Crohn's disease
| Crohn's disease | |
 | |
|---|---|
| The three most common sites of intestinal involvement in Crohn's disease are ileal, ileocolic and colonic.[1] | |
| ICD-10 | K50 |
| ICD-9 | 555 |
| OMIM | 266600 |
| DiseasesDB | 3178 |
| MedlinePlus | 000249 |
| MeSH | D003424 |
|
Crohn's disease |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Crohn's disease On the Web |
|
American Roentgen Ray Society Images of Crohn's disease |
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Synonyms and keywords: Regional enteritis
Overview
Historical Perspective
Classification
Pathophysiology
Causes
Differential Diagnosis
Risk Factors
Natural History, Complications and Prognosis
Diagnosis
History and Symptoms | Physical Examination | Laboratory tests | ECG | Chest X Ray |CT | MRI | Echocardiography or Ultrasound |Other imaging studies | Alternative diagnostics
Treatment
Medical therapy | Surgical options | Prevention | Financial costs| Future therapies



Images shown below are courtesy of RadsWiki and copylefted
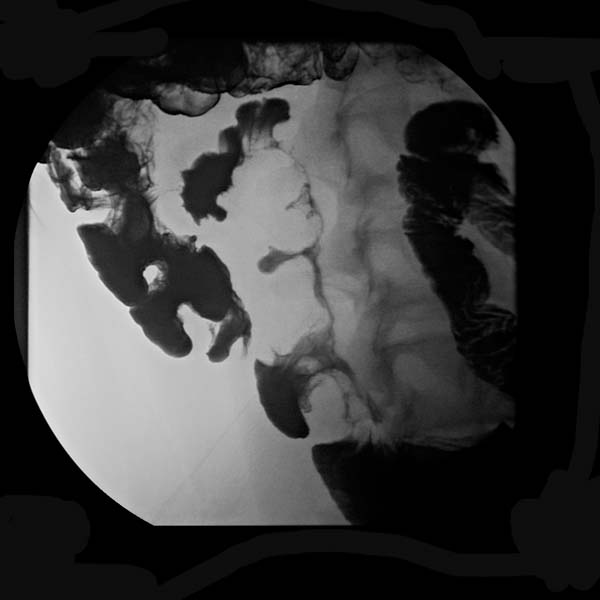
-

Abdominal x-ray of a patient with Crohn disease
-

Pseudosacculations in Crohn's disease
-

Pseudosacculations in Crohn's disease
-
Pseudosacculations in Crohn's disease




-
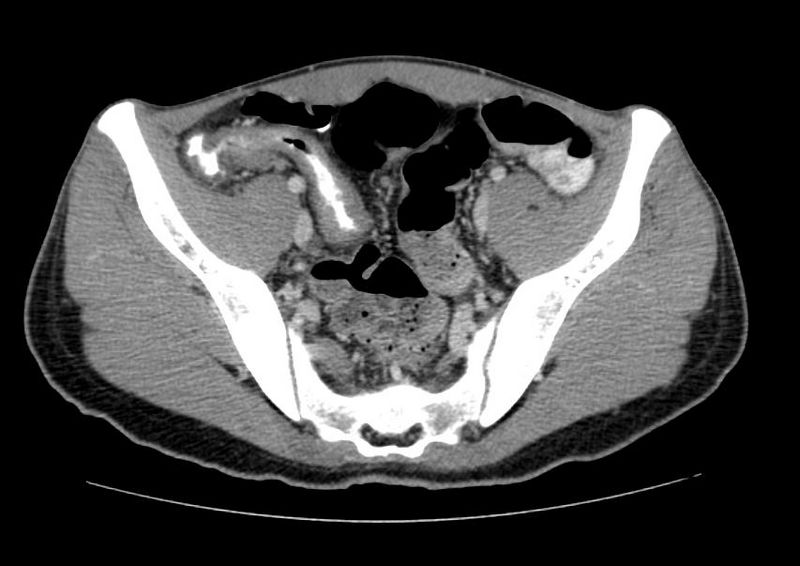
Active Crohn's disease CT
-

Active Crohn's disease MRI
-
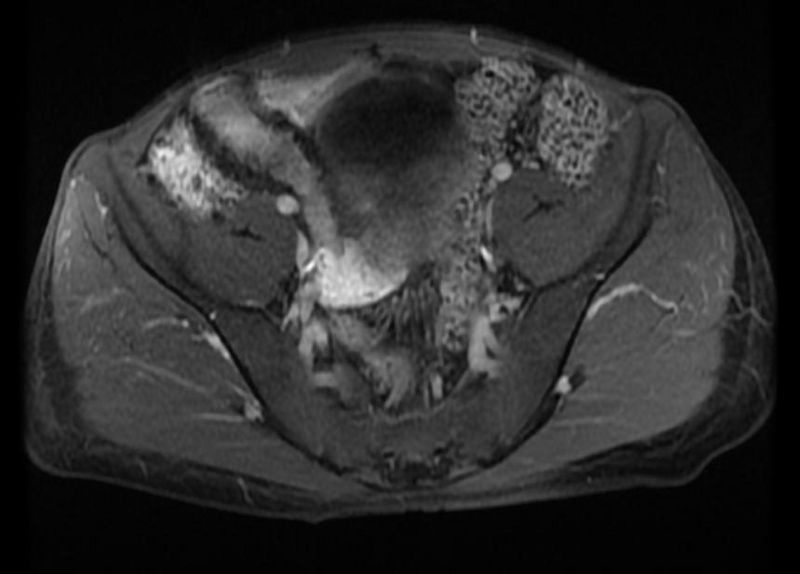
Active Crohn's disease MRI
-

Active Crohn's disease small bowel series
-
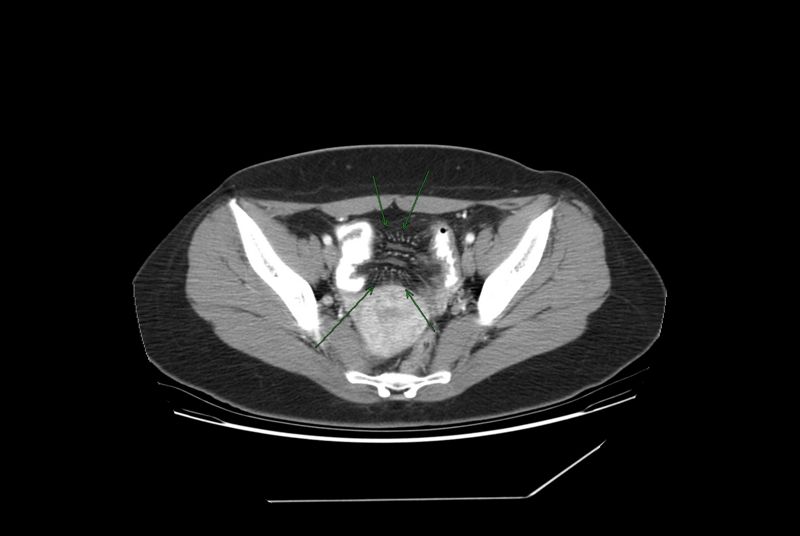
Comb sign in Crohn's disease





Treatment
Treatment is only needed for people exhibiting symptoms. The therapeutic approach to Crohn's disease is sequential: to treat acute disease and then to maintain remission. Treatment initially involves the use of medications to treat any infection and to reduce inflammation. This usually involves the use of aminosalicylate anti-inflammatory drugs and corticosteroids, and may include antibiotics.
Once remission is induced, the goal of treatment becomes maintaining remission and avoiding flares. Because of side-effects, the prolonged use of corticosteroids must be avoided. Although some people are able to maintain remission with aminosalicylates alone, many require immunosuppressive drugs.[2]
On 14 January 2008 the U.S. Food and Drug Administration approved natalizumab (Tysabri) for both induction of remission and maintenance of remission in Crohns. Natalizumab is humanised monoclonal antibody (MAb), and the first alpha-4 antagonist in a new class of agents called selective adhesion-molecule (SAM) inhibitors. Alpha-4 integrin is required for leukocytes to adhere to the walls of blood vessels and migrate into the gut; natalizumab prevents leukocytes from doing that. Natalizumab was previously approved for multiple sclerosis. However, because it suppresses the immune system, natalizumab has been linked to a very rare adverse effect that is usually fatal if undetected. Leukocytes also protect the body from viruses, and 2 patients on natalizumab, who were also receiving other immuno-suppressive drugs (Avonex and Immuran), died of a rare brain infection, progressive multifocal leukoencephalopathy. Because of this danger, patients must be in a special monitoring program, and natalizumab is given as a mono-therapy.[3].As of late December 2007, more than 21,000 MS patients were receiving natalizumab mono-therapy without a single incidence of PML occurring.[4].
Surgery may be required for complications such as obstructions, fistulas and/or abscesses, or if the disease does not respond to drugs within a reasonable time. For patients with an obstruction due to a stricture, two options for treatment are strictureplasty and resection of that portion of bowel. According to a retrospective review at the Cleveland Clinic, there is no statistical significance between strictureplasty alone versus strictureplasty and resection specifically in cases of duodenal involvement. In these cases, re-operation rates were 31% and 27%, respectively, indicating that strictureplasty is a safe and effective treatment for selected patients with duodenal involvement.[5]
Recent studies using Helminthic therapy or Hookworms to treat Crohn's Disease and other (non-viral) auto-immune diseases seem to yield promising results.[6][7][8]
See also
References
- ↑
- ↑
- ↑ "FDA Approves Tysabri to Treat Moderate-to-Severe Crohn's Disease" (Press release). U.S. Food and Drug Administration. 2008-01-14. Retrieved 2008-01-16.
- ↑ .http://www.elan.com/News/full.asp?ID=1091942
- ↑ Ozuner G, Fazio VW, Lavery IC, Milsom JW, Strong SA (1996). "Reoperative rates for Crohn's disease following strictureplasty. Long-term analysis". Dis. Colon Rectum. 39 (11): 1199–203. PMID 8918424.
- ↑ British Medical Journal A proof of concept study establishing Necator americanus in Crohn’s patients and reservoir donors
- ↑ Daily Mail. The bloodsucking worm that fights allergies from inside your tummy 14-09-2007.
- ↑ How to cure your asthma or hayfever using hookworm - a practical guide. 01-05-2006.
Template:Crohn's Template:Gastroenterology