Venous insufficiency
| Venous insufficiency | |
 | |
|---|---|
| Venous insufficiency |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [2] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Overview
Venous insufficiency is a condition in which the veins do not efficiently return blood from the lower limbs back to the heart. Venous insufficiency involves one or more veins.
Normal Anatomy and Function
- The superficial veins lie in the subcutaneous fatty layer of the body just beneath the skin and superficial to the deep fascia enveloping the body musculature. The principal veins in the legs are the great and lesser saphenous veins and their tributaries; in the arms they are the basilic and cephalic veins and their tributaries.
- The deep veins accompany arteries and bear the same name as the arteries they parallel. It is common in the extremities for there to be two or more veins accompanying a small to medium sized artery.
- The perforating veins penetrate the deep fascia and connect the superficial veins to the deep veins. Those along the inner (medial) side of the lower leg play a major role in the pathogenesis of the postphlebitic leg.
- The intramuscular sinusoidal veins are large, very thin walled, valveless veins within skeletal muscle. They connect directly with the deep veins.
-
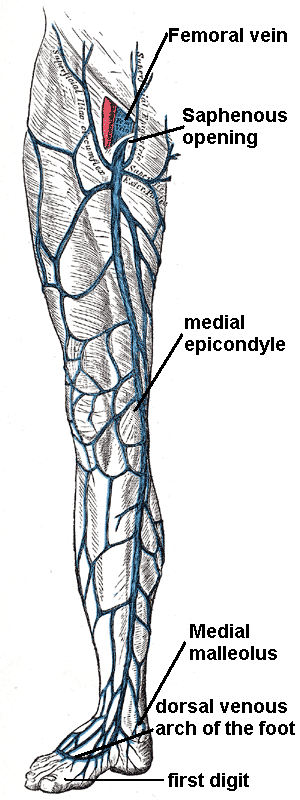
Great saphenous vein
-
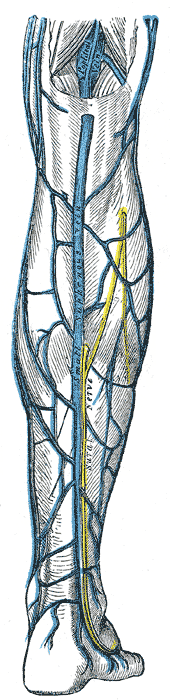
Small saphenous vein and its tributaries.
-
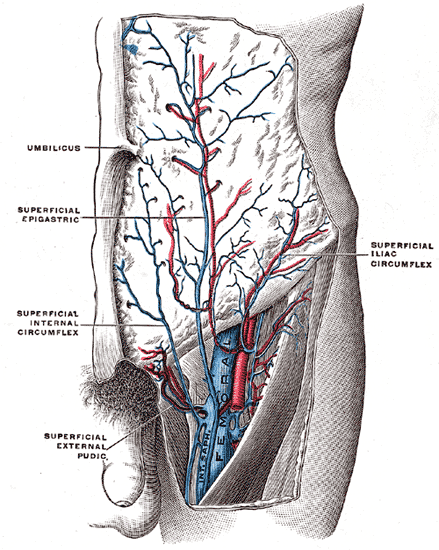
The femoral vein and its tributaries.

Function

Veins serve to return blood from organs to the heart.
In systemic circulation oxygenated blood is pumped by the left ventricle through the arteries to the muscles and organs of the body, where its nutrients and gases are exchanged at capillaries, entering the veins filled with cellular waste and carbon dioxide.
The de-oxygenated blood is taken by veins to the right atrium of the heart, which transfers the blood to the right ventricle, where it is then pumped to the pulmonary arteries and eventually the lungs.
In pulmonary circulation the pulmonary veins return oxygenated blood from the lungs to the left atrium, which empties into the left ventricle, completing the cycle of blood circulation. Normal venous flow is dependent on four factors:
- Dynamic Flow: The heart related flow (dynamics/spontaneous flow). Flow in the arterial system is dependent on the pumping action of the heart and the elasticity and muscular activity of the arteries.
- Phasic Flow: Respiration related factors. Phasic flow is the effects of respiration on normal venous flow. In the arms and neck, venous blood flow increases during inspiration due to the negative intrathoracic pressure. The opposite mechanism apply for lower extremities. During the inspiration, the diaphragms are lower and increase the intraabdominal pressure. During the expiration diaphragms are elevate and lower the intraabdominal pressure. This help to venous return from lower extremities.
- The muscle pump or the venous pump: The muscle pump mechanism is highly developed in the calf muscles. Large venous sinusoids located in these muscles. As they contract, the force helps to emptying the below veins. Contractions of the calf muscles can produce a sufficient pressure to empty the sinusoids into the deep veins. The deep veins are affected with the similar compressing force due to a strong fascial structure. As a result, with each muscle contraction venous blood is pumped towards to the heart.
- The valves: The valves are prevent retrograde flow. They prevent retrograde flow from heart to veins and from deep veins to superfacial veins.
Pathophysiology
Risk Factors
- Age
- Family history
- Sedentary lifestyle
Classification
- According to Clinical Presentation
- Asymptomatic
- Symptomatic
- According to Etiology
- Congenital
- Primary
- Secondary)
- According to Anatomical Localization / Distribution
- Superficial
- Deep
- Perforator
- Alone
- In combination
- According to Pathophysiological Dysfunction
- Reflux
- Obstruction
- Alone
- In combination
Diagnosis
Signs and Symptoms
- Leg discomfort and / or pain: Complains may include dull aching, heaviness, or cramping. Venous claudication may mimic arterial intermittent claudication, though it typically takes longer to subside after stopping exercise.
- Skin pigmentation and discoloration of the skin. Venous insufficiency is characterized by a dark bluish / purple discoloration. Over time, long standing stasis of blood leads to the deposition of hemosiderin, giving the skin a dark, speckled appearance. If the leg is placed in a dependent position, the bluish/purple discoloration may darken dramatically, further suggestive of venous insufficiency. This occurs as a result of gravity working against an already ineffective blood return system. Patients with severe arterial insufficiency, on the other hand, may have relatively pale skin as a result of under perfusion. When their legs are placed in a dependent position, gravity enhances arterial inflow and the skin may become more red as maximally dilated arterioles attempt to bring blood to otherwise starved tissues. In cases of severe ischemia, the affected areas (usually involving the most distal aspect of the foot), can appear whitish or mottled, giving the leg a marbleized appearance. Dead tissue turns black (a.k.a. gangrene). Cellulitis (infection in the skin) will cause the skin to appear bright red. These changes can be difficult to detect in people of color.
- Ulceration: Non-healing ulcers especially around the medial malleolus
- Lipodermatosclerosis: LDS or liposclerosis refers to a thickening in the tissues underneath the skin.
- Varicose eczema: the skin becomes red, wet and scaly.
- Leg swelling
Physical Examination
Doppler USG
Duplex scanning of the deep and superficial veins can detect obstruction. In addition, the function of valves in each segment of the evaluated veins can be assessed by determining the direction of blood-flow using Doppler ultrasound.
The examination is often done in the upright position, as this is the best way to evaluate valve function.
MRI
Computed Tomography
Venogram
Differential diagnosis of causes of venous insufficiency
Treatment
Pharmacotherapy
Compression Stockings
Stent Application
Surgery
Indication of surgery depends on color flow duplex ultrasound evaluation results. Following an examination there are four main levels of venous pathology:
- Superficial venous reflux only
- Deep venous reflux only
- Mixed superficial and deep venous reflux
- Occluded deep venous system
Sclerotherapy
Saphenous Venous Ablation (Closure)
- Endovenous laser ablation (EVLA) is a relatively simple and quick technique which can be performed under a local anesthetic. Endovenous laser techniques employ an 810 nm-diode laser to heat the long or short saphenous vein (or major tributaries), inducing a combination of endothelial damage, focal
coagulative necrosis, shrinkage of the vein and thrombotic occlusion.
- Radiofrequency ablation
Complications
Prevention
Examination Findings
-

Venous insufficiency
-

-

Assymetric Leg, Swelling secondary to Deep Venous Thrombosis in Right Leg
-

Venous Stasis Ulcer
-

Edema of Right Foot
-

Massive edema





References
Additional Resources
See Also
External Links
Template:Veins Template:VeinsHeadNeck Template:Veins of the upper extremity Template:Veins of the lower extremity Template:SIB