Pleomorphic adenoma: Difference between revisions
Tarek Nafee (talk | contribs) |
Tarek Nafee (talk | contribs) |
||
| Line 58: | Line 58: | ||
==Epidemiology and Demographics== | ==Epidemiology and Demographics== | ||
===Epidemiology=== | |||
*Pleomorphic adenoma accounts for 60% of all parotid gland tumors and represents 45-75% of all salivary gland neoplasms. | *Pleomorphic adenoma accounts for 60% of all parotid gland tumors and represents 45-75% of all salivary gland neoplasms. | ||
*The [[incidence]] of pleomorphic adenoma is approximately 2-3.5 per 100,000 individuals worldwide. | *The [[incidence]] of pleomorphic adenoma is approximately 2-3.5 per 100,000 individuals worldwide. | ||
Revision as of 18:25, 24 August 2016
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Maria Fernanda Villarreal, M.D. [2]; Tarek Nafee, M.D. [3]
Synonyms and keywords: Pleomorphic adenoma of the salivary glands; BMT; Benign mixed tumors of the salivary gland
Overview
Pleomorphic adenoma (also known as "Benign mixed tumor of the salivary gland") is a benign neoplastic tumor of the salivary glands. Pleomorphic adenoma is the most common type of salivary gland tumor and the most common tumor of the parotid gland.[1] Pleomorphic adenoma was first described by Beahrs in 1957.[2] Pleomorphic adenoma may be classified according to anatomical distribution into 4 groups: parotid gland pleomorphic adenoma, submandibular gland pleomorphic adenoma, minor salivary gland pleomorphic adenoma, and sublingual gland pleomorphic adenoma. The pathogenesis of pleomorphic adenoma is characterized by an admixture of polygonal epithelial and spindle-shaped myoepithelial elements. A mutation on the PLAG1 gene is associated with the development of pleomorphic adenoma. Pleomorphic adenoma is common and it accounts for 60% of all parotid gland tumors (represents 45-75% of all salivary gland neoplasms). The incidence of pleomorphic adenoma is approximately 2-3.5 per 100,000 individuals worldwide. The most characteristic clinical feature of pleomorphic adenoma is a painless single-nodular parotid mass. Pleomorphic adenoma may be initially asymptomatic. Common symptoms of pleomorphic adenoma may include xerostomia, dysphagia, and painful chewing. MRI is the imaging modality of choice for pleomorphic adenoma. Surgical excision in conjunction with pre-surgical biopsy is the most common approach to the management of pleomorphic adenoma. The recurrence rate after surgery will depend on the histological subtype (mixed pleomorphic adenomas have a higher recurrence rate). In some cases, patients with pleomorphic adenoma may receive medications to stimulate saliva production such as pilocarpin and cevimeline for symptomatic relief.
Historical Perspective
Pleomorphic adenoma was first described by Beahrs in 1957.[2][3]
Classification
Pleomorphic adenoma may be classified according to anatomical distribution into 4 groups:[4]
- Parotid gland pleomorphic adenoma (80%)
- Superficial lobe pleomorphic adenoma (most common)
- Submandibular gland pleomorphic adenoma
- Minor salivary gland pleomorphic adenoma
- Sublingual gland pleomorphic adenoma
Pleomorphic adenoma may also be classified according to histological type into 3 subtypes:[4]
- Mixed (hypocellular)
- Cellular
- Classic
Lacrimal gland pleomorphic adenoma is a variant of pleomorphic adenoma which accounts for approximately 50% of lacrimal gland tumors.[4]
Pathophysiology
Pathogenesis
The pathogenesis of pleomorphic adenoma is characterized by an admixture of polygonal epithelial and spindle-shaped myoepithelial elements.[4]
Genetics
The mutation on PLAG1 gene has been associated with the development of pleomorphic adenoma.[4]
Gross Pathology
On gross pathology, characteristic findings of pleomorphic adenoma include:[4]
- May have cartilaginous appearance
- Typically well-circumscribed
- Tumor is usually enveloped by a fibrous capsule
Microscopic Pathology
On microscopic histopathological analysis, characteristic findings of pleomorphic adenoma include:[4]
- Mixture of epithelial and myoepithelial elements
- Background stroma that may be mucoid, mixed, cartilaginous, or hyaline
- Epithelial elements may be arranged in duct-like structures, sheets, clumps and/or interlacing strands
- Epithelial elements consist of polygonal, spindle or stellate-shaped cells (hence pleomorphism)
On immunohistochemical analysis, characteristic findings of pleomorphic adenoma include:[4]
- Positive S-100 protein
- Positive SMA
- Positive GFAP
Causes
There are no established causes for pleomorphic adenoma.
Differentiating Pleomorphic Adenoma from Other Diseases
Pleomorphic adenoma must be differentiated from other diseases that cause xerostomia, single-nodular parotid mass, and dysphagia such as:
- Warthin's tumor
- Mucoepidermoid carcinoma
- Myoepithelioma
- Adenoid cystic carcinoma
Epidemiology and Demographics
Epidemiology
- Pleomorphic adenoma accounts for 60% of all parotid gland tumors and represents 45-75% of all salivary gland neoplasms.
- The incidence of pleomorphic adenoma is approximately 2-3.5 per 100,000 individuals worldwide.
Age
- Pleomorphic adenoma is more commonly observed among patients aged 60 to 70 years old.
- Pleomorphic adenoma is less commonly observed in children.
Gender
- Pleomorphic adenoma affects men and women equally.
Race
- There is no racial predilection for pleomorphic adenoma.
Risk Factors
Common risk factors in the development of pleomorphic adenoma include:[5]
- Ionizing radiation
- Occupations associated with an increased risk such as:
- Rubber products manufacturing
- Asbestos mining
- Plumbing
- Some types of woodworking
Natural History, Complications and Prognosis
- The majority of patients with pleomorphic adenoma remain asymptomatic for years.
- Early clinical features include dry mouth, difficulty swallowing, and a palpable single nodular mass.
- If left untreated, patients with pleomorphic adenoma may progress to develop malignant transformation.
- Common complications of pleomorphic adenoma include:[4]
- Nerve injury
- Cosmetic deformity
- Hemorrhage or hematoma
- Frey's syndrome
- If there is a malignant transformation, prognosis is generally poor. The 5-year survival rate of patients with malignant pleomorphic adenoma is approximately 30%.[4]
Diagnosis
Symptoms
- Pleomorphic adenoma may be initially asymptomatic.
- Symptoms of pleomorphic adenoma may include the following:[4]
Physical Examination
- Patients with pleomorphic adenoma may present with a facial deformity.
- Physical examination of the head and neck may be remarkable for:[6]
- Submandibular single, mobile, painless, and firm nodular mass
- Eversion of the ear lobe
- Limited mandiblular motion
Laboratory Findings
- There are no specific laboratory findings associated with pleomorphic adenoma.[4]
Imaging Findings
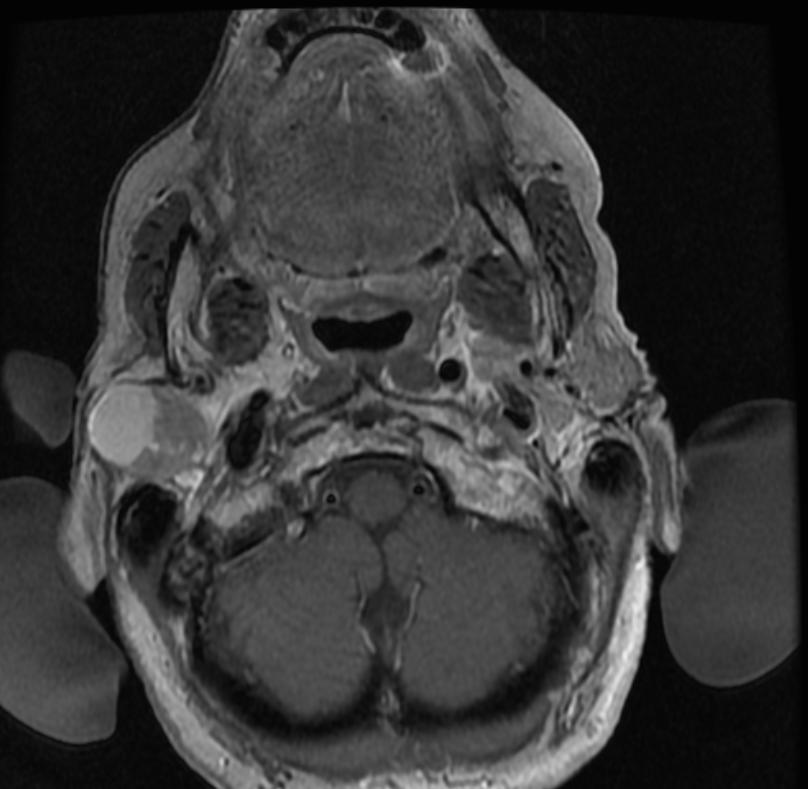
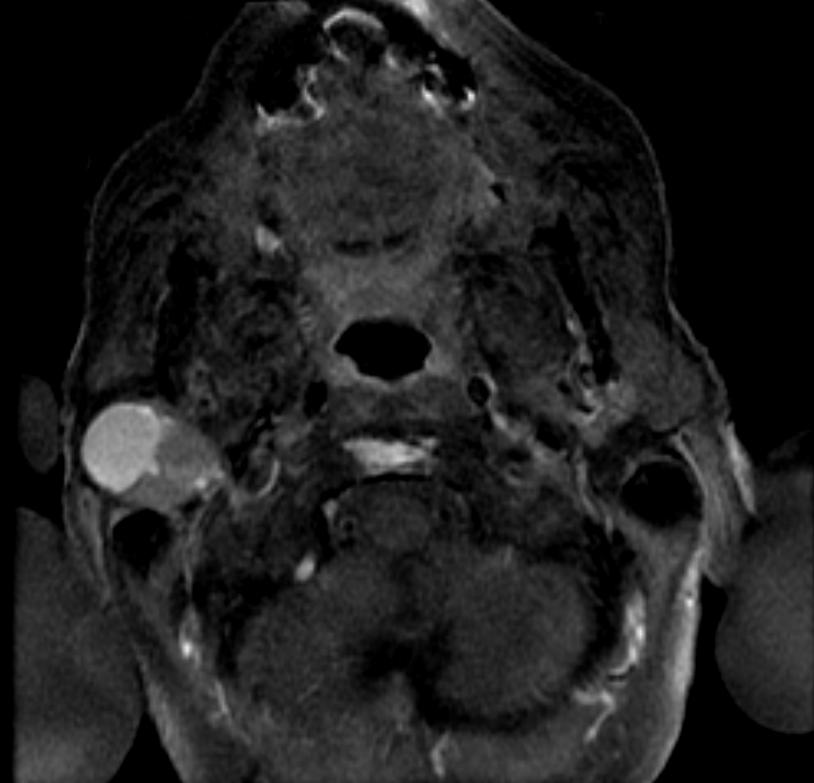
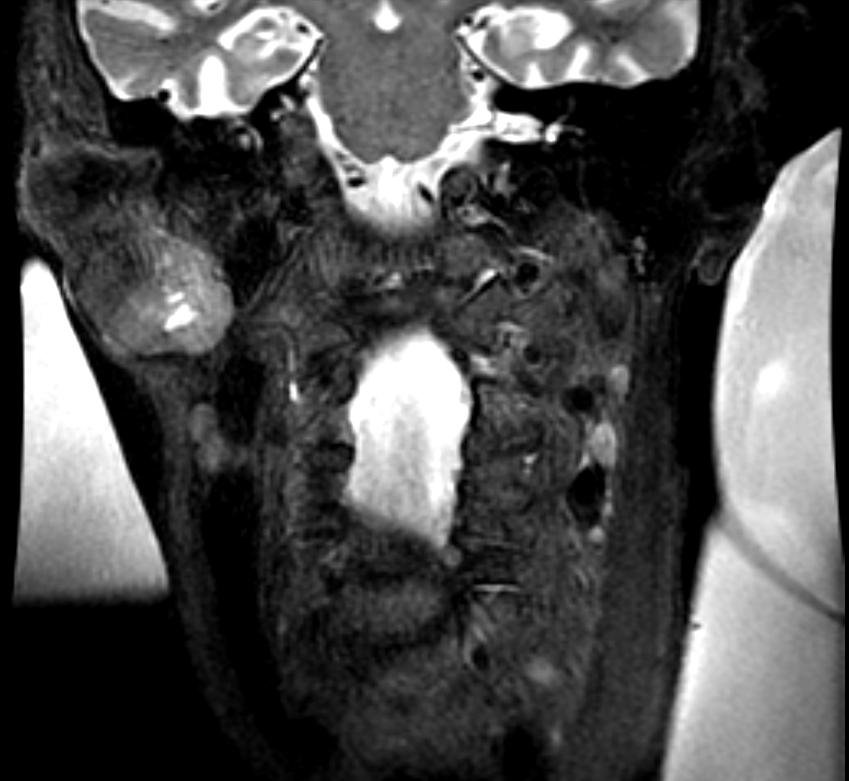
- MRI is the imaging modality of choice for pleomorphic adenoma. On MRI, characteristic findings of pleomorphic adenoma, include:[6][6]
- Pleomorphic adenomas are usually well-circumscribed
- Homogeneous masses with low intensity on T1-weighted images and high intensity on T2-weighted images
- Commonly, a rim of decreased signal intensity on T2-weighted images is observed
- After gadolinium enhancement, the tumors are homogeneously enhancing unless they are large.
- On CT scan, characteristic findings of pleomorphic adenoma include:
- Smooth and well-marginated tumors
- The attenuation values of the mass are usually homogeneous and higher than that of the surrounding gland
- Tumor enhancement is variable and can result in a missed diagnosis if delayed images are not acquired
- Pleomorphic adenomas are poorly enhancing in the early phase of contrast enhancement, though the amount of enhancement increases over time
- On Ultrasound, characteristic findings of pleomorphic adenomas include:
Gallery
-
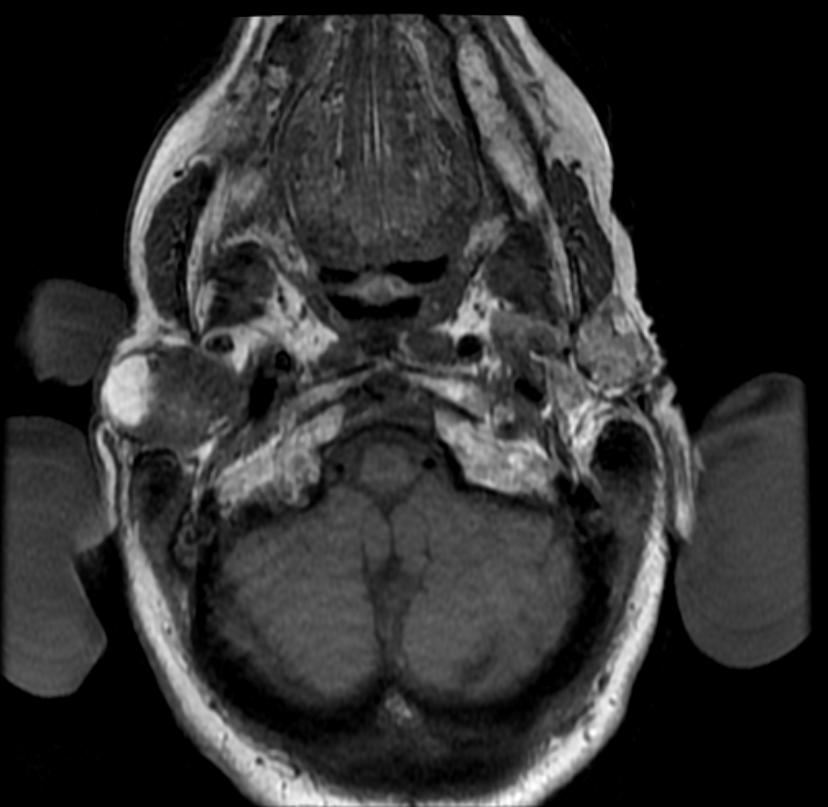
MRI: A right parotid pleomorphic adenoma Images courtesy of RadsWiki
-

MRI: A right parotid pleomorphic adenoma Images courtesy of RadsWiki
-
MRI: A right parotid pleomorphic adenoma Images courtesy of RadsWiki
-
MRI: A right parotid pleomorphic adenoma Images courtesy of RadsWiki
-
MRI: A right parotid pleomorphic adenoma Images courtesy of RadsWiki
-
PET: A right parotid pleomorphic adenoma Images courtesy of RadsWiki






Other Diagnostic Studies
- Pleomorphic adenoma may also be diagnosed using fine needle aspiration (FNA) and core needle biopsy.
- FNA can determine whether the tumor is malignant in nature with a sensitivity approximately 90%[8][9]
- FNA can also distinguish primary salivary tumor from metastatic disease
- Core needle biopsy is more accurate compared to FNA with diagnostic accuracy greater than 97%[10]
- Findings on fine needle aspiration (FNA) and core needle biopsy, include:
- Admixture of polygonal epithelial and spindle-shaped myoepithelial elements
- Mesenchymal stroma (important feature)
- Proliferation of myoepithelium and epithelium
Treatment
Medical Therapy
- There is no treatment for pleomorphic adenoma; the mainstay of therapy is surgery.
- In some cases, patients with pleomorphic adenoma can receive medications to stimulate saliva production, such as:
Surgery
- Surgery is the mainstay of therapy for pleomorphic adenoma.
- Surgical excision in conjunction with pre-surgical biopsy is the most common approach to the treatment of pleomorphic adenoma.
- The recurrence rate after surgery will depend on the histological subtype.
- Mixed pleomorphic adenomas have a higher recurrence rate.
Prevention
- There are no primary preventive measures available for pleomorphic adenoma.
- Once diagnosed and successfully treated, patients with pleomorphic adenoma are followed-up every 6 or 12 months.
References
- ↑ Ewa J. Bialek, Wieslaw Jakubowski, Piotr Zajkowski, Kazimierz T. Szopinski, and Antoni Osmolski. US of the Major Salivary Glands: Anatomy and Spatial Relationships, Pathologic Conditions, and Pitfalls. RadioGraphics 2006 26: 745-763.
- ↑ 2.0 2.1 Keerthi R, Raut RP, Vaibhav N, Ghosh A (2014). "Carcinoma ex pleomorphic adenoma: Diagnostic dilemma and treatment protocol". Indian J Dent. 5 (3): 157–60. doi:10.4103/0975-962X.140840. PMC 4213878. PMID 25565746.
- ↑ BEAHRS OH, WOOLNER LB, KIRKLIN JW, DEVINE KD (1957). "Carcinomatous transformation of mixed tumors of the parotid gland". AMA Arch Surg. 75 (4): 605–13, discussion 613-4. PMID 13457639.
- ↑ 4.00 4.01 4.02 4.03 4.04 4.05 4.06 4.07 4.08 4.09 4.10 4.11 Pleomorphic adenoma. Wikipedia. https://en.wikipedia.org/wiki/Pleomorphic_adenoma. Accessed on April 25, 2016
- ↑ Pleomorphic adenoma. Salivary Gland Cancer Treatment–for health professionals (PDQ®).http://www.cancer.gov/types/head-and-neck/hp/salivary-gland-treatment-pdq#link/_403_toc Accessed on February 17, 2016
- ↑ 6.0 6.1 6.2 Pleomorphic adenoma. Radiopedia. http://radiopaedia.org/cases/pleomorphic-adenoma-9 Accesed on April 28, 2016
- ↑ Białek EJ, Jakubowski W, Karpińska G (2003). "Role of ultrasonography in diagnosis and differentiation of pleomorphic adenomas: work in progress". Arch Otolaryngol Head Neck Surg. 129 (9): 929–33. doi:10.1001/archotol.129.9.929. PMID 12975263. Unknown parameter
|month=ignored (help) - ↑ Cohen EG, Patel SG, Lin O; et al. (2004). "Fine-needle aspiration biopsy of salivary gland lesions in a selected patient population". Arch Otolaryngol Head Neck Surg. 130 (6): 773–8. doi:10.1001/archotol.130.6.773. PMID 15210562. Unknown parameter
|month=ignored (help) - ↑ Batsakis JG, Sneige N, el-Naggar AK (1992). "Fine-needle aspiration of salivary glands: its utility and tissue effects". Ann Otol Rhinol Laryngol. 101 (2 Pt 1): 185–8. PMID 1739267. Unknown parameter
|month=ignored (help) - ↑ Wan YL, Chan SC, Chen YL; et al. (2004). "Ultrasonography-guided core-needle biopsy of parotid gland masses". AJNR Am J Neuroradiol. 25 (9): 1608–12. PMID 15502149. Unknown parameter
|month=ignored (help)