Claudication
For patient information click here Template:DiseaseDisorder infobox
| Cardiology Network |
 Discuss Claudication further in the WikiDoc Cardiology Network |
| Adult Congenital |
|---|
| Biomarkers |
| Cardiac Rehabilitation |
| Congestive Heart Failure |
| CT Angiography |
| Echocardiography |
| Electrophysiology |
| Cardiology General |
| Genetics |
| Health Economics |
| Hypertension |
| Interventional Cardiology |
| MRI |
| Nuclear Cardiology |
| Peripheral Arterial Disease |
| Prevention |
| Public Policy |
| Pulmonary Embolism |
| Stable Angina |
| Valvular Heart Disease |
| Vascular Medicine |
Template:WikiDoc Cardiology News
|
WikiDoc Resources for Claudication |
|
Articles |
|---|
|
Most recent articles on Claudication Most cited articles on Claudication |
|
Media |
|
Powerpoint slides on Claudication |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Claudication at Clinical Trials.gov Clinical Trials on Claudication at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Claudication
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Claudication Discussion groups on Claudication Patient Handouts on Claudication Directions to Hospitals Treating Claudication Risk calculators and risk factors for Claudication
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Claudication |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Please Join in Editing This Page and Apply to be an Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [3] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Overview
Claudication is a cramping sensation in the legs that is present during exercise or walking and occurs as a result of decreased oxygen supply.
This cramping usually occurs in the calf, but may also occur in the feet. When intermittent claudication is discussed it is measured by the number of "blocks" (e.g. 1 or 2 blocks) one can walk comfortably. It often indicates severe atherosclerosis. One of the hallmarks of this clinical entity is that it occurs intermittently. It disappears after a brief rest and the patient can start walking again until the pain recurs.
Intermittent claudication in and of itself is often a symptom of severe atherosclerotic disease of the peripheral vascular system. Claudication derives from the Latin verb claudicare, "to limp."
- It is not:
- pain at rest
- pain while standing, lying, or sitting
- pain that improves with walking
It reflects working muscle's ischemia.
Epidemiology
While 1 in 10 patients over the age of 65 will have peripheral arterial disease, aproximately 50% of these will have classical claudication symptoms. Intermittent claudication most commonly manifests in men older than 50 years. [1]
Pathophysiology
- Metabolic abnormalities stemming from reduced blood flow and O2 delivery
- Significant reduction (50%) in muscle fibers compared with controls
- Smaller type I and II muscle fibers with greater arterial ischemia
- Hyperplastic mitochondria and demyelination of nerve fibers
Signs
The location of pain depends upon the location of the disease. Buttock, thigh, calf or foot claudication, can occur either singly or in combination. The following signs are general signs of atherosclerosis of the lower extremity arteries:
- cyanosis
- atrophic changes like loss of hair, shiny skin
- decreased temperature
- decreased pulse
- redness when limb is returned to a "dependent" position
Mnemonics for signs of intermittent claudicatio;
All the "P's"
- Increase in Pallor
- Decrease in Pulses
- Perishing cold
- Pain
- Paraesthesia
- Paralysis
Aortoiliac occlusive disease (Leriche's syndrome) manifests with buttock and/or hip pain and in some cases, thigh claudication. Thigh pain is most often due to atherosclerotic occlusion of the common femoral artery may induce claudication in the thigh, calf, or both.
Calf cramping in the upper 2/3 of the calf is usually due to superficial femoral disease, while cramping in the lower 1/3 of the calf is due to popliteal disease.
-
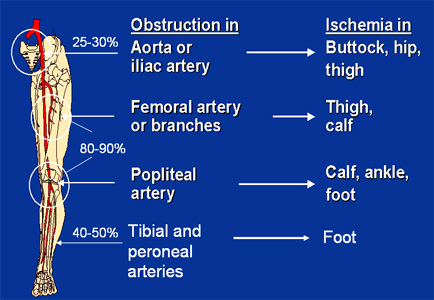
Sites of Claudication. Adapted from TCT 2005

The most frequently affected artery in intermittent claudication is the popliteal artery. Peripheral atherosclerosis related leg pain is relieved only by rest. Leg pain occurs in one leg in 40% of patients and in both legs in 60% of patients. Patients may also experience fatigue or pain in the thighs and buttocks.
In advanced cases, (Advanced Peripheral Artery Disease) the arteries are so blocked that even rest does not help. Leg pain that continues when lying down is called ischemic rest pain.
People with ischemic rest pain are at risk for ulcers and gangrene. In severe cases, amputation may be required.
Symptoms of advanced peripheral arterial disease can include:
- Calf muscles that shrink (wither)
- Hair loss over the toes and feet
- Thick toenails
- Shiny, tight skin
- Painful non-bleeding ulcers on the feet or toes (usually black) that are slow to heal
Physical Examination
A careful history taking and examination will generally distinguish intermittent claudication from nonvascular causes that may mimic claudication (pseudoclaudication).
The patient's lower legs and feet should be examined with shoes and socks off, with attention to pulses, hair loss, skin color, and trophic skin changes.
Differential Diagnosis of Claudication
| Cardiovascular | • Peripheral arterial disease • Claudication due to venous congestion (Venous claudication) • Deep vein thrombosis • Compartment Syndrome |
| Chemical / poisoning | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | No underlying causes |
| Ear Nose Throat | No underlying causes |
| Endocrine | No underlying causes |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | Pseudoxanthoma elasticum |
| Hematologic | No underlying causes |
| Iatrogenic | No underlying causes |
| Infectious Disease | No underlying causes |
| Musculoskeletal / Ortho | • Arthritis • Compartment Syndrome • |
| Neurologic | • Compartment Syndrome • Spinal stenosis • Spondylolisthesis |
| Nutritional / Metabolic | No underlying causes |
| Oncologic | No underlying causes |
| Opthalmologic | No underlying causes |
| Overdose / Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal / Electrolyte | No underlying causes |
| Rheum / Immune / Allergy | • Arthritis • |
| Trauma | No underlying causes |
| Miscellaneous | No underlying causes |
Diagnosis
- Ankle-Brachial Index
- Toe-Brachial Index: In patients with non-compressible vessels (usually patients with diabetes or renal failure), the diagnosis can be confirmed by measuring the toe–brachial index (determined according to the return of pulsatile flow on deflation of a small blood-pressure cuff on the great or second toe with a plethysmographic device). [2]
- Digital Subtraction Angiography (DSA): An invasive method. Ionizing radiation and iodinated contrast material used.
- Duplex ultrasound: Although it is widely available non-invasive tool to help to visualize and quantitate the lesion and its severity, this is an operator dependent tool. Duplex ultrasound's imaging ability is limited by dense calcifications.
- Computed Tomographic Angiography (CTA)[3]
- Magnetic Resonance Angiography (MRA)
Treatment
Treatment of intermittent claudication is combination of medical therapy and lifestyle changes. [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15]
- Smoking cessation: More than 80% of patients with peripheral arterial disease are current or former smokers. In patients who smoke, smoking cessation is the most effective treatment.
- Cholesterol lowering therapy [16] and Diet
- Regular Exercise: Exercise can improve symptoms as do medication to control the lipid profile, diabetes and hypertension.
- Regulating blood pressure.
- Diabetes management
- Using flat shoes
- Treatment for thrombophilia
- Surgery is only indicated in severe cases with limb-threatening ischemia or lifestyle-limiting claudication. The vascular surgeon will perform an endarterectomy of leg arteries or an arterial bypass.
- Patients with claudication or patients who have chronic critical limb ischemia, Percutaneous Transluminal Angioplasty (PTA) is not inferior to surgery, making the procedure associated with less morbidity the treatment of choice.[17] Furthermore, a failed lower extremity bypass is more likely to lead to tissue or limb loss than restenosis after PTA.[18] Unlike surgery, PTA can be repeated at no increased risk to the patient or limb,[19] and promising endovascular strategies to prevent restenosis may be used to maintain patency of the treated femoral popliteal segment.
- Angiotensin converting enzyme inhibitors (ACEI), beta-blockers, antiplatelet agents (ASA and clopidogrel), pentoxifylline and cilostazol are used for the treatment of intermittent claudication.
- Low molecular weight heparin (LMWH), oral anticoagulants (warfarin), vitamin E or chelation therapy is not effective.
References
- ↑ Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999-2000. Circulation 2004;110:738-743. PMID 15262830
- ↑ White C. Intermittent claudication. N Engl J Med 2007; 356: 1241-50.
- ↑ Ouwendijk R, de Vries M, Pattynama PM, et al. Imaging peripheral arterial disease: a randomized controlled trial comparing contrast-enhanced MR angiography and multi-detector row CT angiography. Radiology 2005;236:1094-1103.
- ↑ Leng GC, Lee AJ, Fowkes FG et al. Incidence, natural history and cardiovascular events in symptomatic and asymptomatic peripheral arterial disease in the general population. Int J Epidemiol 1995; 25: 1172-81.
- ↑ Kannel WB, McGee DI. Update on some epidemiological features of intermittent claudication. J Am Geriatr Soc 1985; 33: 13-18.
- ↑ Widmer LK, Greensher A, Kannel WB. Occlusion of peripheral arteries - a study of 6400 working subjects. Circulation 1964; 30: 836-842.
- ↑ Shearman CP. Management of intermittent claudication. Brit J Surg 2002; 89: 529-531.
- ↑ Davies A. The practical management of claudication. Brit Med J 2000; 321: 911-912.
- ↑ Burns P, Gough S, Bradbury AW. Management of peripheral arterial disease in primary care. Brit Med J 2003; 326: 584-588.
- ↑ Stewart KJ, Hiatt WR, Regensteiner JG, Hirsch AT. Exercise training for claudication. N Engl J Med 2002; 347: 1941-1951.
- ↑ Leng GC, Fowler B, Ernst E. Exercise for intermittent claudication (Cochrane Review). In The Cochrane Library Issue 4. Oxford: Update Software, 2001.
- ↑ Strandness DE, Dalman RL, Panian S et al. Effect of cilostazol in patients with intermittent claudication: a randomised, double blind, placebo-controlled study. Vasc Endovasc Surg 2002; 36: 83-91.
- ↑ Robless P, Mikhailidis DP, Stansby G. Systematic review of antiplatelet therapy for the prevention of myocardial infarction, stroke or vascular death in patients with peripheral vascular disease. Brit J Surg 2001; 88: 787-800.
- ↑ Caprie Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events. Lancet 1996; 348: 1329-39.
- ↑ Hankey GJ, Norman PE, Eikelboom JW. Medical treatment of peripheral arterial disease. JAMA 2006; 295: 547-553.
- ↑ Mohler ER, Hiatt WR, Creager MA. Cholesterol reduction with atorvastatin improves walking distance in patients with peripheral arterial disease. Circulation 2003;108:1481-6.
- ↑ Adam DJ, Beard JD, Cleveland T, et al. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomized controlled trial. Lancet 2005; 366: 1925-34.
- ↑ Baldwin ZK, Pearce BJ, Curi MA, et al. Limb salvage after infrainguinal bypass graft failure. J Vasc Surg 2004;39:951-7.
- ↑ Schillinger M, Mlekusch W, Haumer M, Sabeti S, Ahmadi R, Minar E. Angioplasty and elective stenting of de novo versus recurrent femoropopliteal lesions: 1-year follow-up. J Endovasc Ther 2003;10:288-97.
External Links and Patient Resources
- Atherosclerosis
- Peripheral artery occlusive disease
- Intermittent Claudication at NEJM
- Contrast-enhanced Periferal MRA
Acknowledgements
The content on this page was first contributed by: C. Michael Gibson, M.S., M.D.
de:Arterielle Verschlusskrankheit fi:Katkokävely it:Claudicatio intermittens nl:Etalagebenen sv:Fönstertittarsjukan