Some personal stories of dealing with cluster headaches.
{kind=link}
Template:Diseases of the nervous system
de:Cluster-Kopfschmerz
hu:Cluster-fejfájás
nl:Clusterhoofdpijn
no:Clusterhodepine
sv:Hortons huvudvärk