How to read an ECG
| How to Read an ECG |
|---|
| Overview |
| Rhythm |
| Rate |
| Conduction |
| Axis |
| P Wave Morphology |
| QRS Morphology |
| ST Morphology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby
Overview
- The interpretation of an ECG should be done in a consistent step-by-step way. Each ECG should be evaluated for the following:
- Rhythm
- Rate
- Conduction
- Axis
- P wave morphology
- QRS morphology
- ST morphology
- Compare the current ECG to previous ECG
Rhythm
- The sinus node (SA), located in the roof of the right atrium, is the fastest physiological pacemaker. When the sinus node generates an electrical impulse, the surrounding cells of the right atrium depolarize. Then the depolarization wave spreads to the cells of the left atrium, the AV node, the bundle of His and then to the ventricles through the purkinje fibers.
- Criteria for normal sinus rhythm (see also Basics)
- A P wave (atrial contraction) precedes every QRS complex
- The P wave is positive in I and II, and biphasic in V1
- The P waves maximum height is 2.5 mm in II and/or III
- The rhythm is regular, but varies slightly while breathing
- The frequency ranges between 60 and 100 beats per minute
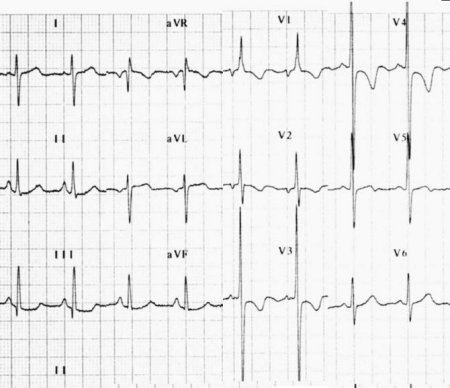
- Below is an ECG showing normal sinus rhythm.
-
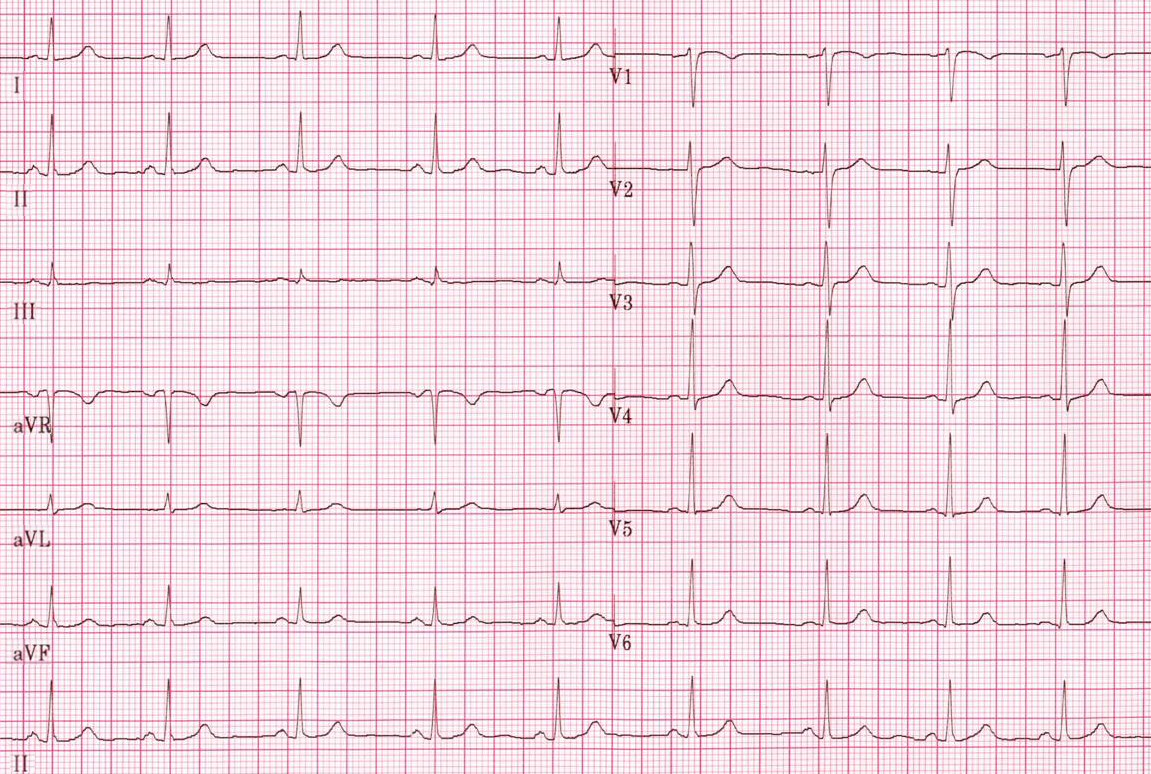 Normal sinus rhythm.
Normal sinus rhythm.

- Characteristics of a normal P wave
- The maximal height of the P wave is 2.5 mm in leads II and/or III
- The P wave is positive in II and aVF, and biphasic in V1
- The P wave duration is usually shorter than 0.12 seconds
- The regularity of the waves
- The distance between two R waves, called RR interval, is constant in a regular rhythm
Abnormalities in the rhythm:
- P wave is absent in atrial fibrillation, junctional or ventricular rhythm.
- Variable morphologies of P waves in a single ECG lead is suggestive of an ectopic pacemaker rhythm such as wandering pacemaker or multifocal atrial tachycardia.
- When the RR interval is not constant, the rhythm is said irregular. When the rhythm is irregularly irregular it is a sign of the presence of atrial fibrillation.
Rate
- The normal heart rate is between 60 and 100 beats per minutes.
- It is important to remember the temporal significance of the small and large squares on an ECG strip. See the picture below for a detailed explanation:
- Below is an image showing the significance of small and large squares in an ECG paper.

- Determining the heart rate can be done using one of these three methods:
- First method: Counting the squares
- Use the sequence 300-150-100-75-60-50-43-37. Count from the first QRS complex, the first thick line is 300, the next thick line 150 etc. Stop the sequence at the next QRS complex. When the second QRS complex is between two lines, take the mean of the two numbers from the sequence
- Below is an image showing the squares counting method used to calculate the heart rate.

- Second method:
- The ECG paper runs at 25 mm/sec through the ECG printer; therefore heart rate can be calculate using the following formula:
![]()
- Third method:
- Count the number of QRS complexes that fit into 3 seconds (some ECG writers print this period on the ECG paper). Multiply this number by 20 to find the number of beats/minute.
Abnormalities in the rate:
- A heart rate less than 60 is called bradycardia.
- A heart rate larger than 100 is called tachycardia.
Conduction
The evaluation of the conduction requires the evaluation of the PR interval, QRS duration and QT interval.
1- PR Interval
- The PR interval is measured from the beginning of the P wave to the beginning of the QRS complex.
- The PR interval reflects the time the electrical impulse takes to travel from the sinus node through the AV node where it enters the ventricles. The PR interval is therefore a good estimate of AV node function.
- The PR interval is normally between 120 to 200 ms long (3 to 5 small boxes).
Abnormalities in the PR interval:
- A long PR interval (of over 200 ms) may indicate a first-degree heart block or electrolyte disturbances (for example hypokalemia)
- A variable PR interval may indicate other types of heart block.
- Mobitz 1
- Mobitz 2
- Third degree heart block
- A short PR interval may indicate a pre-excitation syndrome via an accessory pathway that leads to early activation of the ventricles, such as seen in Wolf Parkinson White syndrome
2- The Duration of QRS
- The QRS duration indicates how fast the ventricles depolarize.
- The normal QRS is < 0.10 seconds
Abnormalities in the duration of QRS:
- When the QRS duration is longer than 110 miliseconds, a conduction delay is present.
- For the diagnosis of LBBB or RBBB QRS duration must be >120 ms.
Causes of abnormal duration of QRS:
In alphabetical order
- Electrolyte disorders
- Idioventricular rhythm
- Left bundle branch block
- Paced ryhthm
- Right bundle branch block
3- The QT Interval
- The QT interval indicates how fast the ventricles are repolarized, becoming ready for a new cycle.
- The QT interval comprises the QRS-complex, the ST-segment, and the T-wave. One difficultly of QT interpretation is that the QT interval gets shorter as the heart rate increases. This problem can be solved by correcting the QT time for heart rate.
- Calculation of QTc using the tangent method:
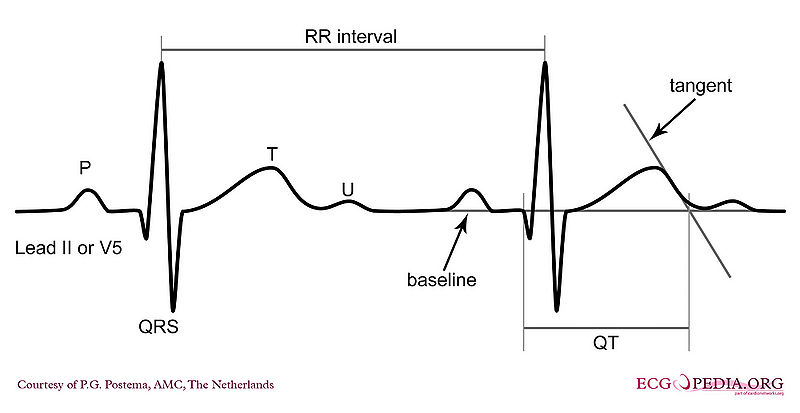
- Use lead II. Use lead V5 alternatively if lead II cannot be read.
- Draw a line through the baseline (preferably the PR segment)
- Draw a tangent against the steepest part of the end of the T wave. If the T wave has two positive deflections, the taller deflection should be chosen. If the T wave is biphasic, the end of the taller deflection should be chosen.
- The QT interval starts at the beginning of the QRS interval and ends where the tangent and baseline cross.
- Calculation of QTc using Bazett’s equation:
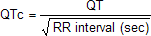
- Calculation of QTc using the tangent method:
- The normal value for QTc (corrected QT interval) is: below 450 ms for men and below 460 ms for women.

Abnormalities in the QT interval:
- QTc can be prolonged.
- If QTc is < 340 ms short QT syndrome can be considered.
Axis
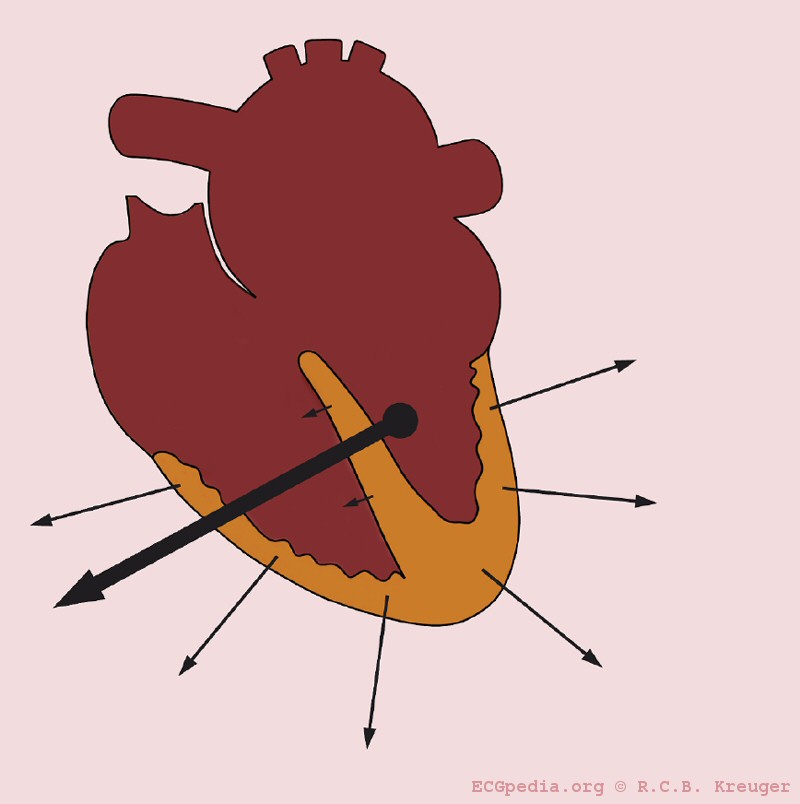
- The cardiac axis is an imaginary vector corresponding to the average of the different depolarization vectors in the heart. The depolarization wave begins in the right atrium and spread to the left and right ventricle. Because the left ventricle wall muscle mass is larger than the right wall muscle mass, the arrow representing the direction of the depolarization wave is directed towards the left.
- The normal depolarization vector is directed towards leads I, II and III. Hence, the deflections in these leads are positive in such a way that the deflection in lead II is more positive than that in leads I and III.
- The shapes of the QRS complex in leads I, II ad III are used to estimate the cardiac axis.
- Keep in mind that:
- When the depolarization is directed towards the lead, the ECG recording in that lead will show positive deflection.
- When the depolarization is directed away from the lead, the ECG recording in that lead will show negative deflection.
- A positive deflection is defined as the QRS having a larger 'area under the curve' above the baseline than below the baseline
QRS Axis
- The normal cardiac axis lies between -30 and +90 degrees.

- Below is an image showing the different angles of the heart with correspondence to the leads.

- A normal cardiac axis along with the different wave forms in leads I, II and III are represented in the image below:
- Below is two image showing the normal axis of the heart and right axis deviation respectively.


Abnormalities in the cardiac axis:
- A right heart axis(between +90 and +180) is present when lead I is negative and III positive.
- If right axis deviation is present the axis will be tilted towards the right. Hence, the axis will be going away from lead I and thus R will be smaller than S in lead I and the axis will be going more towards lead III and thus R will be larger than S in lead III.
- A left heart axis(between -30 and -90 degrees) is present when the QRS in lead I is positive and negative in II and III.
- When the depolarization is perpendicular on the lead, this is called iso-electric. The QRS is neither positive nor negative.
- If R is equal to S in lead II, then it is expected that the cardiac axis lies at a right angle from lead II. Hence, the cardiac axis would be either at an angle of -30 degrees or +150 degrees. The shape of the QRS complex, whether positively or negatively deflected, helps in determining the direction of the cardiac axis.
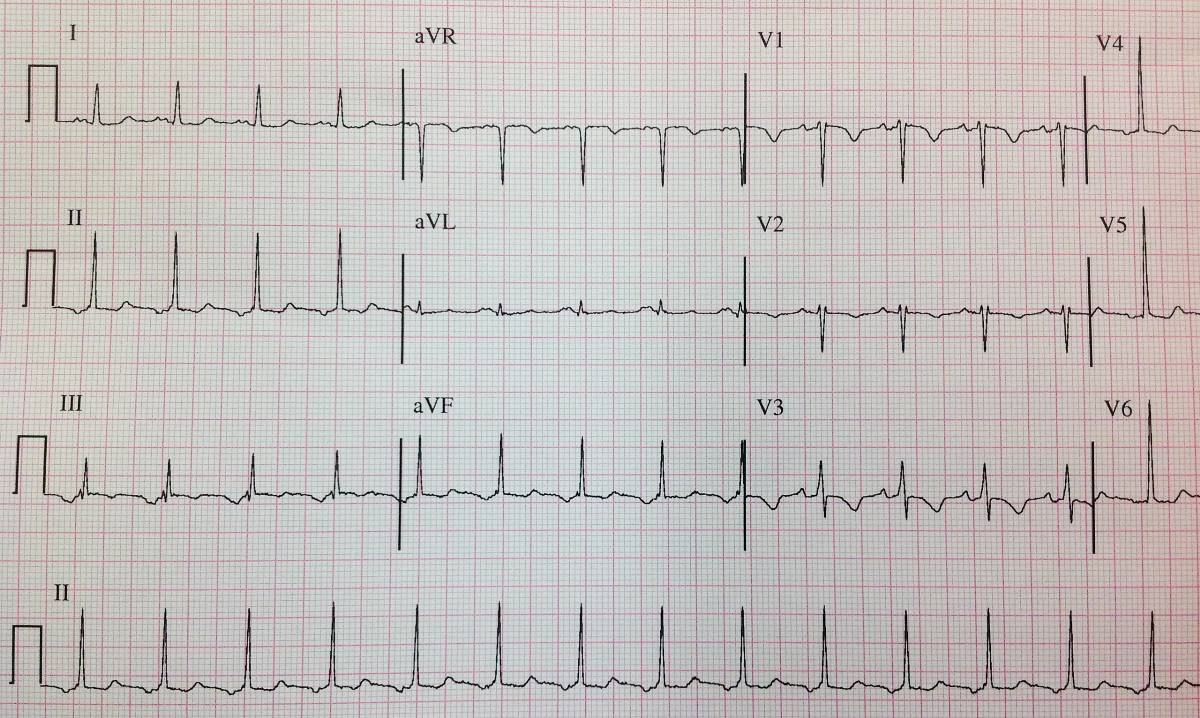
- Below ECGs showing left heart axis deviation and right heart axis deviation respectively.
-
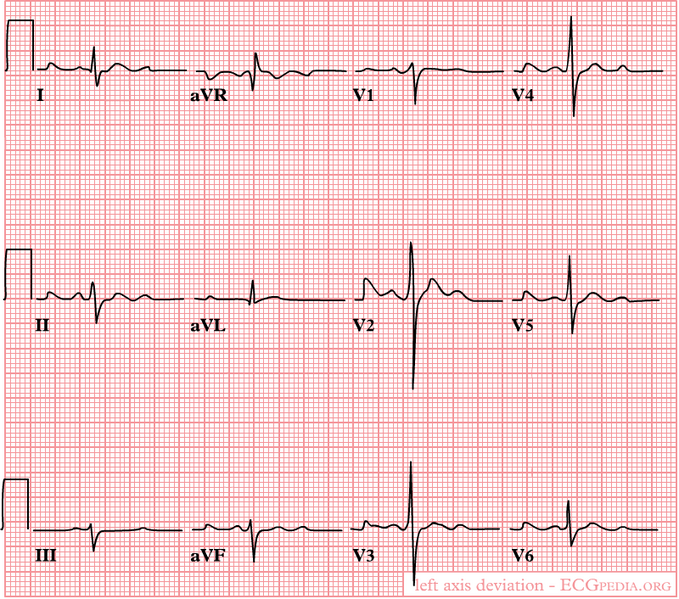 A left heart axis is present when the QRS in lead I is positive and negative in II and III.
A left heart axis is present when the QRS in lead I is positive and negative in II and III. -
 A right heart axis is present when lead I is negative and III positive.
A right heart axis is present when lead I is negative and III positive.


Causes of Axis Deviation:
- 1- Actual rotation of the heart: When the heart itself is rotated (right ventricular overload), obviously the axis turns with it.
- The picture below illustrates heart axis deviation to the right in right ventricular load, as in COPD or pulmonary embolism. A right axis is between +90 and +180 degrees. In this case the axis is +135 degrees
-
 Right axis deviation
Right axis deviation

- 2- Ventricular hypertrophy: The axis will deviate towards the greater electrical activity and the vector will turn towards the hypertrophied tissue.
- 3- Infarcted tissue: An infarcted tissue is electrically dead and thus no electrical activity is registered and the QRS vector turns away from the infarcted tissue
- The picture below illustrates heart axis deviation to the left in case of an inferior infarct. Left anterior hemiblock is a common cause. A left axis is between -30 and -90 degrees. The axis is -30 degrees.
-
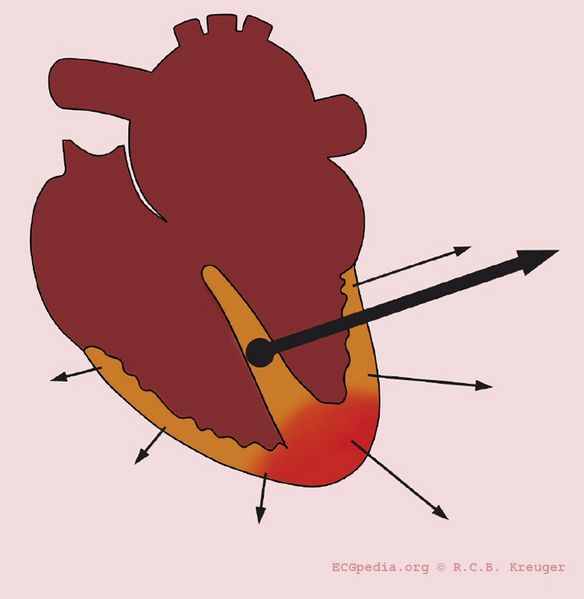 Left axis deviation in the case of an inferior infarct
Left axis deviation in the case of an inferior infarct

- 4- Conduction problems: When RBBB is present the right ventricle depolarizes later than the left ventricle. In a normal situation the vector is influenced by the left ventricle, but in RBBB only the right ventricle determines it.
P Wave Morphology
Evaluation of the P wave
The P wave represents atrial depolarization (stimulation). At rapid rates, the P wave may merge with the preceding T wave and become difficult to identify.
The evaluation of the P wave should include the following:
1. Examination of the P wave contour
- The P wave contour is normally smooth, and is either entirely positive or entirely negative wave (monophasic wave) in all leads except V1.

2. Measurement of the P wave duration
- The P wave duration is normally less than 0.12 seconds
3. Measurement of the maximal P wave amplitude
- The maximal P-wave amplitude is normally no more than 0.2 mV in the frontal plane leads and no more than 0.1 mV in the transverse plane leads.
4. Estimation of the P wave axis
- The P wave normally appears entirely upright on leftward and inferiorly oriented leads such as I, II, aVF, and V4 to V6
- It is negative in aVR because of the rightward orientation of that lead, and it is variable in the other standard leads.
5. Consistency of the P wave shape.
6. The relationship between the P wave and the QRS wave.
7. Morphology of the PTa segment
Abnormalities of the P wave:
- Widened P waves can be a sign of Class Ia antiarrhythmic drugs intoxication (quinidine, etc.) and small or absent P waves can be a sign of hyperkalemia.
- If the p-wave is enlarged, the atria are enlarged.
Inverted P wave
- P waves can be inverted in I and aVL, the differential causes include dextrocardia and reversed arm lead.
- Below is an image showing inverted P waves corresponding to dextrocardia and reversed arm lead.

- P waves can be inverted in the inferior leads in the setting of a low atrial focus as the origin of the rhythm.
- Below is an ECG showing inverted P waves in the inferior leads.
-
 Inverted P waves in inferior leads
Inverted P waves in inferior leads

Abnormal PTa Segment
- Elevation or depression of the PTa segment (the part between the p wave and the beginning of the QRS complex) can result from atrial infarction or pericarditis.
- Below is an image showing abnormal PTa segments.

QRS Morphology
The Basic Questions in the Evaluation of QRS Morphology
- Are there any pathological Q waves as a sign of previous myocardial infarction?
- Are there signs of left or right ventricular hypertrophy?
- Does the QRS complex show microvoltage (roughly QRS < 5mm)?
- Is the conduction normal or prolonged (QRS-interval > 0,12s)?
Q Wave
- If the first deflection of the QRS is downward it is called Q wave.
- The Q wave represents activation of the ventricular septum as the electricity spreads from the left to the right through the septum.
- Pathologic Q waves are a sign of previous myocardial infarction.
- They are the result of absence of electrical activity because a scar tissue is electrically dead.
- Pathologic Q waves are not an early sign of myocardial infarction, but generally take several hours to days to develop.
- Once pathologic Q waves have developed they rarely go away. However, if the myocardial infarction is reperfused early (e.g. as a result of percutaneous coronary intervention) stunned myocardial tissue can recover and pathologic Q waves disappear. In all other situations they usually persist indefinitely.
- Lead III often shows Q waves, which are not pathologic as long as Q waves are absent in leads II and aVF
- Absence of pathologic Q waves does not exclude a myocardial infarction!
- Definition of a pathologic Q wave:
- Any Q-wave in leads V2–V3 ≥ 0.02 s or QS complex in leads V2 and V3
- Q-wave ≥ 0.03 s and > 0.1 mV deep or QS complex in leads I, II, aVL, aVF, or V4–V6 in any two leads of a contiguous lead grouping (I, aVL,V6; V4–V6; II, III, and aVF)
- R-wave ≥ 0.04 s in V1–V2 and R/S ≥ 1 with a concordant positive T-wave in the absence of a conduction defect
-
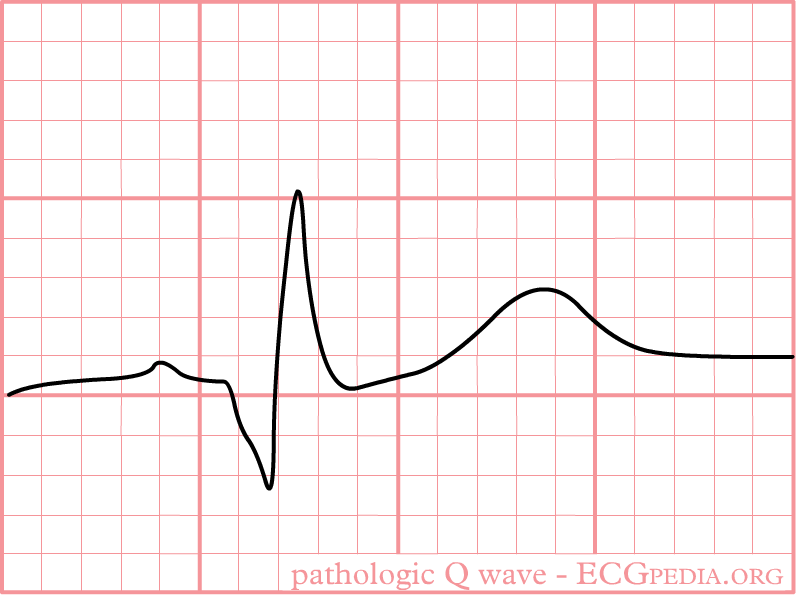 Pathologic Q wave
Pathologic Q wave

R Wave
- The first upward deflection of the QRS is called the R wave.
- Most of the ventricle is activated during the R wave.
- The septal depolarization corresponds to an initial positive deflection (R wave) in V1 and V2 and negative deflection (Q wave) in V3 and V4.
- Because the left ventricular mass is larger than that of the right ventricle, the vector corresponding to the ventricular mass depolarization is directed towards the left. Thus, the ventricular depolarization corresponds to a negative deflection (S wave) in V1 and V2 and a positive deflection (R wave) in V3 and V4.
- The progression of V1 to V6 is important to notice: The QRS complex is predominantly deflected downwards in V1 and gradually becomes positively deflected to show a predominantly upwards deflection in V6
- The transition zone is where the QRS complex changes from predominately negative to predominately positive (R/S ratio becoming >1).
- The transition zone usually occurs at V3 or V4.
- It is normal to have the transition zone at V2 (called "early transition"), and at V5 (called "delayed transition").
Abnormalities in R wave:
- Poor R wave progression (PRWP):
- Prolonged R wave:
- The R wave may be prolonged if the ventricle is enlarged.
- Enlarged R wave:
- The R wave may be abnormally high (indicating strong voltage) if the ventricular muscle tissue is hypertrophied
- Below are images showing normal and poor R wave progression.


ST Morphology
- The ST segment is normally at or near the baseline.
Abnormalities in the ST segment
1-ST Elevation:
- The most important cause of ST segment elevation is acute ischemia.
- An important clue for the diagnosis of ischemia is the presence of reciprocal ST segment depression.
- Below is an ECG showing abnormal ST elevation.

Early Repolarization
- Early repolarization is a term used for ST segment elevation without underlying disease. It probably has nothing to do with actual early repolarization.
- It is commonly seen in young men.
- It is important to discern early repolarization from ST segment elevation from other causes such as ischemia.
- Characteristics of early repolarization are[1]:
- An upward concave elevation of the RS-T segment with distinct or "embryonic" J waves
- Slurred downstroke of R waves or distinct J points or both
- RS-T segment elevation commonly encountered in the precordial leads and more distinct in these leads
- Rapid QRS transition in the precordial leads with counterclockwise rotation
- Persistence of these characteristics for many years
- Absence of reciprocal ST depression
- Large symmetrical T waves
- Below is an image showing ST elevation due to repolarization.

- Below is an ECG showing normal and early repolarization ST elevation.

2- ST depression:
- The most important cause of ST segment depression is Ischemia.
- Reciprocal ST segment depression. If one lead shows ST segment elevation then usually the lead 'on the other side' shows ST segment depression.
3- T wave changes:
- The T wave is a non specific indicator of the presence of a cardiac abnormality.
- T waves can be peaked, normal, flat, or inverted (negative).
- Flat T wave: < 0.5 mm negative or positive T wave in leads I, II, V3, V4, V5 or V6
- Negative (or inverted) T wave: > 0.5 mm negative T wave in leads I, II, V3, V4, V5 or V6
- Below is an image showing the different T wave morphologies.

Causes of ST elevation:[2]:
In alphabetical order
- Early repolarization
- Acute pericarditis: ST elevation in all leads except aVR
- Acute sympathic stress: all leads, especially V1-V6
- Acute neurologic events: all leads, primarily V1-V6
- Brugada syndrome
- Cardiac aneurysm
- Cardiac contusion
- Hyperkalemia: V1-V2 (V3)
- Hypertrophic cardiomyopathy: V3-V5 (sometimes V6)
- Hypothermia: ST elevation in V3-V6, II, III and aVF
- Idioventricular rhythm including paced rhythm
- Ischemia
- Left ventricular hypertrophy
- Pulmonary embolism: ST elevation in V1 and aVR
Causes of ST segment depression:
In alphabetical order
- Digoxin
- Electrolyte disturbances (low potassium, low magnesium)
- Heart rate-induced changes (post tachycardia)
- Ischemia
- Left ventricular hypertophy with "strain" or depolarization abnormality
- Neurologic events
Causes of T wave changes:
In alphabetical order
- Cardiac contusion
- Digoxin
- Ischemia
- Mitral valve prolapse
- Myocardial infarction
- Myocarditis
- Pericarditis
- Subarachnoid hemorrhage
- Ventricular hypertrophy with strain
References
- ↑ Kambara H, Phillips J (1976). "Long-term evaluation of early repolarization syndrome (normal variant RS-T segment elevation)". Am J Cardiol. 38 (2): 157–6. PMID 133604.
- ↑ Wang K, Asinger RW, Marriott HJ (2003). "ST-segment elevation in conditions other than acute myocardial infarction". N Engl J Med. 349 (22): 2128–35. doi:10.1056/NEJMra022580. PMID 14645641.