Bowel obstruction
Template:DiseaseDisorder infobox
|
WikiDoc Resources for Bowel obstruction |
|
Articles |
|---|
|
Most recent articles on Bowel obstruction Most cited articles on Bowel obstruction |
|
Media |
|
Powerpoint slides on Bowel obstruction |
|
Evidence Based Medicine |
|
Cochrane Collaboration on Bowel obstruction |
|
Clinical Trials |
|
Ongoing Trials on Bowel obstruction at Clinical Trials.gov Trial results on Bowel obstruction Clinical Trials on Bowel obstruction at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Bowel obstruction NICE Guidance on Bowel obstruction
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Bowel obstruction Discussion groups on Bowel obstruction Patient Handouts on Bowel obstruction Directions to Hospitals Treating Bowel obstruction Risk calculators and risk factors for Bowel obstruction
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Bowel obstruction |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [2] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Bowel obstruction is a mechanical or functional obstruction of the intestines, preventing the normal transit of the products of digestion. It can occur at any level distal to the duodenum of the small intestine and is a medical emergency. Although many cases are not treated surgically, it is a surgical problem.
Causes
Small bowel obstruction
Differential diagnosis by location
Causes of small bowel obstruction include:
- Adhesions from previous abdominal surgery
- Carcinoid rare, preferred location: ileum
- Crohn's disease causing adhesions or inflammatory strictures
- Foreign bodies (e.g. gallstones in gallstone ileus, swallowed objects)
- Hernias containing bowel
- Intestinal atresia
- Intussusception in children
- Ischaemic strictures
- Neoplasms, benign or malignant
- Volvulus
-
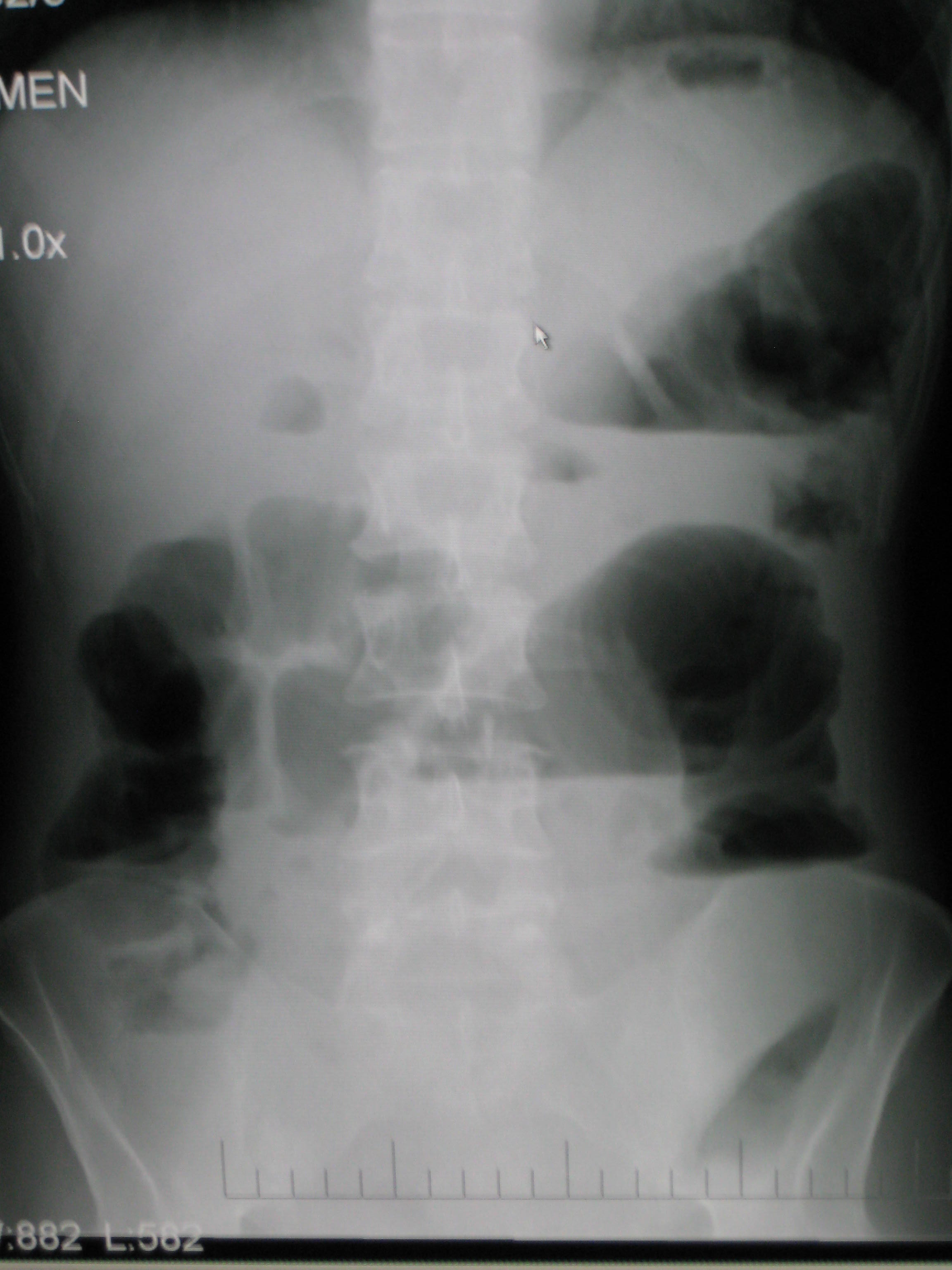
Upright abdominal X-ray demonstrating a small bowel obstruction. Note multiple air fluid levels.

Large bowel obstruction
Causes of large bowel obstruction include:
- Neoplasms
- Hernias
- Inflammatory bowel disease
- Colonic volvulus (sigmoid, caecal, transverse colon)
- Faecal impaction
- Colon atresia
- Benign strictures (Diverticular Disease)
-
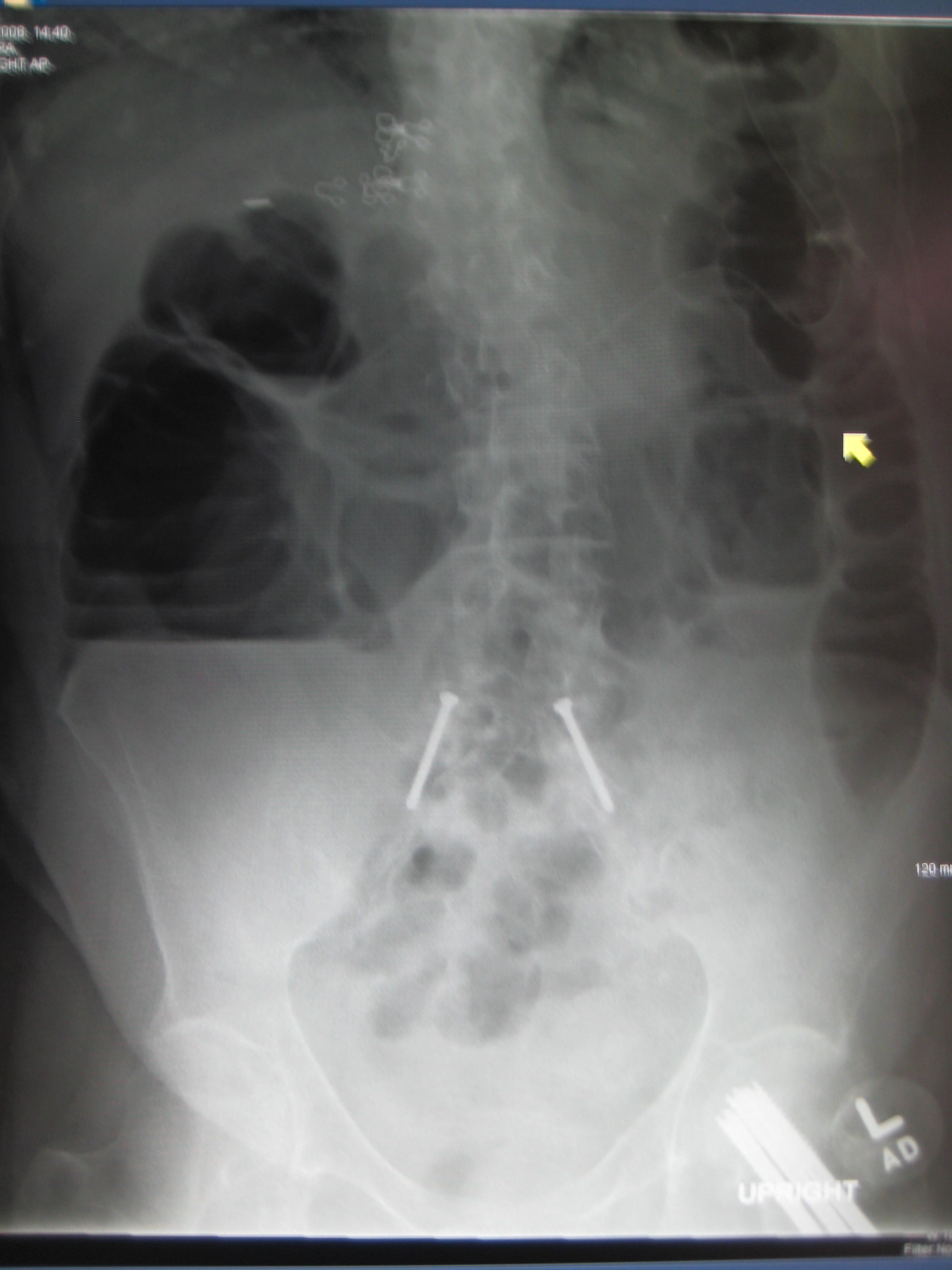
Upright abdominal X-ray of a patient with a large bowel obstruction showing multiple air fluid levels and dilated loops of bowel.

Differential diagnosis of causes of bowel obstruction by organ system
Trauma, mechanical and physical conditions
- Intestinal stricture
- Intususception of intestine
Miscellaneous syndromes
- Pseudo-obstruction or Ogilvie's syndrome
- Paralytic Ileus
Chromosomal abnormalities
- Down syndrome
Autosomal dominant conditions
- Neurofibromatosis type 1
Malignant neoplastic conditions
- Carcinoid tumours and carcinoid syndrome
- Colorectal cancer
- Ovarian cancer
- Pseudomyxoma peritonei
- Small bowel lymphoma
- Stomach cancer
Trauma, mechanical and physical conditions
- Bowel strangulation
- Femoral hernia
- Ileus
- Inguinal hernia
- Intestinal volvulus
- Large bowel obstruction
- Obturator hernia
- Peritoneal adhesions
- Small bowel obstruction
Infectious disorders
Signs, symptoms and causes
Depending on the level of obstruction, bowel obstruction can present with abdominal pain, abdominal distension, vomiting, fecal vomiting, and constipation.
Obstruction may be due to causes within the bowel lumen, within the wall of the bowel, or external to the bowel (such as compression, entrapment or volvulus).
Bowel obstruction may be complicated by dehydration and electrolyte abnormalities due to vomiting; respiratory compromise from pressure on the diaphragm by a distended abdomen, or aspiration of vomitus; bowel ischaemia or perforation from prolonged distension or pressure from a foreign body.
In small bowel obstruction the pain tends to be colicky (cramping and intermittent) in nature, with spasms lasting a few minutes. The pain tends to be central and mid-abdominal. Vomiting occurs before constipation.
In large bowel obstruction the pain is felt lower in the abdomen and the spasms last longer. Constipation occurs earlier and vomiting may be less prominent. Proximal obstruction of the large bowel may present as small bowel obstruction.
Diagnosis
The main diagnostic tools are blood tests, X-rays of the abdomen, CT scanning and/or ultrasound. If a mass is identified, biopsy may determine the nature of the mass.
Radiological signs of bowel obstruction include bowel distension and the presence of multiple (more than six) gas-fluid levels on supine and erect abdominal radiographs.
Contrast enema or small bowel series or CT scan can be used to define the level of obstruction, whether the obstruction is partial or complete, and to help define the cause of the obstruction.
According to a meta-analysis of prospective studies by the Cochrane Collaboration, the appearance of water-soluble contrast in the cecum on an abdominal radiograph within 24 hours of oral administration predicts resolution of an adhesive small bowel obstruction with a pooled sensitivity of 96% and specificity of 96%. PMID 15674958
Colonoscopy, small bowel investigation with ingested camera or push endoscopy, and laparoscopy are other diagnostic options.
Treatment
Some causes of bowel obstruction may resolve spontaneously; many require operative treatment.
In adults, frequently the surgical intervention and the treatment of the causative lesion are required. In malignant large bowel obstruction, endoscopically placed self-expanding metal stents may be used to temporarily relieve the obstruction as a bridge to surgery, or as palliation.
Small bowel obstruction
In the management of small bowel obstructions it is often said that "[n]ever let the sun rise or set on small-bowel obstruction"[1] because they are sometimes fatal if treatment is delayed.
Treatment for a small bowel obstruction is both non-surgical (conservative) and surgical.
Conservative treatment involves insertion of a nasogastric tube, correction of dehydration and electrolyte abnormalities. Opioid pain relievers may be used for patients with severe pain. Antiemetics may be administered if the patient is vomiting. Adhesive obstructions often settle without surgery. If obstruction is complete a surgery is required.
Small bowel obstruction caused by Crohn's disease, peritoneal carcinomatosis, sclerosing peritonitis, radiation enteritis and postpartum bowel obstruction are typically treated conservatively, i.e. without surgery. Conversely, a small bowel obstruction in a "virgin abdomen" (an abdomen that has not seen an operation) is almost never treated conservatively.
Bowel obstruction in children
Fetal and neonatal bowel obstructions are often caused by an intestinal atresia where there is a narrowing or absence of a part of the intestine. These atresias are often discovered before birth via a sonogram and treated with using laparotomy after birth. If the area affected is small then the surgeon may be able to remove the damaged portion and join the intestine back together. In instantances where the narrowing is longer, or the area is damaged and cannot be used for a period of time, a temporary stoma may be placed.
Pathological Findings
-

Intestine: Ileus Newborn Cause Unknown: Gross natural color opened body with protruding grossly dilated loops of bowel there was no evidence of necrotizing enteritis
-

Intestine: Ileus Newborn Cause Unknown: Gross natural color close-up view of distended gut loops


References
See also
External links
- Obstruction, Small Bowel at eMedicine
- Obstruction, Large Bowel at eMedicine
- UCSF Fetal Treatment Center: Bowel Obstructions
- Intestinal Obstruction in Adults
- A Lecture on Bowel Obstruction
Template:SIB Template:Gastroenterology