Pegylated interferon alfa-2b
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Vignesh Ponnusamy, M.B.B.S. [2]
Disclaimer
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Black Box Warning
|
Title
See full prescribing information for complete Boxed Warning.
ConditionName:
|
Overview
Pegylated interferon alfa-2b is a antiviral that is FDA approved for the {{{indicationType}}} of chronic hepatitis c (CHC) in patients with compensated liver disease. There is a Black Box Warning for this drug as shown here. Common adverse reactions include injection site inflammation/reaction, fatigue/asthenia, headache, rigors, fevers, nausea, myalgia and anxiety/emotional lability/irritability.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
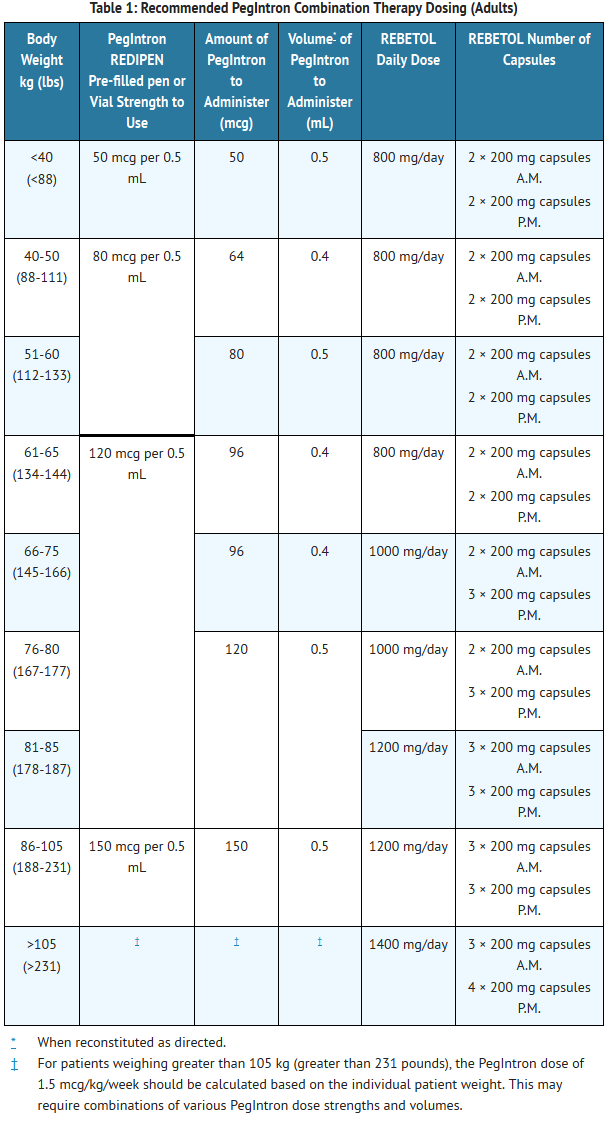
Chronic Hepatitis C (CHC)
- The recommended dose of PegIntron is 1.5 mcg/kg/week. The volume of PegIntron to be injected depends on the strength of PegIntron and patient's body weight (see Table 1).
- The recommended dose of REBETOL for use with PegIntron is 800 to 1400 mg orally based on patient body weight. REBETOL should be taken with food. REBETOL should not be used in patients with creatinine clearance less than 50 mL/min.
- See labeling of the specific HCV NS3/4A protease inhibitor for information regarding dosing regimen and administration of the protease inhibitor in combination with PegIntron and ribavirin.
- Duration of Treatment – Treatment with PegIntron/REBETOL of Interferon Alpha-naïve Patients
- The treatment duration for patients with genotype 1 is 48 weeks. Discontinuation of therapy should be considered in patients who do not achieve at least a 2 log10 drop or loss of HCV-RNA at 12 weeks, or if HCV-RNA remains detectable after 24 weeks of therapy. Patients with genotype 2 and 3 should be treated for 24 weeks.
- Duration of Treatment – Re-treatment with PegIntron/REBETOL of Prior Treatment Failures
- For patients with genotype 1 infection, PegIntron and REBETOL without an HCV NS3/4A protease inhibitor should only be used if there are contraindications, significant intolerance or other clinical factors that would not warrant use of an HCV NS3/4A protease inhibitor. The treatment duration for patients who previously failed therapy is 48 weeks, regardless of HCV genotype. Re-treated patients who fail to achieve undetectable HCV-RNA at Week 12 of therapy, or whose HCV-RNA remains detectable after 24 weeks of therapy, are highly unlikely to achieve SVR and discontinuation of therapy should be considered.
T1
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
Condition1
- Developed by:
- Class of Recommendation:
- Strength of Evidence:
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Guideline-Supported Use of Pegylated interferon alfa-2b in adult patients.
Non–Guideline-Supported Use
Condition1
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Non–Guideline-Supported Use of Pegylated interferon alfa-2b in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
Chronic Hepatitis C (CHC)
- Dosing for pediatric patients is determined by body surface area for PegIntron and by body weight for REBETOL. The recommended dose of PegIntron is 60 mcg/m2/week subcutaneously in combination with 15 mg/kg/day of REBETOL orally in 2 divided doses (see Table 2) for pediatric patients ages 3 to 17 years. Patients who reach their 18th birthday while receiving PegIntron/REBETOL should remain on the pediatric dosing regimen. The treatment duration for patients with genotype 1 is 48 weeks. Patients with genotype 2 and 3 should be treated for 24 weeks.
T2
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
Condition1
- Developed by:
- Class of Recommendation:
- Strength of Evidence:
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Guideline-Supported Use of Pegylated interferon alfa-2b in pediatric patients.
Non–Guideline-Supported Use
Condition1
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Non–Guideline-Supported Use of Pegylated interferon alfa-2b in pediatric patients.
Contraindications
- PegIntron is contraindicated in patients with:
- known hypersensitivity reactions, such as urticaria, angioedema, bronchoconstriction, anaphylaxis, Stevens-Johnson syndrome, and toxic epidermal necrolysis to interferon alpha or any other component of the product
- autoimmune hepatitis
- hepatic decompensation (Child-Pugh score greater than 6 [class B and C]) in cirrhotic CHC patients before or during treatment
- PegIntron/ribavirin combination therapy is additionally contraindicated in:
- women who are pregnant. Ribavirin may cause fetal harm when administered to a pregnant woman. Ribavirin is contraindicated in women who are or may become pregnant. If ribavirin is used during pregnancy, or if the patient becomes pregnant while taking ribavirin, the patient should be apprised of the potential hazard to her fetus.
- men whose female partners are pregnant
- patients with hemoglobinopathies (e.g., thalassemia major, sickle-cell anemia)
- patients with creatinine clearance less than 50 mL/min
Warnings
|
Title
See full prescribing information for complete Boxed Warning.
ConditionName:
|
Precautions
- Use with Ribavirin
- Pregnancy
- Ribavirin may cause birth defects and death of the unborn child. Ribavirin therapy should not be started until a report of a negative pregnancy test has been obtained immediately prior to planned initiation of therapy. Patients should use at least 2 forms of contraception and have monthly pregnancy tests during treatment and during the 6-month period after treatment has been stopped [see Contraindications (4) and ribavirin labeling].
- Anemia
- Ribavirin caused hemolytic anemia in 10% of PegIntron/REBETOL-treated subjects within 1 to 4 weeks of initiation of therapy. Complete blood counts should be obtained pretreatment and at Week 2 and Week 4 of therapy or more frequently if clinically indicated. Anemia associated with ribavirin therapy may result in a worsening of cardiac disease. Decrease in dosage or discontinuation of ribavirin may be necessary [see Dosage and Administration (2.3) and ribavirin labeling].
- Neuropsychiatric Events
- Life-threatening or fatal neuropsychiatric events, including suicide, suicidal and homicidal ideation, depression, relapse of drug addiction/overdose, and aggressive behavior sometimes directed towards others have occurred in patients with and without a previous psychiatric disorder during PegIntron treatment and follow-up. Psychoses, hallucinations, bipolar disorders, and mania have been observed in patients treated with interferon alpha.
- PegIntron should be used with caution in patients with a history of psychiatric disorders. Treatment with interferons may be associated with exacerbated symptoms of psychiatric disorders in patients with co-occurring psychiatric and substance use disorders. If treatment with interferons is initiated in patients with prior history or existence of psychiatric condition or with a history of substance use disorders, treatment considerations should include the need for drug screening and periodic health evaluation, including psychiatric symptom monitoring. Early intervention for re-emergence or development of neuropsychiatric symptoms and substance use is recommended.
- Patients should be advised to report immediately any symptoms of depression or suicidal ideation to their prescribing physicians. Physicians should monitor all patients for evidence of depression and other psychiatric symptoms. If patients develop psychiatric problems, including clinical depression, it is recommended that the patients be carefully monitored during treatment and in the 6-month follow-up period. If psychiatric symptoms persist or worsen, or suicidal ideation or aggressive behavior towards others is identified, it is recommended that treatment with PegIntron be discontinued, and the patient followed, with psychiatric intervention as appropriate. In severe cases, PegIntron should be stopped immediately and psychiatric intervention instituted [see Dosage and Administration (2.3)]. Cases of encephalopathy have been observed in some patients, usually elderly, treated at higher doses of PegIntron.
- Cardiovascular Events
- Cardiovascular events, which include hypotension, arrhythmia, tachycardia, cardiomyopathy, angina pectoris, and myocardial infarction, have been observed in patients treated with PegIntron. PegIntron should be used cautiously in patients with cardiovascular disease. Patients with a history of myocardial infarction and arrhythmic disorder who require PegIntron therapy should be closely monitored [see Warnings and Precautions (5.15)]. Patients with a history of significant or unstable cardiac disease should not be treated with PegIntron/ribavirin combination therapy [see ribavirin labeling].
- Endocrine Disorders
- PegIntron causes or aggravates hypothyroidism and hyperthyroidism. Hyperglycemia has been observed in patients treated with PegIntron. Diabetes mellitus, including cases of new onset Type 1 diabetes, has been observed in patients treated with alpha interferons, including PegIntron. Patients with these conditions who cannot be effectively treated by medication should not begin PegIntron therapy. Patients who develop these conditions during treatment and cannot be controlled with medication should not continue PegIntron therapy.
- Ophthalmologic Disorders
- Decrease or loss of vision, retinopathy including macular edema, retinal artery or vein thrombosis, retinal hemorrhages and cotton wool spots, optic neuritis, papilledema, and serous retinal detachment may be induced or aggravated by treatment with peginterferon alfa-2b or other alpha interferons. All patients should receive an eye examination at baseline. Patients with preexisting ophthalmologic disorders (e.g., diabetic or hypertensive retinopathy) should receive periodic ophthalmologic exams during interferon alpha treatment. Any patient who develops ocular symptoms should receive a prompt and complete eye examination. Peginterferon alfa-2b treatment should be discontinued in patients who develop new or worsening ophthalmologic disorders.
- Cerebrovascular Disorders
- Ischemic and hemorrhagic cerebrovascular events have been observed in patients treated with interferon alfa-based therapies, including PegIntron. Events occurred in patients with few or no reported risk factors for stroke, including patients less than 45 years of age. Because these are spontaneous reports, estimates of frequency cannot be made, and a causal relationship between interferon alfa-based therapies and these events is difficult to establish.
- Bone Marrow Toxicity
- PegIntron suppresses bone marrow function, sometimes resulting in severe cytopenias. PegIntron should be discontinued in patients who develop severe decreases in neutrophil or platelet counts [see Dosage and Administration (2.3)]. Ribavirin may potentiate the neutropenia induced by interferon alpha. Very rarely alpha interferons may be associated with aplastic anemia.
- Autoimmune Disorders
- Development or exacerbation of autoimmune disorders (e.g., thyroiditis, thrombotic thrombocytopenic purpura, idiopathic thrombocytopenic purpura, rheumatoid arthritis, interstitial nephritis, systemic lupus erythematosus, and psoriasis) has been observed in patients receiving PegIntron.
- PegIntron should be used with caution in patients with autoimmune disorders.
- Pancreatitis
- Fatal and nonfatal pancreatitis has been observed in patients treated with alpha interferon. PegIntron therapy should be suspended in patients with signs and symptoms suggestive of pancreatitis and discontinued in patients diagnosed with pancreatitis.
- Colitis
- Fatal and nonfatal ulcerative or hemorrhagic/ischemic colitis have been observed within 12 weeks of the start of alpha interferon treatment. Abdominal pain, bloody diarrhea, and fever are the typical manifestations. PegIntron treatment should be discontinued immediately in patients who develop these signs and symptoms. The colitis usually resolves within 1 to 3 weeks of discontinuation of alpha interferons.
- Pulmonary Disorders
- Dyspnea, pulmonary infiltrates, pneumonia, bronchiolitis obliterans, interstitial pneumonitis, pulmonary hypertension, and sarcoidosis, some resulting in respiratory failure or patient deaths, may be induced or aggravated by PegIntron or alpha interferon therapy. Recurrence of respiratory failure has been observed with interferon rechallenge. PegIntron combination treatment should be suspended in patients who develop pulmonary infiltrates or pulmonary function impairment. Patients who resume interferon treatment should be closely monitored.
- Because of the fever and other "flu-like" symptoms associated with PegIntron administration, it should be used cautiously in patients with debilitating medical conditions, such as those with a history of pulmonary disease (e.g., chronic obstructive pulmonary disease).
- Hepatic Failure
- Chronic Hepatitis C (CHC) patients with cirrhosis may be at risk of hepatic decompensation and death when treated with alpha interferons, including PegIntron. Cirrhotic CHC patients co-infected with HIV receiving highly active antiretroviral therapy (HAART) and alpha interferons with or without ribavirin appear to be at increased risk for the development of hepatic decompensation compared to patients not receiving HAART. During treatment, patients' clinical status and hepatic function should be closely monitored, and PegIntron treatment should be immediately discontinued if decompensation (Child-Pugh score greater than 6) is observed [see Contraindications (4)].
- Patients with Renal Insufficiency
- Increases in serum creatinine levels have been observed in patients with renal insufficiency receiving interferon alpha products, including PegIntron. Patients with impaired renal function should be closely monitored for signs and symptoms of interferon toxicity, including increases in serum creatinine, and PegIntron dosing should be adjusted accordingly or discontinued [see Clinical Pharmacology (12.3) and Dosage and Administration (2.3)]. PegIntron monotherapy should be used with caution in patients with creatinine clearance less than 50 mL/min; the potential risks should be weighed against the potential benefits in these patients. Combination therapy with ribavirin must not be used in patients with creatinine clearance less than 50 mL/min [see ribavirin labeling].
- Hypersensitivity
- Serious, acute hypersensitivity reactions (e.g., urticaria, angioedema, bronchoconstriction, anaphylaxis) and cutaneous eruptions (Stevens-Johnson syndrome, toxic epidermal necrolysis) have been rarely observed during alpha interferon therapy. If such a reaction develops during treatment with PegIntron, discontinue treatment and institute appropriate medical therapy immediately. Transient rashes do not necessitate interruption of treatment.
- Laboratory Tests
- PegIntron alone or in combination with ribavirin may cause severe decreases in neutrophil and platelet counts, and hematologic, endocrine (e.g., TSH), and hepatic abnormalities. Transient elevations in ALT (2- to 5-fold above baseline) were observed in 10% of subjects treated with PegIntron, and were not associated with deterioration of other liver functions. Triglyceride levels are frequently elevated in patients receiving alpha interferon therapy including PegIntron and should be periodically monitored.
- Patients on PegIntron or PegIntron/REBETOL combination therapy should have hematology and blood chemistry testing before the start of treatment and then periodically thereafter. In the adult clinical trial, complete blood counts (including hemoglobin, neutrophil, and platelet counts) and chemistries (including AST, ALT, bilirubin, and uric acid) were measured during the treatment period at Weeks 2, 4, 8, and 12, and then at 6-week intervals, or more frequently if abnormalities developed. In pediatric subjects, the same laboratory parameters were evaluated with additional assessment of hemoglobin at treatment Week 6. TSH levels were measured every 12 weeks during the treatment period. HCV-RNA should be measured periodically during treatment.
- Patients who have pre-existing cardiac abnormalities should have electrocardiograms done before treatment with PegIntron/ribavirin.
- Dental and Periodontal Disorders
- Dental and periodontal disorders have been reported in patients receiving PegIntron/REBETOL combination therapy. In addition, dry mouth could have a damaging effect on teeth and mucous membranes of the mouth during long-term treatment with the combination of REBETOL and PegIntron. Patients should brush their teeth thoroughly twice daily and have regular dental examinations. If vomiting occurs, patients should be advised to rinse out their mouth thoroughly afterwards.
- Triglycerides
- Elevated triglyceride levels have been observed in patients treated with interferon alpha, including PegIntron therapy. Hypertriglyceridemia may result in pancreatitis. Elevated triglyceride levels should be managed as clinically appropriate. Discontinuation of PegIntron therapy should be considered for patients with symptoms of potential pancreatitis, such as abdominal pain, nausea, or vomiting, and persistently elevated triglycerides (e.g., triglycerides greater than 1000 mg/dL).
- Impact on Growth — Pediatric Use
- Data on the effects of PegIntron plus REBETOL on growth come from an open-label trial in 107 subjects, 3 through 17 years of age, in which weight and height changes are compared to US normative population data. In general, the weight and height gain of pediatric subjects treated with PegIntron plus REBETOL lags behind that predicted by normative population data for the entire length of treatment. Severely inhibited growth velocity (less than 3rd percentile) was observed in 70% of the subjects while on treatment. Following treatment, rebound growth and weight gain occurred in most subjects. Long-term follow-up data in pediatric subjects, however, indicates that PegIntron in combination therapy with REBETOL may induce a growth inhibition that results in reduced adult height in some patients.
- Peripheral Neuropathy
- Peripheral neuropathy has been reported when alpha interferons were given in combination with telbivudine. In one clinical trial, an increased risk and severity of peripheral neuropathy was observed with the combination use of telbivudine and pegylated interferon alfa-2a as compared to telbivudine alone. The safety and efficacy of telbivudine in combination with interferons for the treatment of chronic hepatitis B has not been demonstrated.
Adverse Reactions
Clinical Trials Experience
- Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
- Clinical trials with PegIntron alone or in combination with REBETOL have been conducted in over 6900 subjects from 3 to 75 years of age.
- Serious adverse reactions have occurred in approximately 12% of subjects in clinical trials with PegIntron with or without REBETOL. The most common serious events occurring in subjects treated with PegIntron and REBETOL were depression and suicidal ideation [see Warnings and Precautions (5.2), each occurring at a frequency of less than 1%. The most common fatal events occurring in subjects treated with PegIntron and REBETOL were cardiac arrest, suicidal ideation, and suicide attempt, all occurring in less than 1% of subjects.
- Greater than 96% of all subjects in clinical trials experienced one or more adverse events. The most commonly reported adverse reactions in adult subjects receiving either PegIntron or PegIntron/REBETOL were injection-site inflammation/reaction, fatigue/asthenia, headache, rigors, fevers, nausea, myalgia, and emotional lability/irritability. The most common adverse events in pediatric subjects, ages 3 and older, were pyrexia, headache, vomiting, neutropenia, fatigue, anorexia, injection-site erythema, and abdominal pain.
Adults
- Study 1 compared PegIntron monotherapy with INTRON® A monotherapy. Study 2 compared combination therapy of PegIntron/REBETOL with combination therapy with INTRON A/REBETOL. In these clinical trials, nearly all subjects experienced one or more adverse reactions. Study 3 compared a PegIntron/weight-based REBETOL combination to a PegIntron/flat dose REBETOL regimen. Study 4 compared two PegIntron (1.5 mcg/kg/week and 1 mcg/kg/week) doses in combination with REBETOL and a third treatment group receiving Pegasys® (180 mcg/week)/Copegus® (1000-1200 mg/day).
- Adverse reactions that occurred in Studies 1 and 2 at greater than 5% incidence are provided in Table 8 by treatment group. Due to potential differences in ascertainment procedures, adverse reaction rate comparisons across trials should not be made. Table 9 summarizes the treatment-related adverse reactions in Study 4 that occurred at a greater than or equal to 10% incidence.
T8
T9
- The adverse reaction profile in Study 3, which compared PegIntron/weight-based REBETOL combination to a PegIntron/flat-dose REBETOL regimen, revealed an increased rate of anemia with weight-based dosing (29% vs. 19% for weight-based vs. flat-dose regimens, respectively). However, the majority of cases of anemia were mild and responded to dose reductions.
- The incidence of serious adverse reactions was comparable in all trials. In the PegIntron monotherapy trial (Study 1) the incidence of serious adverse reactions was similar (about 12%) in all treatment groups. In Study 2, the incidence of serious adverse reactions was 17% in the PegIntron/REBETOL groups compared to 14% in the INTRON A/REBETOL group. In Study 3, there was a similar incidence of serious adverse reactions reported for the weight-based REBETOL group (12%) and for the flat-dose REBETOL regimen.
- In many but not all cases, adverse reactions resolved after dose reduction or discontinuation of therapy. Some subjects experienced ongoing or new serious adverse reactions during the 6-month follow-up period.
- There have been 31 subject deaths that occurred during treatment or during follow-up in these clinical trials. In Study 1, there was 1 suicide in a subject receiving PegIntron monotherapy and 2 deaths among subjects receiving INTRON A monotherapy (1 murder/suicide and 1 sudden death). In Study 2, there was 1 suicide in a subject receiving PegIntron/REBETOL combination therapy, and 1 subject death in the INTRON A/REBETOL group (motor vehicle accident). In Study 3, there were 14 deaths, 2 of which were probable suicides, and 1 was an unexplained death in a person with a relevant medical history of depression. In Study 4, there were 12 deaths, 6 of which occurred in subjects receiving PegIntron/REBETOL combination therapy; 5 in the PegIntron 1.5 mcg/REBETOL arm (N=1019) and 1 in the PegIntron 1 mcg/REBETOL arm (n=1016); and 6 of which occurred in subjects receiving Pegasys/Copegus (N=1035). There were 3 suicides that occurred during the off-treatment follow-up period in subjects who received PegIntron (1.5 mcg/kg)/REBETOL combination therapy.
- In Studies 1 and 2, 10% to 14% of subjects receiving PegIntron, alone or in combination with REBETOL, discontinued therapy compared with 6% treated with INTRON A alone and 13% treated with INTRON A in combination with REBETOL. Similarly in Study 3, 15% of subjects receiving PegIntron in combination with weight-based REBETOL and 14% of subjects receiving PegIntron and flat-dose REBETOL discontinued therapy due to an adverse reaction. The most common reasons for discontinuation of therapy were related to known interferon effects of psychiatric, systemic (e.g., fatigue, headache), or gastrointestinal adverse reactions. In Study 4, 13% of subjects in the PegIntron 1.5 mcg/REBETOL arm, 10% in the PegIntron 1 mcg/REBETOL arm, and 13% in the Pegasys 180 mcg/Copegus arm discontinued therapy due to adverse events.
- In Study 2, dose reductions due to adverse reactions occurred in 42% of subjects receiving PegIntron (1.5 mcg/kg)/REBETOL and in 34% of those receiving INTRON A/REBETOL. The majority of subjects (57%) weighing 60 kg or less receiving PegIntron (1.5 mcg/kg)/REBETOL required dose reduction. Reduction of interferon was dose-related (PegIntron 1.5 mcg/kg more than PegIntron 0.5 mcg/kg or INTRON A), 40%, 27%, 28%, respectively. Dose reduction for REBETOL was similar across all three groups, 33% to 35%. The most common reasons for dose modifications were neutropenia (18%) or anemia (9%). Other common reasons included depression, fatigue, nausea, and thrombocytopenia. In Study 3, dose modifications due to adverse reactions occurred more frequently with weight-based dosing (WBD) compared to flat dosing (29% and 23%, respectively). In Study 4, 16% of subjects had a dose reduction of PegIntron to 1 mcg/kg in combination with REBETOL, with an additional 4% requiring the second dose reduction of PegIntron to 0.5 mcg/kg due to adverse events, compared to 15% of subjects in the Pegasys/Copegus arm, who required a dose reduction to 135 mcg/week with Pegasys, with an additional 7% requiring a second dose reduction to 90 mcg/week with Pegasys.
- In the PegIntron/REBETOL combination trials the most common adverse reactions were psychiatric, which occurred among 77% of subjects in Study 2 and 68% to 69% of subjects in Study 3. These psychiatric adverse reactions included most commonly depression, irritability, and insomnia, each reported by approximately 30% to 40% of subjects in all treatment groups. Suicidal behavior (ideation, attempts, and suicides) occurred in 2% of all subjects during treatment or during follow-up after treatment cessation [see Warnings and Precautions (5.2)]. In Study 4, psychiatric adverse reactions occurred in 58% of subjects in the PegIntron 1.5 mcg/REBETOL arm, 55% of subjects in the PegIntron 1 mcg/REBETOL arm, and 57% of subjects in the Pegasys 180 mcg/Copegus arm.
- PegIntron induced fatigue or headache in approximately two-thirds of subjects, with fever or rigors in approximately half of the subjects. The severity of some of these systemic symptoms (e.g., fever and headache) tended to decrease as treatment continued. In Studies 1 and 2, application site inflammation and reaction (e.g., bruise, itchiness, and irritation) occurred at approximately twice the incidence with PegIntron therapies (in up to 75% of subjects) compared with INTRON A. However, injection-site pain was infrequent (2-3%) in all groups. In Study 3, there was a 23% to 24% incidence overall for injection-site reactions or inflammation.
- In Study 2, many subjects continued to experience adverse reactions several months after discontinuation of therapy. By the end of the 6-month follow-up period, the incidence of ongoing adverse reactions by body class in the PegIntron 1.5/REBETOL group was 33% (psychiatric), 20% (musculoskeletal), and 10% (for endocrine and for GI). In approximately 10% to 15% of subjects, weight loss, fatigue, and headache had not resolved.
- Individual serious adverse reactions in Study 2 occurred at a frequency less than or equal to 1% and included suicide attempt, suicidal ideation, severe depression; psychosis, aggressive reaction, relapse of drug addiction/overdose; nerve palsy (facial, oculomotor); cardiomyopathy, myocardial infarction, angina, pericardial effusion, retinal ischemia, retinal artery or vein thrombosis, blindness, decreased visual acuity, optic neuritis, transient ischemic attack, supraventricular arrhythmias, loss of consciousness; neutropenia, infection (sepsis, pneumonia, abscess, cellulitis); emphysema, bronchiolitis obliterans, pleural effusion, gastroenteritis, pancreatitis, gout, hyperglycemia, hyperthyroidism and hypothyroidism, autoimmune thrombocytopenia with or without purpura, rheumatoid arthritis, interstitial nephritis, lupus-like syndrome, sarcoidosis, aggravated psoriasis; urticaria, injection-site necrosis, vasculitis, and phototoxicity.
- Subjects receiving PegIntron/REBETOL as re-treatment after failing a previous interferon combination regimen reported adverse reactions similar to those previously associated with this regimen during clinical trials of treatment-naïve subjects.
Pediatric Subjects
- In general, the adverse-reaction profile in the pediatric population was similar to that observed in adults. In the pediatric trial, the most prevalent adverse reactions in all subjects were pyrexia (80%), headache (62%), neutropenia (33%), fatigue (30%), anorexia (29%), injection-site erythema (29%), and vomiting (27%). The majority of adverse reactions reported in the trial were mild or moderate in severity. Severe adverse reactions were reported in 7% (8/107) of all subjects and included injection-site pain (1%), pain in extremity (1%), headache (1%), neutropenia (1%), and pyrexia (4%). Important adverse reactions that occurred in this subject population were nervousness (7%; 7/107), aggression (3%; 3/107), anger (2%; 2/107), and depression (1%; 1/107). Five subjects received levothyroxine treatment; three with clinical hypothyroidism and two with asymptomatic TSH elevations. Weight and height gain of pediatric subjects treated with PegIntron plus REBETOL lagged behind that predicted by normative population data for the entire length of treatment. Severely inhibited growth velocity (less than 3rd percentile) was observed in 70% of the subjects while on treatment.
- Dose modifications were required in 25% of subjects, most commonly for anemia, neutropenia, and weight loss. Two subjects (2%; 2/107) discontinued therapy as the result of an adverse reaction.
- Adverse reactions that occurred with a greater than or equal to 10% incidence in the pediatric trial subjects are provided in Table 10.
T10
- Ninety-four of 107 subjects enrolled in a 5 year long-term follow-up trial. The long-term effects on growth were less in those subjects treated for 24 weeks than those treated for 48 weeks. Twenty-four percent of subjects (11/46) treated for 24 weeks and 40% of subjects (19/48) treated for 48 weeks had a >15 percentile height-for-age decrease from pre-treatment to the end of the 5 year long-term follow-up compared to pre-treatment baseline percentiles. Eleven percent of subjects (5/46) treated for 24 weeks and 13% of subjects (6/48) treated for 48 weeks were observed to have a decrease from pre-treatment baseline of >30 height-for-age percentiles to the end of the 5 year long-term follow-up. While observed across all age groups, the highest risk for reduced height at the end of long-term follow-up appeared to correlate with initiation of combination therapy during the years of expected peak growth velocity.
Laboratory Values
Adults
- Changes in selected laboratory values during treatment with PegIntron alone or in combination with REBETOL treatment are described below. Decreases in hemoglobin, neutrophils, and platelets may require dose reduction or permanent discontinuation from therapy.
- Hemoglobin. Hemoglobin levels decreased to less than 11 g/dL in about 30% of subjects in Study 2. In Study 3, 47% of subjects receiving WBD REBETOL and 33% on flat-dose REBETOL had decreases in hemoglobin levels less than 11 g/dL. Reductions in hemoglobin to less than 9 g/dL occurred more frequently in subjects receiving WBD compared to flat dosing (4% and 2%, respectively). In Study 2, dose modification was required in 9% and 13% of subjects in the PegIntron/REBETOL and INTRON A/REBETOL groups. In Study 4, subjects receiving PegIntron (1.5 mcg/kg)/REBETOL had decreases in hemoglobin levels to between 8.5 to less than 10 g/dL (28%) and to less than 8.5 g/dL (3%), whereas in subjects receiving Pegasys 180 mcg/Copegus these decreases occurred in 26% and 4% of subjects, respectively. Hemoglobin levels became stable by treatment Weeks 4 to 6 on average. The typical pattern observed was a decrease in hemoglobin levels by treatment Week 4 followed by stabilization and a plateau, which was maintained to the end of treatment. In the PegIntron monotherapy trial, hemoglobin decreases were generally mild and dose modifications were rarely necessary [see Dosage and Administration (2.3)].
- Neutrophils. Decreases in neutrophil counts were observed in a majority of subjects treated with PegIntron alone (70%) or as combination therapy with REBETOL in Study 2 (85%) and INTRON A/REBETOL (60%). Severe potentially life-threatening neutropenia (less than 0.5 × 109/L) occurred in 1% of subjects treated with PegIntron monotherapy, 2% of subjects treated with INTRON A/REBETOL, and in approximately 4% of subjects treated with PegIntron/REBETOL in Study 2. Two percent of subjects receiving PegIntron monotherapy and 18% of subjects receiving PegIntron/REBETOL in Study 2 required modification of interferon dosage. Few subjects (less than 1%) required permanent discontinuation of treatment. Neutrophil counts generally returned to pretreatment levels 4 weeks after cessation of therapy [see Dosage and Administration (2.3)].
- Platelets. Platelet counts decreased to less than 100,000/mm3 in approximately 20% of subjects treated with PegIntron alone or with REBETOL and in 6% of subjects treated with INTRON A/REBETOL. Severe decreases in platelet counts (less than 50,000/mm3) occur in less than 4% of subjects. Patients may require discontinuation or dose modification as a result of platelet decreases [see Dosage and Administration (2.3)]. In Study 2, 1% or 3% of subjects required dose modification of INTRON A or PegIntron, respectively. Platelet counts generally returned to pretreatment levels 4 weeks after the cessation of therapy.
- Triglycerides. Elevated triglyceride levels have been observed in patients treated with interferon alphas, including PegIntron.
- Thyroid Function. Development of TSH abnormalities, with or without clinical manifestations, is associated with interferon therapies. In Study 2, clinically apparent thyroid disorders occurred among subjects treated with either INTRON A or PegIntron (with or without REBETOL) at a similar incidence (5% for hypothyroidism and 3% for hyperthyroidism). Subjects developed new-onset TSH abnormalities while on treatment and during the follow-up period. At the end of the follow-up period, 7% of subjects still had abnormal TSH values.
- Bilirubin and Uric Acid. In Study 2, 10% to 14% of subjects developed hyperbilirubinemia and 33% to 38% developed hyperuricemia in association with hemolysis. Six subjects developed mild to moderate gout.
Pediatric Subjects
- Decreases in hemoglobin, white blood cells, platelets, and neutrophils may require dose reduction or permanent discontinuation from therapy. Changes in selected laboratory values during treatment of 107 pediatric subjects with PegIntron/REBETOL combination therapy are described in Table 11. Most of the changes in laboratory values in this trial were mild or moderate.
T11
Postmarketing Experience
- The following adverse reactions have been identified during post-approval use of PegIntron therapy. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Blood and Lymphatic System Disorders
Pure red cell aplasia, thrombotic thrombocytopenic purpura
Cardiac Disorders
Palpitations
Ear and Labyrinth Disorders
Hearing loss, vertigo, hearing impairment
Endocrine Disorders
Diabetic ketoacidosis, diabetes
Eye Disorders
Vogt-Koyanagi-Harada syndrome, serous retinal detachment
Gastrointestinal Disorders
Aphthous stomatitis
General Disorders and Administration Site Conditions
Asthenic conditions (including asthenia, malaise, fatigue)
Immune System Disorders
Cases of acute hypersensitivity reactions (including anaphylaxis, angioedema, urticaria); Stevens-Johnson syndrome, toxic epidermal necrolysis, systemic lupus erythematosus, erythema multiforme
Infections and Infestations
Bacterial infection including sepsis
Metabolism and Nutrition Disorders
Dehydration, hypertriglyceridemia
Musculoskeletal and Connective Tissue Disorders
Rhabdomyolysis, myositis
Nervous System Disorders
Seizures, memory loss, peripheral neuropathy, paraesthesia, migraine headache
Psychiatric Disorders
Homicidal ideation
Respiratory, Thoracic, and Mediastinal Disorders
Pulmonary hypertension
Renal and Urinary Disorders
Renal failure, renal insufficiency
Skin and Subcutaneous Tissue Disorders
Psoriasis
Vascular Disorders
Hypertension, hypotension
Drug Interactions
- Drugs Metabolized by Cytochrome P-450
- When administering PegIntron with medications metabolized by CYP2C8/9 (e.g., warfarin and phenytoin) or CYP2D6 (e.g., flecainide), the therapeutic effect of these substrates may be decreased.
- Methadone
- PegIntron may increase methadone concentrations [see Clinical Pharmacology (12.3)]. The clinical significance of this finding is unknown; however, patients should be monitored for signs and symptoms of increased narcotic effect.
- Use with Ribavirin (Nucleoside Analogues)
- Hepatic decompensation (some fatal) has occurred in cirrhotic HIV/HCV co-infected patients receiving combination antiretroviral therapy for HIV and interferon alpha and ribavirin. Adding treatment with alpha interferons alone or in combination with ribavirin may increase the risk in this patient subset. Patients receiving interferon with ribavirin and nucleoside reverse transcriptase inhibitors (NRTIs) should be closely monitored for treatment- associated toxicities, especially hepatic decompensation and anemia. Discontinuation of NRTIs should be considered as medically appropriate [see labeling for individual NRTI product]. Dose reduction or discontinuation of interferon, ribavirin, or both should also be considered if worsening clinical toxicities are observed, including hepatic decompensation (e.g., Child-Pugh greater than 6).
- Stavudine, Lamivudine, and Zidovudine
- In vitro studies have shown ribavirin can reduce the phosphorylation of pyrimidine nucleoside analogues such as stavudine, lamivudine, and zidovudine. In a trial with another pegylated interferon alpha, no evidence of a pharmacokinetic or pharmacodynamic (e.g., loss of HIV/HCV virologic suppression) interaction was seen when ribavirin was co-administered with zidovudine, lamivudine, or stavudine in HIV/HCV co-infected subjects.
- HIV/HCV co-infected subjects who were administered zidovudine in combination with pegylated interferon alpha and ribavirin developed severe neutropenia (ANC less than 500) and severe anemia (hemoglobin less than 8 g/dL) more frequently than similar subjects not receiving zidovudine.
- Didanosine
- Co-administration of ribavirin and didanosine is not recommended. Reports of fatal hepatic failure, as well as peripheral neuropathy, pancreatitis, and symptomatic hyperlactatemia/lactic acidosis have been reported in clinical trials.
Use in Specific Populations
Pregnancy
- Pregnancy Category C
- Nonpegylated interferon alfa-2b has been shown to have abortifacient effects in Macaca mulatta (rhesus monkeys) at 15 and 30 million IU/kg (estimated human equivalent of 5 and 10 million IU/kg, based on body surface area adjustment for a 60-kg adult). PegIntron should be assumed to also have abortifacient potential. There are no adequate and well-controlled trials in pregnant women. PegIntron therapy is to be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Therefore, PegIntron is recommended for use in fertile women only when they are using effective contraception during the treatment period.
- Use with Ribavirin
- Pregnancy Category X: Significant teratogenic and/or embryocidal effects have been demonstrated in all animal species exposed to ribavirin. Ribavirin therapy is contraindicated in women who are pregnant and in the male partners of women who are pregnant.
- A Ribavirin Pregnancy Registry has been established to monitor maternal-fetal outcomes of pregnancies in female patients and female partners of male patients exposed to ribavirin during treatment and for 6 months following cessation of treatment. Physicians and patients are encouraged to report such cases by calling 1-800-593-2214.
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Pegylated interferon alfa-2b in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Pegylated interferon alfa-2b during labor and delivery.
Nursing Mothers
- It is not known whether the components of PegIntron and/or ribavirin are excreted in human milk. Studies in mice have shown that mouse interferons are excreted in breast milk. Because of the potential for adverse reactions from the drug in nursing infants, a decision must be made whether to discontinue nursing or discontinue the PegIntron and ribavirin treatment, taking into account the importance of the therapy to the mother.
Pediatric Use
- Safety and effectiveness in pediatric patients below the age of 3 years have not been established. Clinical trials in pediatric subjects less than 3 years of age are not considered feasible due to the small proportion of patients in this age group requiring treatment for CHC.
- Long-term follow-up data in pediatric subjects indicates that PegIntron in combination with REBETOL may induce a growth inhibition that results in reduced height in some patients.
Geriatic Use
- In general, younger patients tend to respond better than older patients to interferon-based therapies. Clinical trials of PegIntron alone or in combination with REBETOL did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently than younger subjects. Treatment with alpha interferons, including PegIntron, is associated with neuropsychiatric, cardiac, pulmonary, GI, and systemic (flu-like) adverse effects. Because these adverse reactions may be more severe in the elderly, caution should be exercised in the use of PegIntron in this population. This drug is known to be substantially excreted by the kidney. Because elderly patients are more likely to have decreased renal function, the risk of toxic reactions to this drug may be greater in patients with impaired renal function. When using PegIntron/ ribavirin therapy, refer also to the ribavirin labeling.
Gender
There is no FDA guidance on the use of Pegylated interferon alfa-2b with respect to specific gender populations.
Race
There is no FDA guidance on the use of Pegylated interferon alfa-2b with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Pegylated interferon alfa-2b in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Pegylated interferon alfa-2b in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Pegylated interferon alfa-2b in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Pegylated interferon alfa-2b in patients who are immunocompromised.
Administration and Monitoring
Administration
- Subcutaneous
Monitoring
There is limited information regarding Monitoring of Pegylated interferon alfa-2b in the drug label.
IV Compatibility
There is limited information regarding IV Compatibility of Pegylated interferon alfa-2b in the drug label.
Overdosage
Acute Overdose
- There is limited experience with overdosage. In the clinical trials, a few subjects accidentally received a dose greater than that prescribed. There were no instances in which a participant in the monotherapy or combination therapy trials received more than 10.5 times the intended dose of PegIntron. The maximum dose received by any subject was 3.45 mcg/kg weekly over a period of approximately 12 weeks. The maximum known overdosage of ribavirin was an intentional ingestion of 10 g (fifty 200 mg capsules). There were no serious reactions attributed to these overdosages. In cases of overdosing, symptomatic treatment and close observation of the patient are recommended.
Chronic Overdose
There is limited information regarding Chronic Overdose of Pegylated interferon alfa-2b in the drug label.
Pharmacology
Pegylated interferon alfa-2b
| |
| Systematic (IUPAC) name | |
| PEGylated human interferon alpha 2b | |
| Identifiers | |
| CAS number | |
| ATC code | L03 |
| PubChem | ? |
| DrugBank | |
| Chemical data | |
| Formula | Template:OrganicBox atomTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox |
| Mol. mass | 19269.1 g/mol |
| Pharmacokinetic data | |
| Bioavailability | ? |
| Metabolism | ? |
| Half life | 22–60 hrs |
| Excretion | ? |
| Therapeutic considerations | |
| Pregnancy cat. |
contraindicated[1] |
| Legal status | |
| Routes | ? |
Mechanism of Action
- The biological activity of PegIntron is derived from its interferon alfa-2b moiety. Peginterferon alfa-2b binds to and activates the human type 1 interferon receptor. Upon binding, the receptor subunits dimerize, and activate multiple intracellular signal transduction pathways. Signal transduction is initially mediated by the JAK/STAT activation, which may occur in a wide variety of cells. Interferon receptor activation also activates NFκB in many cell types. Given the diversity of cell types that respond to interferon alfa-2b, and the multiplicity of potential intracellular responses to interferon receptor activation, peginterferon alfa-2b is expected to have pleiotropic biological effects in the body.
- The mechanism by which ribavirin contributes to its antiviral efficacy in the clinic is not fully understood. Ribavirin has direct antiviral activity in tissue culture against many RNA viruses. Ribavirin increases the mutation frequency in the genomes of several viruses and ribavirin triphosphate inhibits HCV polymerase in a biochemical reaction.
- Antiviral Activity
- The anti-HCV activity of interferon was demonstrated in cell culture using self-replicating HCV-RNA (HCV replicon cells) or HCV infection and resulted in an effective concentration (EC50) value of 1 to 10 IU/mL.
- The antiviral activity of ribavirin in the HCV-replicon is not well understood and has not been defined because of the cellular toxicity of ribavirin.
- Resistance
- HCV genotypes show wide variability in their response to pegylated recombinant human interferon/ribavirin therapy. Genetic changes associated with the variable response have not been identified.
- Cross-resistance
- There is no reported cross-resistance between pegylated/nonpegylated interferons and ribavirin.
Structure
- PegIntron, peginterferon alfa-2b, is a covalent conjugate of recombinant alfa-2b interferon with monomethoxy polyethylene glycol (PEG). The average molecular weight of the PEG portion of the molecule is 12,000 daltons. The average molecular weight of the PegIntron molecule is approximately 31,000 daltons. The specific activity of peginterferon alfa-2b is approximately 0.7 × 108 IU/mg protein.
- Interferon alfa-2b is a water-soluble protein with a molecular weight of 19,271 daltons produced by recombinant DNA techniques. It is obtained from the bacterial fermentation of a strain of Escherichia coli bearing a genetically engineered plasmid containing an interferon gene from human leukocytes.
- PegIntron is supplied in both vials and the REDIPEN single-use pre-filled pen for subcutaneous use.
- Vials
- Each vial contains either 74 mcg, 118.4 mcg, 177.6 mcg, or 222 mcg of PegIntron as a white to off-white tablet-like solid that is whole/in pieces or as a loose powder, and 1.11 mg dibasic sodium phosphate anhydrous, 1.11 mg monobasic sodium phosphate dihydrate, 59.2 mg sucrose, and 0.074 mg polysorbate 80. Following reconstitution with 0.7 mL of the supplied Sterile Water for Injection USP, each vial contains PegIntron at strengths of either 50 mcg per 0.5 mL, 80 mcg per 0.5 mL, 120 mcg per 0.5 mL, or 150 mcg per 0.5 mL.
- REDIPEN single-use pre-filled pen
- REDIPEN pre-filled pen is a dual-chamber glass cartridge containing lyophilized PegIntron as a white to off-white tablet or powder that is whole or in pieces in the sterile active chamber and a second chamber containing Sterile Water for Injection USP. Each PegIntron REDIPEN pre-filled pen contains either 67.5 mcg, 108 mcg, 162 mcg, or 202.5 mcg of PegIntron, and 1.013 mg dibasic sodium phosphate anhydrous, 1.013 mg monobasic sodium phosphate dihydrate, 54 mg sucrose, and 0.0675 mg polysorbate 80. Each cartridge is reconstituted to allow for the administration of up to 0.5 mL of solution. Following reconstitution, each REDIPEN pre-filled pen contains PegIntron at strengths of either 50 mcg per 0.5 mL, 80 mcg per 0.5 mL, 120 mcg per 0.5 mL, or 150 mcg per 0.5 mL for a single use. Because a small volume of reconstituted solution is lost during preparation of PegIntron, each REDIPEN pre-filled pen contains an excess amount of PegIntron powder and diluent to ensure delivery of the labeled dose.
This image is provided by the National Library of Medicine.

Pharmacodynamics
- The pharmacodynamic effects of peginterferon alfa-2b include inhibition of viral replication in virus-infected cells, the suppression of cell cycle progression/cell proliferation, induction of apoptosis, anti-angiogenic activities, and numerous immunomodulating activities, such as enhancement of the phagocytic activity of macrophages, activation of NK cells, stimulation of cytotoxic T-lymphocytes, and the upregulation of the Th1 T-helper cell subset.
- PegIntron raises concentrations of effector proteins such as serum neopterin and 2'5' oligoadenylate synthetase, raises body temperature, and causes reversible decreases in leukocyte and platelet counts. The correlation between the in vitro and in vivo pharmacologic and pharmacodynamic and clinical effects is unknown.
Pharmacokinetics
- Following a single subcutaneous dose of PegIntron, the mean absorption half-life (t ½ ka) was 4.6 hours. Maximal serum concentrations (Cmax) occur between 15 and 44 hours postdose, and are sustained for up to 48 to 72 hours. The Cmax and AUC measurements of PegIntron increase in a dose-related manner. After multiple dosing, there is an increase in bioavailability of PegIntron. Week 48 mean trough concentrations (320 pg/mL; range 0, 2960) are approximately 3-fold higher than Week 4 mean trough concentrations (94 pg/mL; range 0, 416). The mean PegIntron elimination half-life is approximately 40 hours (range 22-60 hours) in patients with HCV infection. The apparent clearance of PegIntron is estimated to be approximately 22 mL/hr∙kg. Renal elimination accounts for 30% of the clearance.
- Pegylation of interferon alfa-2b produces a product (PegIntron) whose clearance is lower than that of nonpegylated interferon alfa-2b. When compared to INTRON A, PegIntron (1 mcg/kg) has approximately a 7-fold lower mean apparent clearance and a 5-fold greater mean half-life, permitting a reduced dosing frequency. At effective therapeutic doses, PegIntron has approximately 10-fold greater Cmax and 50-fold greater AUC than interferon alfa-2b.
- Renal Dysfunction
- Following multiple dosing of PegIntron (1 mcg/kg subcutaneously given every week for 4 weeks) the clearance of PegIntron is reduced by a mean of 17% in subjects with moderate renal impairment (creatinine clearance 30-49 mL/min) and by a mean of 44% in subjects with severe renal impairment (creatinine clearance 10-29 mL/min) compared to subjects with normal renal function. Clearance was similar in subjects with severe renal impairment not on dialysis and subjects who are receiving hemodialysis. The dose of PegIntron for monotherapy should be reduced in patients with moderate or severe renal impairment. REBETOL should not be used in patients with creatinine clearance less than 50 mL/min.
- Gender
- During the 48-week treatment period with PegIntron, no differences in the pharmacokinetic profiles were observed between male and female subjects with chronic hepatitis C infection.
- Geriatric Patients
- The pharmacokinetics of geriatric subjects (65 years of age and older) treated with a single subcutaneous dose of 1 mcg/kg of PegIntron were similar in Cmax, AUC, clearance, or elimination half-life as compared to younger subjects (28-44 years of age).
- Pediatric Patients
- Population pharmacokinetics for PegIntron and REBETOL (capsules and oral solution) were evaluated in pediatric subjects with chronic hepatitis C between 3 and 17 years of age. In pediatric patients receiving PegIntron 60 mcg/m2/week subcutaneously, exposure may be approximately 50% higher than observed in adults receiving 1.5 mcg/kg/week subcutaneously. The pharmacokinetics of REBETOL (dose-normalized) in this trial were similar to those reported in a prior trial of REBETOL in combination with INTRON A in pediatric subjects and in adults.
- Effect of Food on Absorption of Ribavirin
- Both AUCtf and Cmax increased by 70% when REBETOL capsules were administered with a high-fat meal (841 kcal, 53.8 g fat, 31.6 g protein, and 57.4 g carbohydrate) in a single-dose pharmacokinetic trial.
- Drug Interactions
- Drugs Metabolized by Cytochrome P-450
- The pharmacokinetics of representative drugs metabolized by CYP1A2 (caffeine), CYP2C8/9 (tolbutamide), CYP2D6 (dextromethorphan), CYP3A4 (midazolam), and N-acetyltransferase (dapsone) were studied in 22 subjects with chronic hepatitis C who received PegIntron (1.5 mcg/kg) once weekly for 4 weeks. PegIntron treatment resulted in a 28% (mean) increase in a measure of CYP2C8/9 activity. PegIntron treatment also resulted in a 66% (mean) increase in a measure of CYP2D6 activity; however, the effect was variable as 13 subjects had an increase, 5 subjects had a decrease, and 4 subjects had no significant change.
- No significant effect was observed on the pharmacokinetics of representative drugs metabolized by CYP1A2, CYP3A4, or N-acetyltransferase. The effects of PegIntron on CYP2C19 activity were not assessed.
- Methadone
- The pharmacokinetics of concomitant administration of methadone and PegIntron were evaluated in 18 PegIntron-naïve chronic hepatitis C subjects receiving 1.5 mcg/kg PegIntron subcutaneously weekly. All subjects were on stable methadone maintenance therapy receiving greater than or equal to 40 mg/day prior to initiating PegIntron. Mean methadone AUC was approximately 16% higher after 4 weeks of PegIntron treatment as compared to baseline. In 2 subjects, methadone AUC was approximately double after 4 weeks of PegIntron treatment as compared to baseline.
- Use with Ribavirin
- Zidovudine, Lamivudine, and Stavudine
- Ribavirin has been shown in vitro to inhibit phosphorylation of zidovudine, lamivudine, and stavudine. However, in a trial with another pegylated interferon in combination with ribavirin, no pharmacokinetic (e.g., plasma concentrations or intracellular triphosphorylated active metabolite concentrations) or pharmacodynamic (e.g., loss of HIV/HCV virologic suppression) interaction was observed when ribavirin and lamivudine (n=18), stavudine (n=10), or zidovudine (n=6) were co-administered as part of a multi-drug regimen to HIV/HCV co-infected subjects.
- Didanosine
- Exposure to didanosine or its active metabolite (dideoxyadenosine 5'- triphosphate) is increased when didanosine is co-administered with ribavirin, which could cause or worsen clinical toxicities.
Nonclinical Toxicology
- Carcinogenesis and Mutagenesis
- PegIntron has not been tested for its carcinogenic potential. Neither PegIntron nor its components, interferon or methoxypolyethylene glycol, caused damage to DNA when tested in the standard battery of mutagenesis assays, in the presence and absence of metabolic activation.
- Use with Ribavirin: See ribavirin labeling for additional warnings relevant to PegIntron therapy in combination with ribavirin.
- Impairment of Fertility
- PegIntron may impair human fertility. Irregular menstrual cycles were observed in female cynomolgus monkeys given subcutaneous injections of 4239 mcg/m2 PegIntron alone every other day for 1 month (approximately 345 times the recommended weekly human dose based upon body surface area). These effects included transiently decreased serum levels of estradiol and progesterone, suggestive of anovulation. Normal menstrual cycles and serum hormone levels resumed in these animals 2 to 3 months following cessation of PegIntron treatment. Every other day dosing with 262 mcg/m2 (approximately 21 times the weekly human dose) had no effects on cycle duration or reproductive hormone status. The effects of PegIntron on male fertility have not been studied.
Clinical Studies
Chronic Hepatitis C in Adults
- PegIntron Monotherapy — Study 1
- A randomized trial compared treatment with PegIntron (0.5, 1, or 1.5 mcg/kg once weekly subcutaneously) to treatment with INTRON A (3 million units 3 times weekly subcutaneously) in 1219 adults with chronic hepatitis from HCV infection. The subjects were not previously treated with interferon alpha, had compensated liver disease, detectable HCV-RNA, elevated ALT, and liver histopathology consistent with chronic hepatitis. Subjects were treated for 48 weeks and were followed for 24 weeks post-treatment.
- Seventy percent of all subjects were infected with HCV genotype 1, and 74 percent of all subjects had high baseline levels of HCV-RNA (more than 2 million copies per mL of serum), two factors known to predict poor response to treatment.
- Response to treatment was defined as undetectable HCV-RNA and normalization of ALT at 24 weeks post-treatment. The response rates to the 1 and 1.5 mcg/kg PegIntron doses were similar (approximately 24%) to each other and were both higher than the response rate to INTRON A (12%) (see Table 13).
T13
- Subjects with both viral genotype 1 and high serum levels of HCV-RNA at baseline were less likely to respond to treatment with PegIntron. Among subjects with the two unfavorable prognostic variables, 8% (12/157) responded to PegIntron treatment and 2% (4/169) responded to INTRON A. Doses of PegIntron higher than the recommended dose did not result in higher response rates in these subjects. Subjects receiving PegIntron with viral genotype 1 had a response rate of 14% (28/199) while subjects with other viral genotypes had a 45% (43/96) response rate.
- Ninety-six percent of the responders in the PegIntron groups and 100% of responders in the INTRON A group first cleared their viral RNA by Week 24 of treatment [see Dosage and Administration (2.1)].
- The treatment response rates were similar in men and women. Response rates were lower in African-American and Hispanic subjects and higher in Asians compared to Caucasians. Although African Americans had a higher proportion of poor prognostic factors compared to Caucasians, the number of non-Caucasians studied (9% of the total) was insufficient to allow meaningful conclusions about differences in response rates after adjusting for prognostic factors.
- Liver biopsies were obtained before and after treatment in 60% of subjects. A modest reduction in inflammation compared to baseline that was similar in all 4 treatment groups was observed.
- PegIntron/REBETOL Combination Therapy — Study 2
- A randomized trial compared treatment with two PegIntron/REBETOL regimens [PegIntron 1.5 mcg/kg subcutaneously once weekly/REBETOL 800 mg orally daily (in divided doses); PegIntron 1.5 mcg/kg subcutaneously once weekly for 4 weeks then 0.5 mcg/kg subcutaneously once weekly for 44 weeks/REBETOL 1000 or 1200 mg orally daily (in divided doses)] with INTRON A [3 MIU subcutaneously thrice weekly/REBETOL 1000 or 1200 mg orally daily (in divided doses)] in 1530 adults with chronic hepatitis C. Interferon-naïve subjects were treated for 48 weeks and followed for 24 weeks post-treatment. Eligible subjects had compensated liver disease, detectable HCV-RNA, elevated ALT, and liver histopathology consistent with chronic hepatitis.
- Response to treatment was defined as undetectable HCV-RNA at 24 weeks post-treatment. The response rate to the PegIntron 1.5 mcg/kg plus REBETOL 800 mg dose was higher than the response rate to INTRON A/REBETOL (see Table 14). The response rate to PegIntron 1.5→0.5 mcg/kg/REBETOL was essentially the same as the response to INTRON A/REBETOL (data not shown).
t14
- Subjects with viral genotype 1, regardless of viral load, had a lower response rate to PegIntron (1.5 mcg/kg)/REBETOL (800 mg) compared to subjects with other viral genotypes. Subjects with both poor prognostic factors (genotype 1 and high viral load) had a response rate of 30% (78/256) compared to a response rate of 29% (71/247) with INTRON A/REBETOL.
- Subjects with lower body weight tended to have higher adverse reaction rates and higher response rates than subjects with higher body weights. Differences in response rates between treatment arms did not substantially vary with body weight.
- Treatment response rates with PegIntron/REBETOL were 49% in men and 56% in women. Response rates were lower in African American and Hispanic subjects and higher in Asians compared to Caucasians. Although African Americans had a higher proportion of poor prognostic factors compared to Caucasians, the number of non-Caucasians studied (11% of the total) was insufficient to allow meaningful conclusions about differences in response rates after adjusting for prognostic factors in this trial.
- Liver biopsies were obtained before and after treatment in 68% of subjects. Compared to baseline, approximately two-thirds of subjects in all treatment groups were observed to have a modest reduction in inflammation.
- PegIntron/REBETOL Combination Therapy — Study 3
- In a large United States community-based trial, 4913 subjects with chronic hepatitis C were randomized to receive PegIntron 1.5 mcg/kg subcutaneously once weekly in combination with a REBETOL dose of 800 to 1400 mg (weight-based dosing [WBD]) or 800 mg (flat) orally daily (in divided doses) for 24 or 48 weeks based on genotype. Response to treatment was defined as undetectable HCV-RNA (based on an assay with a lower limit of detection of 125 IU/mL) at 24 weeks post-treatment.
- Treatment with PegIntron 1.5 mcg/kg and REBETOL 800 to 1400 mg resulted in a higher sustained virologic response compared to PegIntron in combination with a flat 800 mg daily dose of REBETOL. Subjects weighing greater than 105 kg obtained the greatest benefit with WBD, although a modest benefit was also observed in subjects weighing greater than 85 to 105 kg (see Table 15). The benefit of WBD in subjects weighing greater than 85 kg was observed with HCV genotypes 1-3. Insufficient data were available to reach conclusions regarding other genotypes. Use of WBD resulted in an increased incidence of anemia.
T15
- A total of 1552 subjects weighing greater than 65 kg in Study 3 had genotype 2 or 3 and were randomized to 24 or 48 weeks of therapy. No additional benefit was observed with the longer treatment duration.
- PegIntron/REBETOL Combination Therapy — Study 4
- A large randomized trial compared the safety and efficacy of treatment for 48 weeks with two PegIntron/REBETOL regimens [PegIntron 1.5 mcg/kg and 1 mcg/kg subcutaneously once weekly both in combination with REBETOL 800 to 1400 mg PO daily (in two divided doses)] and Pegasys 180 mcg subcutaneously once weekly in combination with Copegus 1000 to 1200 mg PO daily (in two divided doses) in 3070 treatment-naïve adults with chronic hepatitis C genotype 1. In this trial, lack of early virologic response (undetectable HCV-RNA or greater than or equal to 2 log10 reduction from baseline) by treatment Week 12 was the criterion for discontinuation of treatment. SVR was defined as undetectable HCV-RNA (Roche COBAS TaqMan assay, a lower limit of quantitation of 27 IU/mL) at 24 weeks post-treatment (see Table 16).
T16
- Overall SVR rates were similar among the three treatment groups. Regardless of treatment group, SVR rates were lower in subjects with poor prognostic factors. Subjects with poor prognostic factors randomized to PegIntron (1.5 mcg/kg)/REBETOL or Pegasys/Copegus, however, achieved higher SVR rates compared to similar subjects randomized to PegIntron 1 mcg/kg/REBETOL. For the PegIntron 1.5 mcg/kg plus REBETOL dose, SVR rates for subjects with and without the following prognostic factors were as follows: cirrhosis (10% vs. 42%), normal ALT levels (32% vs. 42%), baseline viral load greater than 600,000 IU/mL (35% vs. 61%), 40 years of age and older (38% vs. 50%), and African American race (23% vs. 44%). In subjects with undetectable HCV-RNA at Week 12 who received PegIntron (1.5 mcg/kg)/REBETOL, the SVR rate was 81% (328/407).
- PegIntron/REBETOL Combination Therapy in Prior Treatment Failures — Study 5
- In a noncomparative trial, 2293 subjects with moderate to severe fibrosis who failed previous treatment with combination alpha interferon/ribavirin were re-treated with PegIntron, 1.5 mcg/kg subcutaneously, once weekly, in combination with weight adjusted ribavirin. Eligible subjects included prior nonresponders (subjects who were HCV-RNA positive at the end of a minimum 12 weeks of treatment) and prior relapsers (subjects who were HCV-RNA negative at the end of a minimum 12 weeks of treatment and subsequently relapsed after post-treatment follow-up). Subjects who were negative at Week 12 were treated for 48 weeks and followed for 24 weeks post-treatment. Response to treatment was defined as undetectable HCV-RNA at 24 weeks post-treatment (measured using a research-based test, limit of detection 125 IU/mL). The overall response rate was 22% (497/2293) (99% CI: 19.5, 23.9). Subjects with the following characteristics were less likely to benefit from re-treatment: previous nonresponse, previous pegylated interferon treatment, significant bridging fibrosis or cirrhosis, and genotype 1 infection.
- The re-treatment sustained virologic response rates by baseline characteristics are summarized in Table 17.
T17
- Achievement of an undetectable HCV-RNA at treatment Week 12 was a strong predictor of SVR. In this trial, 1470 (64%) subjects did not achieve an undetectable HCV-RNA at treatment Week 12, and were offered enrollment into long-term treatment trials, due to an inadequate treatment response. Of the 823 (36%) subjects who were HCV-RNA undetectable at treatment Week 12, those infected with genotype 1 had an SVR of 48% (245/507), with a range of responses by fibrosis scores (F4-F2) of 39-55%. Subjects infected with genotype 2/3 who were HCV-RNA undetectable at treatment Week 12 had an overall SVR of 70% (196/281), with a range of responses by fibrosis scores (F4-F2) of 60-83%. For all genotypes, higher fibrosis scores were associated with a decreased likelihood of achieving SVR.
Chronic Hepatitis C in Pediatrics
- PegIntron/REBETOL Combination Therapy — Pediatric Trial
- Previously untreated pediatric subjects 3 to 17 years of age with compensated chronic hepatitis C and detectable HCV-RNA were treated with REBETOL 15 mg/kg/day plus PegIntron 60 mcg/m2 once weekly for 24 or 48 weeks based on HCV genotype and baseline viral load. All subjects were to be followed for 24 weeks post-treatment. A total of 107 subjects received treatment, of which 52% were female, 89% were Caucasian, and 67% were infected with HCV genotype 1. Subjects infected with genotype 1, 4 or genotype 3 with HCV-RNA greater than or equal to 600,000 IU/mL received 48 weeks of therapy while those infected with genotype 2 or genotype 3 with HCV-RNA less than 600,000 IU/mL received 24 weeks of therapy. The trial results are summarized in Table 18.
T18
How Supplied
T
- Storage
- PegIntron REDIPEN single-use pre-filled pen
- PegIntron REDIPEN pre-filled pen should be stored at 2-8°C (36-46°F).
- After reconstitution, the solution should be used immediately, but may be stored up to 24 hours at 2-8°C (36-46°F). The reconstituted solution contains no preservative, and is clear and colorless. DO NOT FREEZE. Keep away from heat.
- PegIntron Vials
- PegIntron should be stored at 25°C (77°F); excursions permitted to 15-30°C (59-86°F). After reconstitution with supplied diluent, the solution should be used immediately but may be stored up to 24 hours at 2-8°C (36-46°F). The reconstituted solution contains no preservative, and is clear and colorless. DO NOT FREEZE. Keep away from heat.
- Disposal Instructions
- Patients should be thoroughly instructed in the importance of proper disposal. After preparation and administration of PegIntron for Injection, patients should be advised to use a puncture-resistant container for the disposal of used syringes, needles, and the REDIPEN pre-filled pen. The full container should be disposed of in accordance with state and local laws. Patients should also be cautioned against reusing or sharing needles, syringes, or the REDIPEN pre-filled pen.
Storage
There is limited information regarding Pegylated interferon alfa-2b Storage in the drug label.
Images
Drug Images
{{#ask: Page Name::Pegylated interferon alfa-2b |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Pegylated interferon alfa-2b |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
- A patient should self-inject PegIntron only if it has been determined that it is appropriate, the patient agrees to medical follow-up as necessary, and training in proper injection technique has been given to him/her.
- Pregnancy
- Patients must be informed that REBETOL (ribavirin) may cause birth defects and death of the unborn child. Extreme care must be taken to avoid pregnancy in female patients and in female partners of male patients during treatment with combination PegIntron/ribavirin therapy and for 6 months post-therapy. Combination PegIntron/ribavirin therapy should not be initiated until a report of a negative pregnancy test has been obtained immediately prior to initiation of therapy. It is recommended that patients undergo monthly pregnancy tests during therapy and for 6 months post-therapy.
- HCV Transmission
- Inform patients that there are no data regarding whether PegIntron therapy will prevent transmission of HCV infection to others. Also, it is not known if treatment with PegIntron will cure hepatitis C or prevent cirrhosis, liver failure, or liver cancer that may be the result of infection with the hepatitis C virus.
- Laboratory Evaluations, Hydration, "Flu-like" Symptoms
- Patients should be advised that laboratory evaluations are required before starting therapy and periodically thereafter. It is advised that patients be well hydrated, especially during the initial stages of treatment. "Flu-like" symptoms associated with administration of PegIntron may be minimized by bedtime administration of PegIntron or by use of antipyretics.
- Patients developing fever, cough, shortness of breath or other symptoms of a lung problem during treatment with PegIntron may need to have a chest X-ray or other tests to adequately treat them.
- Instructions for Use
- Patients receiving PegIntron should be directed in its appropriate preparation, handling, measurement, and injection, and referred to the Instructions for Use for PegIntron Powder for Solution and PegIntron REDIPEN Single-use Pre-filled pen.
- Patients should be directed to store PegIntron before mixing as follows:
- PegIntron REDIPEN single-use pre-filled pens: store in the refrigerator between 36-46°F (2-8°C)
- PegIntron Powder for Solution: store at room temperature between 59-86°F (15-30°C)
- Patients should be instructed on the importance of site selection for self-administering the injection, as well as the importance on rotating the injection sites.
Precautions with Alcohol
- Alcohol-Pegylated interferon alfa-2b interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- PEGINTRON®[2]
Look-Alike Drug Names
- A® — B®[3]
Drug Shortage Status
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
- ↑ http://www.fda.gov/downloads/Drugs/DrugSafety/UCM133677.pdf See line 27
- ↑ "PEGINTRON peginterferon alfa-2b kit".
- ↑ "http://www.ismp.org". External link in
|title=(help)
{{#subobject:
|Page Name=Pegylated interferon alfa-2b |Pill Name=No image.jpg |Drug Name= |Pill Ingred=|+sep=; |Pill Imprint= |Pill Dosage= |Pill Color=|+sep=; |Pill Shape= |Pill Size (mm)= |Pill Scoring= |Pill Image= |Drug Author= |NDC=
}}
{{#subobject:
|Label Page=Pegylated interferon alfa-2b |Label Name=Pegylated interferon alfa-2b11.png
}}
{{#subobject:
|Label Page=Pegylated interferon alfa-2b |Label Name=Pegylated interferon alfa-2b11.png
}}