Hypertrophic cardiomyopathy histopathology
|
Hypertrophic Cardiomyopathy Microchapters |
|
Differentiating Hypertrophic Cardiomyopathy from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Hypertrophic cardiomyopathy histopathology On the Web |
|
Directions to Hospitals Treating Hypertrophic cardiomyopathy |
|
Risk calculators and risk factors for Hypertrophic cardiomyopathy histopathology |
Editors-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
On histopathologic examination, hypertrophic cardiomyopathy is characterized by both myocardial disarray and by periarteriolar fibrosis. Myocardial disarray can be associated with aberrant impulse conduction and arrhythmias, and periarteriolar fibrosis can be associated with myocardial ischemia.
Histopathologic Abnormalities
Myocardial Disarray
In HCM, the normal alignment of muscle cells is disrupted (there is a swirling pattern to the arrangement of the muscle cells), a phenomenon known as myocardial disarray. HCM is believed to be due to a mutation in one of many genes that results in a mutated myosin heavy chain, one of the components of the myocyte (the muscle cell of the heart). Histopathologically, the cardiac sarcomere is abnormal resulting in hypertrophy of the left ventricle in the absence of other disorders that could produce the condition such as hypertension, amyloid or aortic stenosis. The presence of myocardial disarray may be associated with abnormalities of electrical conduction in the heart (including electrical reentry loops) which thereby contributes to an increased risk of sudden cardiac death.
-
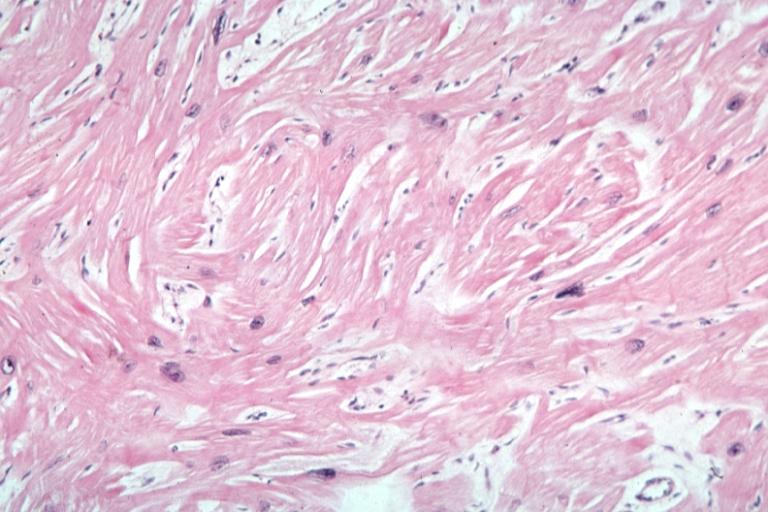 Myocardial disarray with swirling pattern of myocytes
Myocardial disarray with swirling pattern of myocytes -
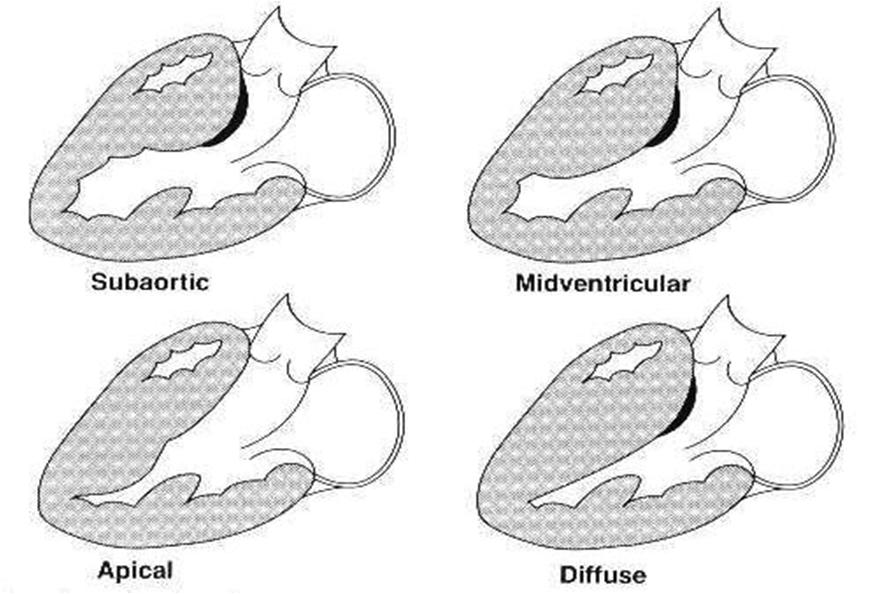 Variants of hypertrophic cardiomyopathy
Variants of hypertrophic cardiomyopathy -
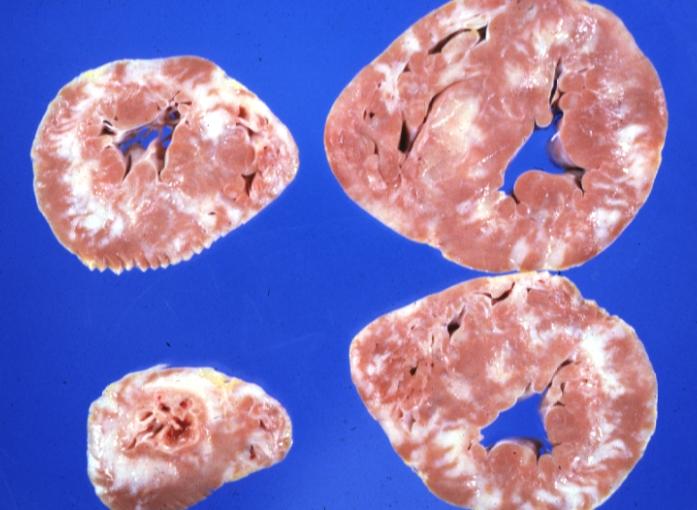 White areas of fibrosis or scar in a patient with HCM which may contribute in part to arrhythmias
White areas of fibrosis or scar in a patient with HCM which may contribute in part to arrhythmias



Periarteriolar Fibrosis
Compared to normal arterioles on the left, the arterioles from a patient with hyertension (middle) show moderate periarteriolar thickening and fibrosis. Shown on the right is a patient with HCM in which there is even more signficant periarteriolar thickening and fibrosis. This thickening of the wall of the intramyocardial arterioles leads to an increased wall/lumen ratio, subendocardial ischemia and impaired coronary flow reserve[1][2]. Patients who subsequently died in one series had abnormal coronary flow reserve on PET scanning at baseline indicating that ischemia may play a role, at least in part, in subsequent mortality.
-
 Normal arteriole
Normal arteriole -
 Hypertensive arteriole with wall thickening and myocyte hypertrophy
Hypertensive arteriole with wall thickening and myocyte hypertrophy -
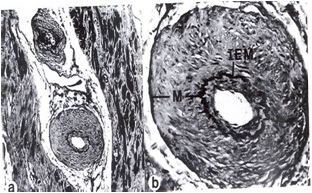 Arteriole in HCM patient with periarteriole fibrosis and thicknening
Arteriole in HCM patient with periarteriole fibrosis and thicknening



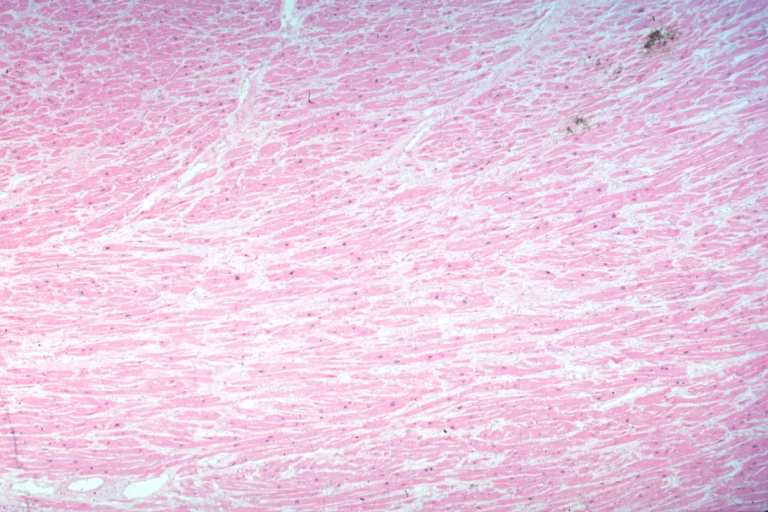
Microscopic Pathological Findings
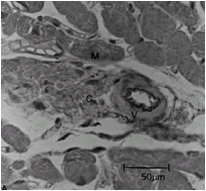
Histopathologically, small vessels have hypertrophy of the tunica media. Combined with increased wall tension, decreased vasodilator reserve and inadequate capillary density, there is a mismatch between blood supply and demand. Over time, it is thought that there is repeated ischemia followed by fibrosis and eventually, dilation and systolic dysfunction (“burned out hypertrophy”).
-
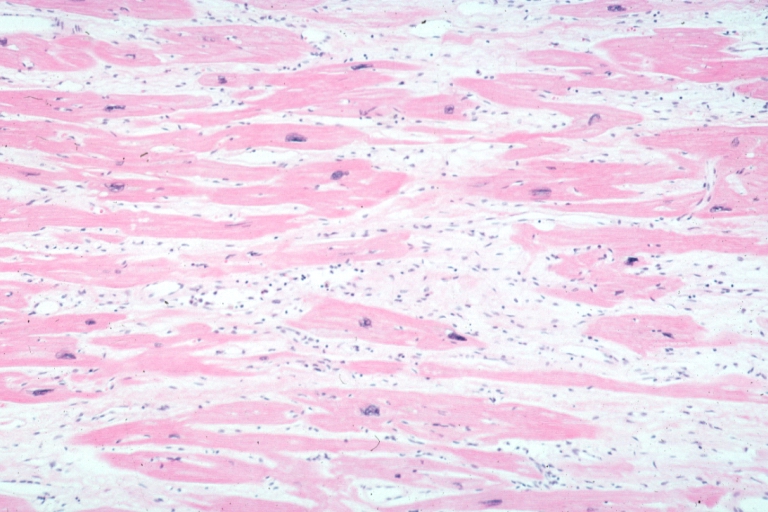
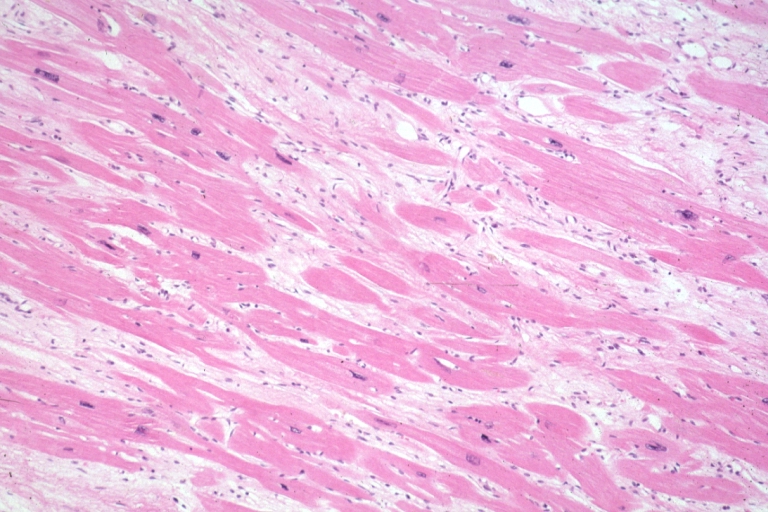 Micro med mag H&E mid-mural myocardium with hypertrophy and interstitial fibrosis atrophy is present marked increase in interstitial fibroblastic cells
Micro med mag H&E mid-mural myocardium with hypertrophy and interstitial fibrosis atrophy is present marked increase in interstitial fibroblastic cells -
 Micro high mag H&E myofiber hypertrophy and interstitial fibrosis with marked increase in interstitial fibroblastic cells
Micro high mag H&E myofiber hypertrophy and interstitial fibrosis with marked increase in interstitial fibroblastic cells


-
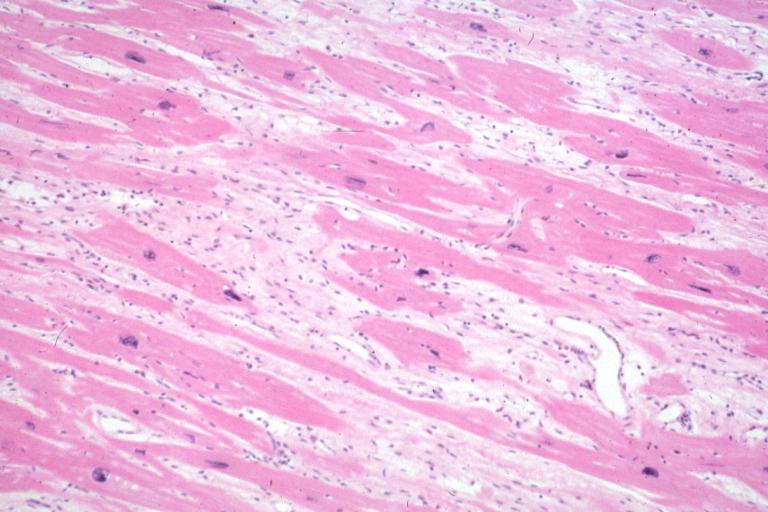
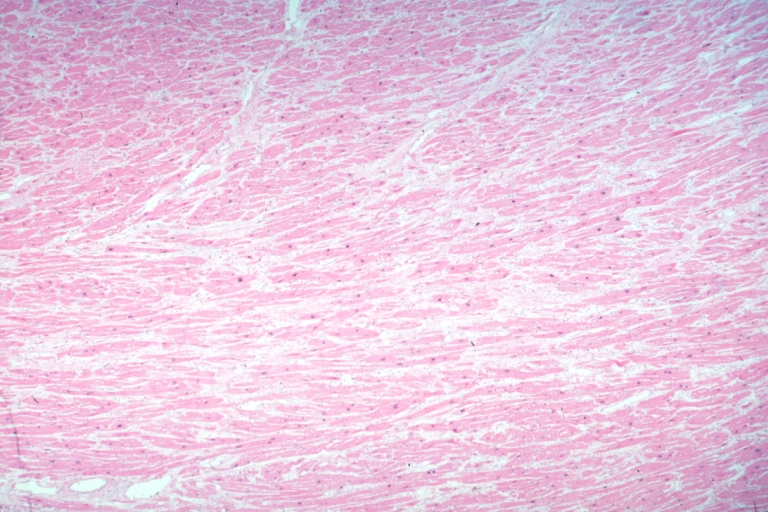
 Micro med mag H&E myofiber hypertrophy some atrophy interstitial fibrosis with many fibroblastic cells
Micro med mag H&E myofiber hypertrophy some atrophy interstitial fibrosis with many fibroblastic cells -
 Micro high mag H&E hypertrophied fibers with some evidence of atrophy and marked interstitial fibrosis with many fibroblastic type cells
Micro high mag H&E hypertrophied fibers with some evidence of atrophy and marked interstitial fibrosis with many fibroblastic type cells


-
 Micro low mag H&E shows myofiber hypertrophy and interstitial fibrosis
Micro low mag H&E shows myofiber hypertrophy and interstitial fibrosis -
 Cardiomyopathy: Micro H&E low mag interventricular septum at junction of normal myofiber orientation with asymmetrical hypertrophy (an excellent example)
Cardiomyopathy: Micro H&E low mag interventricular septum at junction of normal myofiber orientation with asymmetrical hypertrophy (an excellent example)


-
 Cardiomyopathy: Micro H&E low mag marked myofiber disarray asymmetrical hypertrophy
Cardiomyopathy: Micro H&E low mag marked myofiber disarray asymmetrical hypertrophy -
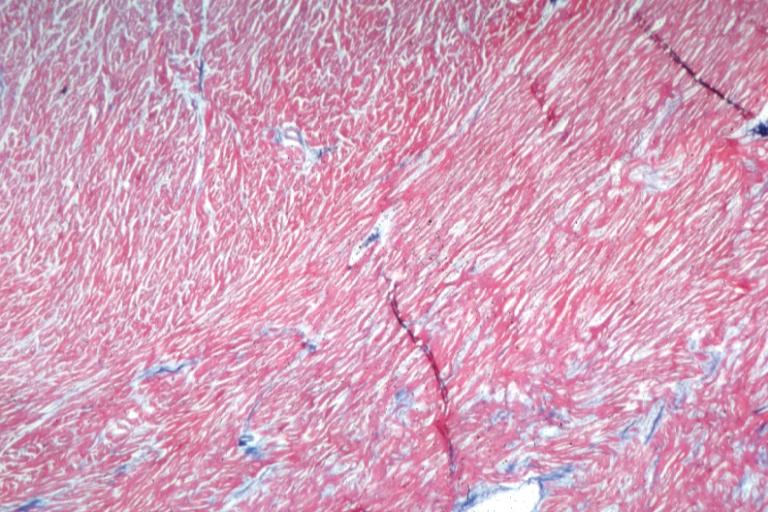
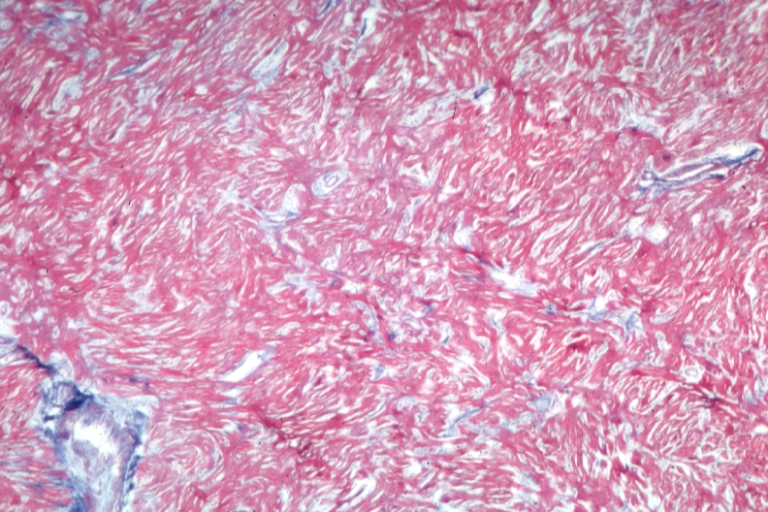
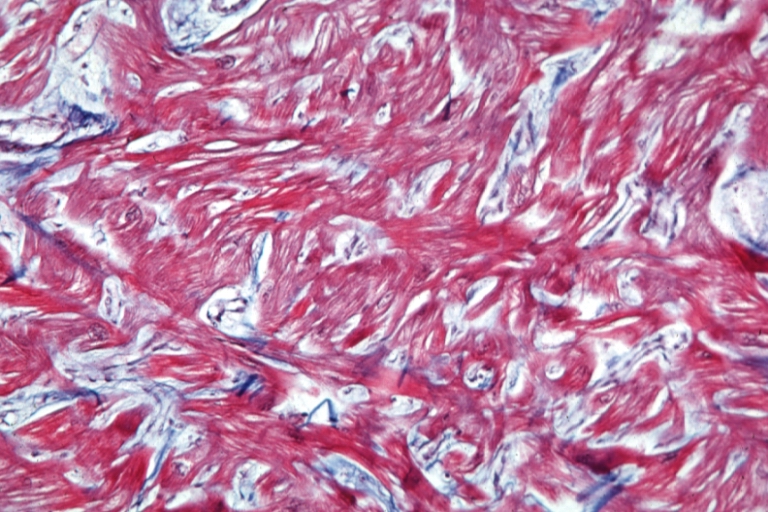 Cardiomyopathy: Micro trichrome high mag marked myofiber disarray
Cardiomyopathy: Micro trichrome high mag marked myofiber disarray


-
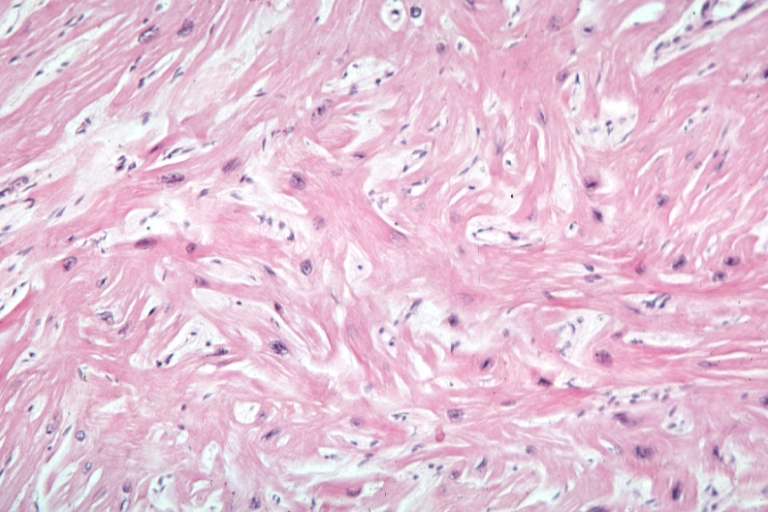 Cardiomyopathy: Micro H&E med mag excellent example myofiber disarray
Cardiomyopathy: Micro H&E med mag excellent example myofiber disarray -
Cardiomyopathy: Micro H&E high mag excellent example myofiber disarray

References
- ↑ Lorenzoni R, Gistri R, Cecchi F, Olivotto I, Chiriatti G, Elliott P; et al. (1998). "Coronary vasodilator reserve is impaired in patients with hypertrophic cardiomyopathy and left ventricular dysfunction". Am Heart J. 136 (6): 972–81. PMID 9842009.
- ↑ Choudhury L, Elliott P, Rimoldi O, Ryan M, Lammertsma AA, Boyd H; et al. (1999). "Transmural myocardial blood flow distribution in hypertrophic cardiomyopathy and effect of treatment". Basic Res Cardiol. 94 (1): 49–59. PMID 10097830.