Aortic dissection MRI: Difference between revisions
(/* Surveillance of Thoracic Aortic Disease or Previously Repaired Patients (DO NOT EDIT){{cite journal |author=Hiratzka LF, Bakris GL, Beckman JA, et al. |title=2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and manag...) |
(/* 2010 ACC/ AHA Guideline Recommendations: Evaluation and Management of Acute Thoracic Aortic Disease (DO NOT EDIT){{cite journal |author=Hiratzka LF, Bakris GL, Beckman JA, et al. |title=2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines...) |
||
| Line 19: | Line 19: | ||
</div> | </div> | ||
==2010 | ==2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guideline Recommendations: Evaluation and Management of Acute Thoracic Aortic Disease (DO NOT EDIT)<ref name="pmid20233780">{{cite journal |author=Hiratzka LF, Bakris GL, Beckman JA, ''et al.'' |title=2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine |journal=[[Circulation]] |volume=121 |issue=13 |pages=e266–369 |year=2010 |month=April |pmid=20233780 |doi=10.1161/CIR.0b013e3181d4739e |url=}}</ref>== | ||
===Screening Tests for Aortic Dissection (DO NOT EDIT)<ref name="pmid20233780">{{cite journal |author=Hiratzka LF, Bakris GL, Beckman JA, ''et al.'' |title=2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine |journal=[[Circulation]] |volume=121 |issue=13 |pages=e266–369 |year=2010 |month=April |pmid=20233780 |doi=10.1161/CIR.0b013e3181d4739e |url=}}</ref>=== | ===Screening Tests for Aortic Dissection (DO NOT EDIT)<ref name="pmid20233780">{{cite journal |author=Hiratzka LF, Bakris GL, Beckman JA, ''et al.'' |title=2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine |journal=[[Circulation]] |volume=121 |issue=13 |pages=e266–369 |year=2010 |month=April |pmid=20233780 |doi=10.1161/CIR.0b013e3181d4739e |url=}}</ref>=== | ||
Revision as of 00:04, 2 November 2012
|
Aortic dissection Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Special Scenarios |
|
Case Studies |
|
|
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] ; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
MRI is the imaging modality of choice in the assessment of longstanding aortic disease in a patient who has chronic chest pain who is hemodynamically stable or for the evaluation of a chronic dissection.
MRI
- Magnetic resonance imaging (MRI) is currently the gold standard test for the detection and assessment of aortic dissection, with a sensitivity of 98% and a specificity of 98%.
- An MRI examination of the aorta will produce a three-dimensional reconstruction of the aorta, allowing the physician to determine the location of the intimal tear, the involvement of branch vessels, and locate any secondary tears.
- It is a non-invasive test, does not require the use of iodinated contrast material, and can detect and quantitate the degree of aortic insufficiency.
- The disadvantage of the MRI scan in the face of aortic dissection is that it has limited availability and is often located only in larger hospitals, and the scan is relatively time consuming.
- Due to the high intensity of the magnetic waves used during MRI, an MRI scan is contraindicated in individuals with metallic implants. *In addition, many individuals develop claustrophobia while in the MRI scanning tube.
-
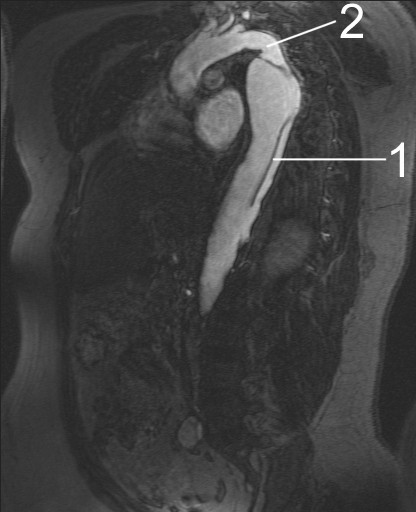
MRI of an aortic dissection. 1 Aorta descendens with dissection. 2 Aortic isthmus.

2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guideline Recommendations: Evaluation and Management of Acute Thoracic Aortic Disease (DO NOT EDIT)[1]
Screening Tests for Aortic Dissection (DO NOT EDIT)[1]
| Class I |
| "1. Urgent and definitive imaging of the aorta using transesophageal echocardiogram, computed tomographic imaging, or magnetic resonance imaging is recommended to identify or exclude thoracic aortic dissection in patients at high risk for the disease by initial screening (Level of Evidence: B)" |
Determining the Presence and Measuring the Progression of Thoracic Aortic Disease (DO NOT EDIT)[1]
| Class I |
| "1. For measurements taken by computed tomographic imaging or magnetic resonance imaging, the external diameter should be measured perpendicular to the axis of blood flow. For aortic root measurements, the widest diameter, typically at the mid-sinus level, should be used. (Level of Evidence: C)" |
Aortic Imaging in Genetic Syndromes (DO NOT EDIT) [1]
| Class I |
| "1. Patients with Loeys-Dietz syndrome should have yearly magnetic resonance imaging from the cerebrovascular circulation to the pelvis. (Level of Evidence: B)" |
Takayasu Arteritis and Giant Cell Arteritis (DO NOT EDIT) [1]
| Class I |
| "1. The initial evaluation of Takayasu arteritis or giant cell arteritis should include thoracic aorta and branch vessel computed tomographic imaging or magnetic resonance imaging to investigate the possibility of aneurysm or occlusive disease in these vessels. (Level of Evidence: C)" |
Surveillance of Thoracic Aortic Disease or Previously Repaired Patients (DO NOT EDIT)[1]
| Class IIa |
| "1. Computed tomographic imaging or magnetic resonance imaging of the thoracic aorta is reasonable after a Type A or B aortic dissection or after prophylactic repair of the aortic root/ascending aorta. (Level of Evidence:C)" |
| "2. Computed tomographic imaging or magnetic resonance imaging of the aorta is reasonable at 1, 3, 6, and 12 months postdissection and, if stable, annually thereafter so that any threatening enlargement can be detected in a timely fashion. (Level of Evidence:C)" |
| "3. When following patients with imaging, utilization of the same modality at the same institution is reasonable, so that similar images of matching anatomic segments can be compared side by side. (Level of Evidence:C)" |
| "4. Surveillance imaging similar to classic aortic dissection is reasonable in patients with intramural hematoma. (Level of Evidence:C)" |
2010 ACC/AHA Guidelines - ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance (DO NOT EDIT)[2]
| “ |
Cardiovascular Magnetic Resonance of thoracic aortic disease, CMR may be used for defining the location and extent of aortic aneurysms, erosions, ulcers, dissections; evaluating postsurgical processes involving the aorta and surrounding structures, and aortic size blood flow and cardiac cycle–dependent changes in area. |
” |
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 Hiratzka LF, Bakris GL, Beckman JA; et al. (2010). "2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine". Circulation. 121 (13): e266–369. doi:10.1161/CIR.0b013e3181d4739e. PMID 20233780. Unknown parameter
|month=ignored (help) - ↑ American College of Cardiology Foundation Task Force on Expert Consensus Documents. Hundley WG, Bluemke DA, Finn JP, Flamm SD, Fogel MA; et al. (2010). "ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents". Circulation. 121 (22): 2462–508. doi:10.1161/CIR.0b013e3181d44a8f. PMC 3034132. PMID 20479157.