Netupitant and palonosetron
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aparna Vuppala, M.B.B.S. [2]
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Overview
Netupitant and palonosetron is an antiemetic that is FDA approved for the prophylaxis of acute and delayed nausea and vomiting associated with initial and repeat courses of cancer chemotherapy. Common adverse reactions include erythema, constipation , indigestion , asthenia , headache , fatigue ,serotonin syndrome..
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Nausea and Vomiting associated with highly emetogenic Chemotherapy
- Netupitant and Palonosetron is indicated for the prevention of acute and delayed nausea and vomiting associated with initial and repeat courses of cancer chemotherapy, including, but not limited to, highly emetogenic chemotherapy. Netupitant and Palonosetron is an oral fixed combination of palonosetron and netupitant: palonosetron prevents nausea and vomiting during the acute phase and netupitant prevents nausea and vomiting during both the acute and delayed phase after cancer chemotherapy.
Dosing Information
Highly Emetogenic Chemotherapy, including Cisplatin Based Chemotherapy
- The recommended dosage in adults is one capsule of Netupitant and Palonosetron administered approximately 1 hour prior to the start of chemotherapy with dexamethasone 12 mg administered orally 30 minutes prior to chemotherapy on day 1 and 8 mg orally once daily on days 2 to 4 .
Anthracyclines and Cyclophosphamide Based Chemotherapy and Chemotherapy Not Considered Highly Emetogenic
- The recommended dosage in adults is one capsule of Netupitant and Palonosetron approximately 1 hour prior to the start of chemotherapy with dexamethasone 12 mg administered orally 30 minutes prior to chemotherapy on day 1. Administration of dexamethasone on days 2 to 4 is not necessary .
- Netupitant and Palonosetron can be taken with or without food.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Netupitant and Palonosetron in adult patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Netupitant and Palonosetron in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Netupitant and Palonosetron in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Netupitant and Palonosetron in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Netupitant and Palonosetron in pediatric patients.
Contraindications
- None.
Warnings
Hypersensitivity
- Hypersensitivity reactions, including anaphylaxis, have been reported with or without known hypersensitivity to other 5-HT3 receptor antagonists.
Serotonin Syndrome
- The development of serotonin syndrome has been reported with 5-HT3 receptor antagonists. Most reports have been associated with concomitant use of serotonergic drugs (e.g., selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), monoamine oxidase inhibitors, mirtazapine, fentanyl, lithium, tramadol, and intravenous methylene blue). Some of the reported cases were fatal. Serotonin syndrome occurring with overdose of another 5-HT3 receptor antagonist alone has also been reported. The majority of reports of serotonin syndrome related to 5-HT3 receptor antagonist use occurred in a post-anesthesia care unit or an infusion center.
- Symptoms associated with serotonin syndrome may include the following combination of signs and symptoms: mental status changes (e.g., agitation, hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile blood pressure, dizziness, diaphoresis, flushing, and hyperthermia), neuromuscular symptoms(e.g., tremor, rigidity, myoclonus, hyperreflexia, and incoordination), seizures, with or without gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea). Patients should be monitored for the emergence of serotonin syndrome, especially with concomitant use of Netupitant and Palonosetron and other serotonergic drugs. If symptoms of serotonin syndrome occur, discontinue Netupitant and Palonosetron and initiate supportive treatment. Patients should be informed of the increased risk of serotonin syndrome, especially if Netupitant and Palonosetron is used concomitantly with other serotonergic drugs
Adverse Reactions
Clinical Trials Experience
Clinical Trials Experience
- Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
- The overall safety of Netupitant and Palonosetron was evaluated in 1538 cancer patients and healthy volunteers in clinical trials. The data described below reflect exposure to Netupitant and Palonosetron in 1169 cancer patients, receiving at least one cycle of cancer chemotherapy in 3 active-controlled trials [see Clinical Studies (14)], including 782 exposed to Netupitant and Palonosetron for at least 4 cycles and 321 exposed for at least 6 cycles, up to a maximum of 12 cycles of chemotherapy. The median age was 55, 79% were female, 83% were White, 13% were Asian, and 4% were Hispanic. All patients received a single oral dose of Netupitant and Palonosetron 1 hour prior to the start of each chemotherapy cycle. In all studies, dexamethasone was co-administered with Netupitant and Palonosetron.
Cisplatin Based Highly Emetogenic Chemotherapy
- In a single-cycle study of patients receiving cisplatin-based highly emetogenic chemotherapy, 136 patients were treated with Netupitant and Palonosetron. Table 1 shows adverse reactions defined as adverse events reported at an incidence of at least 3% and for which the Netupitant and Palonosetron rate exceeded palonosetron alone

Anthracyclines and Cyclophosphamide Based Chemotherapy
- In a study of patients receiving anthracycline and cyclophosphamide based chemotherapy, 725 patients were treated with Netupitant and Palonosetron during Cycle 1, and 635 of these patients continued for up to 8 cycles in a multiple-cycle extension. Table 2 shows adverse reactions defined as adverse events reported at an incidence of at least 3% and for which the Netupitant and Palonosetron rate exceeded palonosetron alone during Cycle 1. The adverse reaction profile in subsequent cycles was similar to that observed in Cycle 1.

- In a multi-cycle safety study of 412 patients, the safety profile of Netupitant and Palonosetron (n = 308) was comparable to aprepitant and palonosetron (n = 104) in patients undergoing initial and repeat cycles (median 5 cycles, range of 1-14 cycles) of chemotherapy, including carboplatin, cisplatin, oxaliplatin, and doxorubicin regimens. There were no reports of concomitant elevations of transaminases > 3 x ULN and total bilirubin in this study in either arm.
- In a randomized, clinical non-inferiority study, that compared oral palonosetron 0.5 mg to intravenous palonosetron 0.25 mg in cancer patients scheduled to receive highly emetogenic cisplatin (>70 mg/m2) based chemotherapy, there were two patients (0.5%; 2/369) in the intravenous palonosetron arm who had concomitant elevations of transaminases and total bilirubin. Neither experienced transaminase elevations of > 10 x ULN.
Postmarketing Experience
There is limited information regarding Postmarketing Experience of Netupitant and Palonosetron in the drug label.
Drug Interactions
Effects of Netupitant and Palonosetron on Other Drugs
Interaction with CYP3A4 Substrates
- Netupitant, a component of Netupitant and Palonosetron, is a moderate inhibitor of CYP3A4.
- Netupitant and Palonosetron should be used with caution in patients receiving concomitant medications that are primarily metabolized through CYP3A4. The plasma concentrations of CYP3A4 substrates can increase when co-administered with Netupitant and Palonosetron. The inhibitory effect on CYP3A4 can last for multiple days.
Dexamethasone
- A two-fold increase in the systemic exposure of dexamethasone was observed 4 days after single dose of netupitant. The duration of the effect was not studied beyond 4 days. Administer a reduced dose of dexamethasone with Netupitant and Palonosetron
Midazolam
- When administered with netupitant, the systemic exposure to midazolam was significantly increased. Consider the potential effects of increased plasma concentrations of midazolam or other benzodiazepines metabolized via CYP3A4 (alprazolam, triazolam) when administering these drugs with Netupitant and Palonosetron.
Interaction with chemotherapeutic agents
- The systemic exposure of chemotherapy agents metabolized by CYP3A4 can increase when administered with Netupitant and Palonosetron. Chemotherapy agents that are known to be metabolized by CYP3A4 include docetaxel, paclitaxel, etoposide, irinotecan, cyclophosphamide, ifosfamide, imatinib, vinorelbine, vinblastine, and vincristine . Caution and monitoring for chemotherapeutic related adverse reactions are advised in patients receiving chemotherapy agents metabolized primarily by CYP3A4.
Interaction with oral contraceptives
- Clinically significant effect of Netupitant and Palonosetron on the efficacy of oral contraceptives containing levonorgestrel and ethinyl estradiol is unlikely.
Effects of Other Drugs on Netupitant and Palonosetron
- Netupitant, a component of Netupitant and Palonosetron, is mainly metabolized by CYP3A4 .
- In vitro metabolism studies have suggested that CYP2D6 and to a lesser extent CYP3A4 and CYP1A2 are involved in the metabolism of palonosetron.
CYP3A4 Inducers
- Avoid concomitant use of Netupitant and Palonosetron in patients who are chronically using a strong CYP3A4 inducer such as rifampin. A strong CYP3A inducer can decrease the efficacy of Netupitant and Palonosetron by substantially reducing plasma concentrations of the netupitant component
CYP3A4 Inhibitors
- Concomitant use of Netupitant and Palonosetron with a strong CYP3A4 inhibitor (e.g., ketoconazole) can significantly increase the systemic exposure to the netupitant component of Netupitant and Palonosetron. However, no dosage adjustment is necessary for single dose administration of Netupitant and Palonosetron
Serotonergic Drugs
- Serotonin syndrome (including altered mental status, autonomic instability, and neuromuscular symptoms) has been described following the concomitant use of 5-HT3 receptor antagonists and other serotonergic drugs, including selective serotonin reuptake inhibitors (SSRIs) and serotonin and noradrenaline reuptake inhibitors (SNRIs)
Use in Specific Populations
Pregnancy
Risk Summary
- Adequate and well-controlled studies with Netupitant and Palonosetron have not been conducted in pregnant women. In animal reproduction studies, no effects on embryo-fetal development were observed following daily administration of netupitant in pregnant rats during the period of organogenesis at doses up to 3.7 times the human AUC (area under the plasma concentration-time curve) at the recommended single human dose to be given with each cycle of chemotherapy. However, a dose-dependent increase in adverse effects on embryo-fetal development was observed following daily administration of netupitant in pregnant rabbits during the period of organogenesis with doses at least 0.2 times the human AUC at the recommended single human dose to be given with each cycle of chemotherapy. Daily administration of netupitant in rats up to 3.7 times the human AUC at the recommended human dose during organogenesis through lactation produced no adverse effects in the offspring. In animal reproduction studies with palonosetron, no effects on embryo-fetal development were observed following oral administration during the period of organogenesis at doses up to 921 and 1841 times the recommended human oral dose in rats and rabbits, respectively. Netupitant and Palonosetron should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Animal Data
- Daily administration of up to 30 mg/kg netupitant in rats (3.7 times the human AUC at the recommended single human dose to be given with each cycle of chemotherapy) during the period of organogenesis produced no effects on embryo-fetal development. However, an increased incidence of external and skeletal abnormalities in rabbit fetuses was observed following daily administration of netupitant in rabbits at 10 mg/kg/day and higher (0.2 times the human AUC at the recommended single human dose to be given with each cycle of chemotherapy) during the period of organogenesis. These abnormalities included positional abnormalities in the limbs and paws, and fused sternebrae. Reduction in fetal rabbit weight occurred at 30 mg/kg/day. Maternal toxicity in rabbits (i.e., loss of bodyweight during the treatment period) was also observed at 30 mg/kg/day. Daily administration of up to 30 mg/kg netupitant (3.7 times the human AUC at the recommended human dose) in rats during organogenesis through lactation produced no adverse effects in the offspring.
- In animal reproduction studies with palonosetron, no effects on embryo-fetal development were observed in pregnant rats given oral doses up to 60 mg/kg/day (921 times the recommended human oral dose based on body surface area) or pregnant rabbits given oral doses up to 60 mg/kg/day (1841 times the recommended human oral dose based on body surface area) during the period of organogenesis.
Pregnancy Category (AUS):
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Netupitant and Palonosetron in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Netupitant and Palonosetron during labor and delivery.
Nursing Mothers
- It is not known whether Netupitant and Palonosetron is present in human milk. Because many drugs are present in human milk and because of the potential for tumorigenicity shown for palonosetron in the rat carcinogenicity study , a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use
- Safety and effectiveness in patients below the age of 18 years have not been established.
Geriatic Use
- Of the 1169 adult cancer patients treated with Netupitant and Palonosetron in clinical studies, 18% were aged 65 and over, while 2% were aged 75 years and over. The nature and frequency of adverse reactions were similar in elderly and younger patients. Exploratory analyses of the impact of age on efficacy were performed in the two trials that compared Netupitant and Palonosetron to palonosetron . In Study 1 in patients treated with cisplatin chemotherapy, among the patients less than age 65 years, 115 were treated with Netupitant and Palonosetron and 116 were treated with palonosetron alone. Among the patients 65 years or older, 20 were treated with Netupitant and Palonosetron and 20 were treated with palonosetron alone. The difference in Complete Response (CR) rates between Netupitant and Palonosetron and palonosetron alone was similar between the two age groups in both the acute and delayed phases. In Study 2 in patients treated with anthracyclines plus cyclophosphamide chemotherapy, among the patients less than age 65 years, 608 were treated with Netupitant and Palonosetron and 602 were treated with palonosetron alone. Among the patients 65 years or older, 116 were treated with Netupitant and Palonosetron and 123 were treated with palonosetron alone. The difference in CR rates between Netupitant and Palonosetron and palonosetron alone (4% in <65 years and 2% in >65 years) was similar between the two age groups in the acute phase. In the delayed phase, the difference in CR rates between Netupitant and Palonosetron and palonosetron alone (9% in <65 years and 1% in ≥ 65 years) was numerically higher in patients <65 years. This difference between age groups in the delayed phase of Study 2 may be explained, in part, by higher CR in the delayed phase associated with palonosetron alone in the older age group (81%) relative to the younger patients treated with palonosetron alone (67%).
- In general, use caution when dosing elderly patients as they have a greater frequency of decreased hepatic, renal or cardiac function and concomitant disease or other drug therapy.
Gender
There is no FDA guidance on the use of Netupitant and Palonosetron with respect to specific gender populations.
Race
There is no FDA guidance on the use of Netupitant and Palonosetron with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Netupitant and Palonosetron in patients with renal impairment.
Hepatic Impairment
- No dosage adjustment for Netupitant and Palonosetron is necessary for patients with mild to moderate hepatic impairment (Child-Pugh score 5 to 8). Limited data are available with Netupitant and Palonosetron in patients with severe hepatic impairment (Child-Pugh score >9). Avoid use of Netupitant and Palonosetron in patients with severe hepatic impairment.
Females of Reproductive Potential and Males
- No dosage adjustment for Netupitant and Palonosetron is necessary in patients with mild to moderate renal impairment. The pharmacokinetics and safety of netupitant has not been studied in patients with severe renal impairment, although severe renal impairment did not substantially affect pharmacokinetics of palonosetron. The pharmacokinetics for netupitant and palonosetron was not studied in patients with end-stage renal disease requiring hemodialysis. Avoid use of Netupitant and Palonosetron in patients with severe renal impairment or end-stage renal disease
Immunocompromised Patients
There is no FDA guidance one the use of Netupitant and Palonosetron in patients who are immunocompromised.
Administration and Monitoring
Administration
- Oral
Monitoring
There is limited information regarding Monitoring of Netupitant and Palonosetron in the drug label.
IV Compatibility
There is limited information regarding IV Compatibility of Netupitant and Palonosetron in the drug label.
Overdosage
- No specific information is available on the treatment of overdosage with Netupitant and Palonosetron. In the event of overdose, Netupitant and Palonosetron should be discontinued and general supportive treatment and monitoring should be provided. Because of the antiemetic activity of Netupitant and Palonosetron, drug-induced emesis may not be effective. Dialysis studies have not been performed; due to the large volume of distribution, dialysis is unlikely to be an effective treatment for Netupitant and Palonosetron overdose.
- A total of 33 adult cancer patients were administered oral palonosetron at a dose of 90 μg/kg (equivalent to 6 mg fixed dose), as part of a dose ranging study. This is approximately 12 times the recommended oral dose of 0.5 mg palonosetron. This dose group had a similar incidence of adverse events compared to the other dose groups and no dose response effects were observed. The highest dose of netupitant administered to 1169 cancer patients was 300 mg. The highest dose of netupitant administered to 49 healthy subjects was 400 mg. A similar incidence of adverse events was observed when compared to lower doses of netupitant in the respective populations of cancer patients and healthy subjects.
Pharmacology

Mechanism of Action
- Netupitant is a selective antagonist of human substance P/neurokinin 1 (NK1) receptors.
- Palonosetron is a 5-HT3 receptor antagonist with a strong binding affinity for this receptor and little or no affinity for other receptors. Cancer chemotherapy may be associated with a high incidence of nausea and vomiting, particularly when certain agents, such as cisplatin, are used. 5-HT3 receptors are located on the nerve terminals of the vagus in the periphery and centrally in the chemoreceptor trigger zone of the area postrema. Chemotherapeutic agents produce nausea and vomiting by stimulating the release of serotonin from the enterochromaffin cells of the small intestine. Serotonin then activates 5-HT3 receptors located on vagal afferents to initiate the vomiting reflex. The development of acute emesis is known to depend on serotonin and its 5-HT3 receptors have been demonstrated to selectively stimulate the emetic response.
- Delayed emesis has been largely associated with the activation of tachykinin family neurokinin 1 (NK1) receptors (broadly distributed in the central and peripheral nervous systems) by substance P. As shown in in vitro and in vivo studies, netupitant inhibits substance P mediated responses.
Structure
- Netupitant and Palonosetron (300 mg netupitant/0.5 mg palonosetron) is an oral fixed combination product of netupitant, a substance P/neurokinin 1 (NK1) receptor antagonist, and palonosetron hydrochloride, a serotonin-3 (5-HT3) receptor antagonist. Both netupitant and palonosetron hydrochloride are anti-nausea and anti-emetic agents.
- Netupitant is chemically described: 2-[3,5-bis(trifluoromethyl)phenyl]-N, 2 dimethyl-N-[4-(2-methylphenyl)-6-(4-methylpiperazin-1-yl)pyridin-3-yl] propanamide. The empirical formula is C30H32F6N4O, with a molecular weight of 578.61. Netupitant exists as a single isomer and has the following structural formula:
This image is provided by the National Library of Medicine.

- Palonosetron hydrochloride is chemically described: (3aS)-2-[(S)-1-Azabicyclo [2.2.2]oct-3-yl]-2,3,3a,4,5,6-hexahydro-1-oxo-1H-benz[de]isoquinoline hydrochloride. The empirical formula is C19H24N2O.HCl, with a molecular weight of 332.87. Palonosetron hydrochloride exists as a single isomer and has the following structural formula:
This image is provided by the National Library of Medicine.

- Netupitant is white to off-white crystalline powder. It is freely soluble in toluene and acetone, soluble in isopropanol and ethanol, and very slightly soluble in water.
- Palonosetron hydrochloride is a white to off-white crystalline powder. It is freely soluble in water, soluble in propylene glycol, and slightly soluble in ethanol and 2-propanol.
- Each Netupitant and Palonosetron (300 mg netupitant/0.5 mg palonosetron) capsule is composed of one white-caramel hard gelatin capsule which contains three tablets each containing 100 mg netupitant and one gelatin capsule containing 0.56 mg palonosetron hydrochloride (equivalent to 0.50 mg palonosetron). The inactive ingredients are microcrystalline cellulose, sucrose fatty acid esters, povidone K-30, croscarmellose sodium, purified water, silicon dioxide, sodium stearyl fumarate, magnesium stearate, mono- and di-glycerides of capryl/capric acid, glycerin, polyglyceryl oleate, butylated hydroxyanisole (BHA), gelatin, sorbitol, titanium dioxide, yellow iron oxide, and red iron oxide. It may contain traces of medium-chain triglycerides, lecithin, and denatured ethanol.
Pharmacodynamics
NK1 Receptor Occupancy
- The receptor occupancy for the CINV dosing regimen of netupitant was measured in a human Positron Emission Tomography (PET) study. Netupitant was shown to cross the blood brain barrier with a NK1receptor occupancy of 92.5%, 86.5%, 85.0%, 78.0%, and 76.0% in striatum at 6, 24, 48, 72, and 96 hours, respectively, after administration of 300 mg netupitant.
Cardiac Electrophysiology
- Co-administration of single dose netupitant 400 mg and palonosetron 1.5 mg had no significant effects on the QTc interval.
Pharmacokinetics
- After single dose administration of Netupitant and Palonosetron in healthy subjects, the peak plasma concentrations for netupitant and palonosetron were reached in about 5 hours.

- When administered under fed condition, the systemic exposure to netupitant and palonosetron was similar to those obtained under fasting condition.
- In cancer patients who received a single dose of Netupitant and Palonosetron 1 hour prior to chemotherapy (docetaxel, etoposide, or cyclophosphamide), the Cmax and AUC of netupitant and its metabolites were similar to those in healthy subjects. The mean Cmax and AUC of palonosetron in cancer patients were similar to those in healthy subjects.
- No significant changes in pharmacokinetics of netupitant and palonosetron were observed when 450 mg oral netupitant and 0.75 mg oral palonosetron were co-administered.
Netupitant
Absorption
- Upon oral administration of a single dose of netupitant, netupitant started to be measurable in plasma between 15 minutes and 3 hours after dosing. Plasma concentrations reached Cmax in approximately 5 hours. There was a greater than dose-proportional increase in the systemic exposure with the dose increase from 10 mg to 300 mg and a dose-proportional increase in systemic exposure with a dose increase from 300 mg to 450 mg.
Distribution
- In cancer patients netupitant disposition was characterized by a large apparent volume of distribution (Vz/F: 1982 ± 906 L) (mean ± SD). Human plasma protein binding of netupitant is greater than 99.5% at drug concentrations ranging from 10-1300 ng/mL and protein binding of its major metabolites (M1, M2 and M3) is greater than 97% at drug concentrations ranging from 100 to 2000 ng/mL.
Metabolism
- Once absorbed, netupitant is extensively metabolized to form three major metabolites: desmethyl derivative, M1; N-oxide derivative, M2; and OH-methyl derivative, M3. Metabolism is mediated primarily by CYP3A4 and to a lesser extent by CYP2C9 and CYP2D6. Metabolites M1, M2 and M3 were shown to bind to the substance P/neurokinin 1 (NK1) receptor.
- Mean Cmax was approximately 11%, 47% and 16% of netupitant for metabolites M1, M2 and M3, respectively. Mean AUC for metabolites M1, M2 and M3 was 29%, 14% and 33% of netupitant, respectively. The median tmax for metabolite M2 was 5 hours and was about 17-32 hours for metabolites M1 and M3.
Elimination
- Netupitant is eliminated from the body in a multi-exponential fashion, with an apparent elimination half-life in cancer patients of 80 ± 29 hours (mean ± SD) and with an estimated systemic clearance of 20.3 ± 9.2 L/h (mean ± SD) after a single oral dose of Netupitant and Palonosetron.
- After a single oral administration of [14C]-netupitant, approximately half the administered radioactivity was recovered from urine and feces within 120 hours of dosing. The total of 3.95% and 70.7% of the radioactive dose was recovered in the urine and feces collected over 336 hours, respectively, and the mean fraction of an oral dose of netupitant excreted unchanged in urine is less than 1% suggesting renal clearance is not a significant elimination route for the netupitant-related entities. About 86.5% and 4.7% of administered radioactivity was estimated to be excreted via the feces and urine in 30 days post-dose
Palonosetron
Absorption
- Following oral administration, palonosetron is well absorbed with its absolute bioavailability reaching 97%. After single oral doses using buffered solution mean maximum palonosetron concentrations (Cmax) and area under the concentration-time curve (AUC0-∞) were dose proportional over the dose range of 3.0 to 80 µg/kg in healthy subjects.
Distribution
- Palonosetron has a volume of distribution of approximately 8.3 ± 2.5 L/kg. Approximately 62% of palonosetron is bound to plasma proteins.
Metabolism
- Palonosetron is eliminated by multiple routes with approximately 50% metabolized to form two primary metabolites: N-oxide-palonosetron and 6-S-hydroxy-palonosetron. These metabolites each have less than 1% of the 5-HT3 receptor antagonist activity of palonosetron. In vitro metabolism studies have suggested that CYP2D6 and to a lesser extent CYP3A4 and CYP1A2 are involved in the metabolism of palonosetron. However, clinical pharmacokinetic parameters are not significantly different between poor and extensive metabolizers of CYP2D6 substrates.
Elimination
- Following administration of a single oral 0.75 mg dose of [14C]-palonosetron to six healthy subjects, 85% to 93% of the total radioactivity was excreted in urine, and 5% to 8% was eliminated in feces. The amount of unchanged palonosetron excreted in the urine represented approximately 40% of the administered dose. In cancer patients, t½ was 48 ± 19 hours. After a single-dose of approximately 0.75 mg intravenous palonosetron, the total body clearance of palonosetron in healthy subjects was 160 ± 35 mL/h/kg (mean ± SD) and renal clearance was 66.5 ± 18.2 mL/h/kg.
Specific Populations
Gender
- In a pooled analysis, the Cmax for netupitant was 35% higher in females than in males while the AUC was similar between males and females. In female subjects, the mean AUC for palonosetron was 35% higher and the mean Cmax was 26% higher than in male subjects.
Geriatrics
- In cancer patients receiving Netupitant and Palonosetron, population PK analysis indicated that age (within the range of 29 to 75 years old) did not influence the pharmacokinetics of netupitant or palonosetron. In healthy elderly subjects (>65 years old) the mean AUC0-∞ and Cmax was 25% and 36% higher, respectively, for netupitant, and 37% and 10% higher, respectively, for palonosetron compared to those in healthy younger adults (22-45 years old).
Hepatic Impairment
- The effects of hepatic impairment on the PK of netupitant and palonosetron were studied following administration of a single oral dose of Netupitant and Palonosetron to patients with mild (Child-Pugh score 5 to 6), moderate (Child-Pugh score 7 to 9), or severe (Child-Pugh score >9) hepatic impairment.
- In patients with mild or moderate hepatic impairment, the mean AUC0-∞ of netupitant was 67% and 86% higher, respectively, than in healthy subjects and the mean Cmax for netupitant was about 40% and 41% higher, respectively, than in healthy subjects.
- In patients with mild or moderate hepatic impairment, the mean AUC0-∞ of palonosetron was 33% and 62% higher, respectively, than in healthy subjects and the mean Cmax for palonosetron was about 14% higher and unchanged, respectively, than in healthy subjects.
- The pharmacokinetics of netupitant and palonosetron was available from only two patients with severe hepatic impairment. As such the data are too limited to draw a conclusion.
Renal Impairment
- In a population PK analysis, mild and moderate renal impairment did not significantly affect the pharmacokinetics of netupitant in cancer patients. Netupitant has not been studied in patients with severe renal impairment.
- Mild to moderate renal impairment does not significantly affect palonosetron pharmacokinetic parameters. In a study with intravenous palonosetron, total systemic exposure to palonosetron increased by approximately 28% in patients with severe renal impairment relative to healthy subjects.
- The pharmacokinetics of either palonosetron or netupitant has not been studied in subjects with end-stage renal disease.
Drug Interactions:
- In vitro studies have shown that netupitant and its metabolite M1 are inhibitors of CYP3A4. An in vivo study has confirmed that netupitant is a moderate inhibitor of CYP3A4.
- Based on the in vitro studies, netupitant and its metabolites’ are unlikely to have in vivo drug-drug interaction via inhibition of CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, and CYP2D6 at the clinical dose of 300 mg.
- Netupitant and its metabolites, M1, M2 and M3, are not inducers of CYP1A2, CYP2C9, CYP2C19 and CYP3A4. Their induction potential of CYP2B6 is unknown.
- Based on in vitro studies, netupitant is an inhibitor of P-gp and BCRP transporters. In addition, metabolite M2 is a substrate for P-gp. Netupitant’s potential for being a substrate for P-gp is unknown.In vitro studies indicate that netupitant and its three major metabolites are unlikely to have in vivodrug-drug interactions with human efflux transporters BSEP, MRP2, and human uptake transporters OATP1B1, OATP1B3, OAT1, OAT3, OCT1, and OCT2 at the clinical dose of 300 mg.
- In vitro studies, palonosetron does not inhibit CYP1A2, CYP2A6, CYP2B6, CYP2C9, CYP2D6, CYP2E1 and CYP3A4/5 or induce CYP1A2, CYP2D6 or CYP3A4/5. CYP2C19 was not investigated.
- Co-administration of a single dose of netupitant (300 mg) with a dexamethasone regimen (20 mg on Day 1, followed by 8 mg b.i.d. from Day 2 to Day 4) significantly increased exposure to dexamethasone. When netupitant was co-administered on Day 1, the mean AUC of dexamethasone was increased by 1.7-fold on Day 1 and up to 2.4-fold on Day 2 and Day 4.
- Chemotherapeutic Agents (docetaxel, etoposide, cyclophosphamide)
- Systemic exposure to intravenously administered chemotherapeutic agents that are metabolized by CYP3A4 was higher when Netupitant and Palonosetron was co-administered than when palonosetron alone was co-administered in cancer patients.
- With co-administration of Netupitant and Palonosetron the mean Cmax and AUC of docetaxel were 49% and 35% higher, respectively, and mean Cmax and AUC of etoposide were increased by 10% and 28%, respectively, compared to when co-administered with palonosetron alone.
- Mean Cmax and AUC for cyclophosphamide after co-administration with Netupitant and Palonosetron was 27% and 20% higher compared to when co-administered with palonosetron alone.
- The mean AUC of palonosetron was about 65% higher when Netupitant and Palonosetron was co-administered with docetaxel than with etoposide or cyclophosphamide, while the mean AUC of netupitant was similar among groups that received docetaxel, etoposide, or cyclophosphamide.
- When 500 mg erythromycin was co-administered with netupitant 300 mg, the systemic exposure of erythromycin was highly variable and the mean Cmax and AUC of erythromycin were increased by 92% and 56%, respectively.
- Oral Contraceptives
- Single dose Netupitant and Palonosetron, when given with a single oral dose of 60 μg ethinyl estradiol and 300 μg levonorgestrel, increased the AUC of levonorgestrel by 46%. Netupitant and Palonosetron had no significant effect on the AUC of ethinyl estradiol.
- Co-administration of netupitant 450 mg did not significantly affect the systemic exposure and urinary excretion of digoxin, a substrate of P-glycoprotein, at steady-state. Concurrent administration of Netupitant and Palonosetron with digoxin is not expected to affect the systemic exposure to digoxin.
Effects of other drugs on Netupitant and Palonosetron
- Single dose Netupitant and Palonosetron was administered with rifampicin, a strong CYP3A4 inducer, following once daily administration of 400 mg rifampicin for 17 days. Pharmacokinetics of netupitant and palonosetron were compared to that after administration of Netupitant and Palonosetron alone. Co-administration of rifampicin decreased the mean Cmax and AUC0-∞ of netupitant by 62% and 82%, respectively, compared to those after Netupitant and Palonosetron alone. Co-administration of rifampicin decreased the mean Cmax and AUC for palonosetron by 15% and 19%, respectively.
- Single dose Netupitant and Palonosetron was administered with ketoconazole, a strong CYP3A4 inhibitor, following once daily administration of 400 mg ketoconazole for 12 days. Pharmacokinetics of netupitant and palonosetron were compared to that after administration of Netupitant and Palonosetron alone. Co-administration with ketoconazole increased mean Cmax and AUC of netupitant by 25% and 140%, respectively, compared to those after administration of Netupitant and Palonosetron alone. The mean AUC and Cmax of palonosetron were 10% and 15% higher, respectively, when co-administered with ketoconazole.
Nonclinical Toxicology
Carcinogenesis, Mutagenesis, Impairment of Fertility
Netupitant
- Long-term studies in animals to evaluate carcinogenic potential have not been performed with netupitant. Netupitant was not genotoxic in the Ames test, the mouse lymphoma cell mutation test, or the in vivo rat micronucleus test.
- Daily oral administration of netupitant in rats at doses up to 30 mg/kg (1.9 times the human AUC in male rats and 3.7 times the human AUC in female rats at the recommended human dose) had no effects on fertility or reproductive performance.
Palonosetron
- In a 104-week carcinogenicity study in CD-1 mice, animals were treated with oral doses of palonosetron at 10, 30, and 60 mg/kg/day. Treatment with palonosetron was not tumorigenic. The highest tested dose produced a systemic exposure to palonosetron (plasma AUC) of about 90 to 173 times the human exposure (AUC=49.7 ng•h/mL) at the recommended oral dose of 0.5 mg. In a 104-week carcinogenicity study in Sprague-Dawley rats, male and female rats were treated with oral doses of 15, 30, and 60 mg/kg/day and 15, 45, and 90 mg/kg/day, respectively. The highest doses produced a systemic exposure to palonosetron (plasma AUC) of 82 and 185 times the human exposure at the recommended dose. Treatment with palonosetron produced increased incidences of adrenal benign pheochromocytoma and combined benign and malignant pheochromocytoma, increased incidences of pancreatic Islet cell adenoma and combined adenoma and carcinoma and pituitary adenoma in male rats. In female rats, it produced hepatocellular adenoma and carcinoma and increased the incidences of thyroid C-cell adenoma and combined adenoma and carcinoma.
- Palonosetron was not genotoxic in the Ames test, the Chinese hamster ovarian cell (CHO/HGPRT) forward mutation test, the ex vivo hepatocyte unscheduled DNA synthesis (UDS) test, or the mouse micronucleus test. It was, however, positive for clastogenic effects in the Chinese hamster ovarian (CHO) cell chromosomal aberration test. Palonosetron at oral doses up to 60 mg/kg/day (about 921 times the recommended human oral dose based on body surface area) was found to have no effect on fertility and reproductive performance of male and female rats.
Clinical Studies
- Oral administration of Netupitant and Palonosetron in combination with dexamethasone has been shown to prevent acute and delayed nausea and vomiting associated with initial and repeat courses of chemotherapy in two trials.
Study 1
- In a multicenter, randomized, parallel, double-blind, controlled clinical trial of 694 patients, the efficacy and safety of a single dose of oral netupitant in combination with oral palonosetron was compared with a single oral dose of palonosetron in cancer patients receiving a chemotherapy regimen that included cisplatin (median dose=75 mg/m2). The efficacy of Netupitant and Palonosetron was assessed in 135 patients who received Netupitant and Palonosetron (netupitant 300 mg and palonosetron 0.5 mg) and 136 patients who received oral palonosetron 0.5 mg.
- Treatment regimens for the Netupitant and Palonosetron and palonosetron arms are summarized in Table 5.

- Of the 135 patients who received Netupitant and Palonosetron, 43% were women, and all patients were White. The age ranged from 19 to 77 years, with a median age of 53 years.
- During the study, 86% of the 135 treated patients in the Netupitant and Palonosetron arm received a concomitant chemotherapeutic agent in addition to protocol-mandated cisplatin. The most common chemotherapeutic agents and the proportion of patients exposed were cyclophosphamide (34%), fluorouracil (24%), etoposide (21%), and doxorubicin (16%).
- The key efficacy endpoints were complete response (CR) (defined as no emetic episode and no use of rescue medication) for the 25‑120 hour interval (delayed phase), CR for the 0-24 hour interval (acute phase), and CR within 120 hours (overall phase) after the start of the chemotherapy administration.
- A summary of the key results from this study is shown in Table 6.

Study 2
- In a multicenter, randomized, parallel, double-blind, active controlled, superiority trial, the efficacy and safety of a single oral dose of Netupitant and Palonosetron was compared with a single oral dose of palonosetron 0.5 mg in cancer patients scheduled to receive the first cycle of an anthracycline and cyclophosphamide (AC) regimen for the treatment of a solid malignant tumor (Study 2). All patients received a single oral dose of dexamethasone.
- Treatment regimens for the Netupitant and Palonosetron and palonosetron arms are summarized in Table 7.

- After completion of cycle 1, patients had the option to participate in a multiple-cycle extension, receiving the same treatment as assigned in cycle 1. There was no pre-specified limit of the number of repeat consecutive cycles for any patient.
- A total of 1455 patients were randomized to the Netupitant and Palonosetron arm or palonosetron arm. A total of 1450 patients (Netupitant and Palonosetron n=725; palonosetron n=725) received study medication: of these, 1438 patients (98.8%) completed cycle 1 and 1286 patients (88.4%) continued treatment in the multiple‑cycle extension. A total of 907 patients (62.3%) completed the multiple‑cycle extension up to a maximum of eight treatment cycles.
- Of the 725 patients who received Netupitant and Palonosetron, 711 (98%) were women; 79% were White, 14% Asian, 6% Hispanic, and <1% were Black or Other. Age ranged from 22 to 79 years, with a median age of 54 years. A total of 724 patients (99.9%) were treated with cyclophosphamide. All patients were additionally treated with either doxorubicin (68.0%) or epirubicin (32.0%).
- During the first cycle, 32% of the 725 patients treated with Netupitant and Palonosetron received a concomitant chemotherapeutic agent in addition to protocol-mandated regimens, with the most common chemotherapeutic being fluorouracil (28.3%) and docetaxel (2.6%).
- The primary efficacy endpoint was the CR rate in the delayed phase, 25-120 hours after the start of chemotherapy administration.
- Major secondary efficacy endpoints included CR for the acute and overall phases.
- A summary of key results from Study 2 is shown in Table 8.
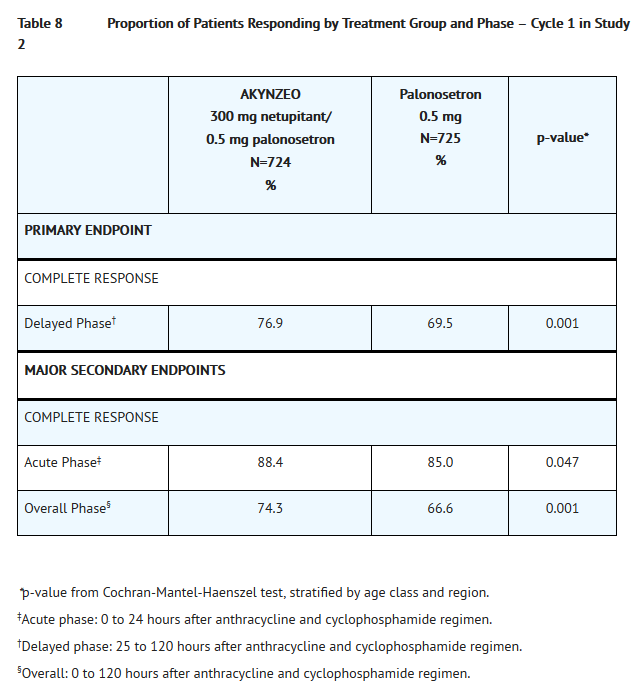
This image is provided by the National Library of Medicine.

Multiple cycles
- Patients continued into the Multiple-Cycle extension for up to 7 additional cycles of chemotherapy. The proportion of patients with complete response in the delayed phase by treatment group at each cycle (cycles 2 to 6) is displayed in Figure 1. A limited number of patients received treatment beyond cycle 6. During all cycles the CR rate in the delayed phase was higher for Netupitant and Palonosetron than for palonosetron. Antiemetic activity of Netupitant and Palonosetron was maintained throughout repeat cycles for those patients continuing in each of the multiple cycles

- Additional clinical trials (Study 3 and Study 4) were conducted to support the efficacy of Netupitant and Palonosetron.
Study 3
- In a separate study, 309 patients undergoing initial and repeat cycles of chemotherapy (including carboplatin, cisplatin, oxaliplatin, and doxorubicin regimens) received Netupitant and Palonosetron; efficacy was maintained throughout all cycles.
Study 4
- In one multicenter, multinational, randomized, active-controlled, double-blind, double-dummy, parallel group, clinical non-inferiority study, the efficacy and safety of a single dose of oral palonosetron 0.50 mg was compared to intravenous palonosetron 0.25 mg in cancer patients scheduled to receive highly emetogenic cisplatin (>70 mg/m2) based chemotherapy. The purpose of this study was to demonstrate that oral palonosetron 0.5 mg contributes to the efficacy of Netupitant and Palonosetron during the acute phase (first 24 hours after cancer chemotherapy) in the setting of cisplatin based chemotherapy. A total of 739 patients (oral palonosetron n=370; intravenous palonosetron n=369) received study medication.
- The primary efficacy endpoint was complete response (CR) (defined as no emetic episode and no use of rescue medication) within 24 hours (acute phase) after the start of cisplatin-based chemotherapy administration. In the oral palonosetron arm, 89.4% of patients achieved a CR in the acute phase compared to 86.2% of patients in the intravenous palonosetron arm, with a difference of 3.21% (99%
CI: -2.74% to 9.17%). Non-inferiority of oral palonosetron versus intravenous palonosetron was demonstrated since the lower limit of the two‑sided 99% CI for the difference in proportions of patients with CR was greater (i.e., closer to zero) than the pre-defined non-inferiority margin set at -15%.
How Supplied
- NDC # 62856-796-01, Netupitant and Palonosetron (300 mg netupitant/0.5 mg palonosetron). Netupitant and Palonosetron is supplied as hard gelatin capsules with white body and caramel cap with “HE1” printed on the body, one capsule per blister.
Storage
- Store at 20 °C to 25 °C (68 °F to 77 °F); excursions permitted from 15 °C to 30 °C (59 °F to 86 °F) [see USP Controlled Room Temperature].
Images
Drug Images
{{#ask: Page Name::Netupitant and palonosetron |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Netupitant and palonosetron |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
- Advise patients to read the FDA-approved patient labeling (Patient Information).
Administration
- Advise patients to take Netupitant and Palonosetron with or without food approximately 1 hour prior to the start of chemotherapy.
Hypersensitivity Reactions
- Advise patients that hypersensitivity reactions, including anaphylaxis, have been reported in patients receiving palonosetron. Advise patients to seek immediate medical attention if any signs or symptoms of a hypersensitivity reaction occur while taking Netupitant and Palonosetron.
Serotonin Syndrome
- Advise patients of the possibility of serotonin syndrome especially with concomitant use of Netupitant and Palonosetron and another serotonergic agent such as medications to treat depression and migraines. Advise patients to seek immediate medical attention if the following symptoms occur: changes in mental status, autonomic instability, neuromuscular symptoms, with or without gastrointestinal symptoms
Precautions with Alcohol
- Alcohol-Netupitant and Palonosetron interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- Akynzeo®[1]
Look-Alike Drug Names
- A® — B®[2]
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
- ↑ Empty citation (help)
- ↑ "http://www.ismp.org". External link in
|title=(help)
{{#subobject:
|Page Name=Netupitant and palonosetron
|Pill Name=No image.jpg
|Drug Name=
|Pill Ingred=|+sep=;
|Pill Imprint=
|Pill Dosage={{{dosageValue}}} {{{dosageUnit}}}
|Pill Color=|+sep=;
|Pill Shape=
|Pill Size (mm)=
|Pill Scoring=
|Pill Image=
|Drug Author=
|NDC=
}}
{{#subobject:
|Label Page=Netupitant and palonosetron |Label Name=Netupitant and palonosetron10.png
}}
{{#subobject:
|Label Page=Netupitant and palonosetron |Label Name=Netupitant and palonosetron11.png
}}
{{#subobject:
|Label Page=Netupitant and palonosetron |Label Name=Netupitant and palonosetron12.png
}}