Squamous cell carcinoma of the lung pathophysiology: Difference between revisions
No edit summary |
YazanDaaboul (talk | contribs) No edit summary |
||
| Line 5: | Line 5: | ||
==Overview== | ==Overview== | ||
Squamous cell carcinoma of the lung arises from the [[epithelial]] cells of the lung of the central [[bronchi]] to terminal [[alveoli]], which are normally involved in the protection of the airways. The pathological irritation caused by cigarette smoke causes the mucus-secreting ciliated pseudostratified columnar respiratory epithelial cells that line the airways to be replaced by stratified squamous epithelium. Squamous cell carcinoma of the lung has a central location | Squamous cell carcinoma of the lung arises from the [[epithelial]] cells of the lung of the central [[bronchi]] to terminal [[alveoli]], which are normally involved in the protection of the airways. The pathological irritation caused by cigarette smoke causes the mucus-secreting ciliated pseudostratified columnar respiratory epithelial cells that line the airways to be replaced by stratified squamous epithelium. Squamous cell carcinoma of the lung has a central location and usually appears as a hiliar or perihiliar mass. Squamous cell carcinoma of the lung is a rapidly growing cancer which may metastasize to various organs of the body. Genes involved in the pathogenesis of squamous cell carcinoma include several oncogenes, such as: [[EGFR|''EGFR'']]'', EML-4, [[KRAS]], [[HER2/neu|HER2]],'' and [[ALK-1|''ALK'']].<ref name="pmid22722794">{{cite journal |vauthors=Heist RS, Sequist LV, Engelman JA |title=Genetic changes in squamous cell lung cancer: a review |journal=J Thorac Oncol |volume=7 |issue=5 |pages=924–33 |year=2012 |pmid=22722794 |pmc=3404741 |doi=10.1097/JTO.0b013e31824cc334 |url=}}</ref> On gross pathology, findings include central necrosis, cavitation, and invasion of peribronchial soft tissue. On microscopic histopathological analysis squamous cell carcinoma of the lung demonstrate large polygonal malignant cells containing keratin and intercellular bridges.<ref name="pmid16107574">{{cite journal |vauthors=Miller YE |title=Pathogenesis of lung cancer: 100 year report |journal=Am. J. Respir. Cell Mol. Biol. |volume=33 |issue=3 |pages=216–23 |year=2005 |pmid=16107574 |pmc=2715312 |doi=10.1165/rcmb.2005-0158OE |url=}}</ref> On inmunohistochemistry, findings associated with squamous cell carcinoma of the lung include the presence of [[p53]] and high-molecular weight keratins for squamous cell carcinoma. Other squamous immunomarkers, include: CK5/6, CEA, 34BE12, TTF-1, and CK7.<ref name="pmid16107574">{{cite journal |vauthors=Miller YE |title=Pathogenesis of lung cancer: 100 year report |journal=Am. J. Respir. Cell Mol. Biol. |volume=33 |issue=3 |pages=216–23 |year=2005 |pmid=16107574 |pmc=2715312 |doi=10.1165/rcmb.2005-0158OE |url=}}</ref> | ||
==Pathogenesis== | ==Pathogenesis== | ||
*Squamous cell carcinoma of the lung arises from bronchial epithelial cell damage ( usually related with active smoking) | *Squamous cell carcinoma of the lung arises from bronchial epithelial cell damage (usually related with active smoking). | ||
*Pathological irritation caused by cigarette smoke causes the mucus-secreting ciliated [[Pseudostratified epithelium|pseudostratified columnar respiratory epithelial cells]] that line the airways to be replaced by stratified squamous epithelium | *Pathological irritation caused by cigarette smoke causes the mucus-secreting ciliated [[Pseudostratified epithelium|pseudostratified columnar respiratory epithelial cells]] that line the airways to be replaced by stratified squamous epithelium. | ||
*The [[squamous metaplasia]] is then followed by epithelial dysplasia, which consists of an expansion of immature cells with a corresponding decrease in the number and location of mature cells | *The [[squamous metaplasia]] is then followed by epithelial dysplasia, which consists of an expansion of immature cells with a corresponding decrease in the number and location of mature cells. | ||
*[[Dysplasia]] is often indicative of an early neoplastic process | *[[Dysplasia]] is often indicative of an early neoplastic process in squamous cell carcinoma of the lung. | ||
*Squamous cell carcinoma of the lung has a central location | *Squamous cell carcinoma of the lung has a central location and usually appears as a hiliar or perihiliar mass. | ||
*Squamous cell carcinoma of the lung is a rapidly growing cancer which may metastasize to | *Squamous cell carcinoma of the lung is a rapidly growing cancer which may metastasize to various organs of the body. | ||
*Basaloid lung cell carcinoma is the most aggressive subtype of squamous cell carcinoma of the lung | *Basaloid lung cell carcinoma is the most aggressive subtype of squamous cell carcinoma of the lung. | ||
===Molecular Pathogenesis=== | ===Molecular Pathogenesis=== | ||
* Squamous cell carcinoma of the lung is a [[diploid]] or hyperdiploid [[aneuploid]] neoplasm with mean chromosome numbers in the triploid range<ref name="pmid24488911">{{cite journal |vauthors=Shi WY, Liu KD, Xu SG, Zhang JT, Yu LL, Xu KQ, Zhang TF |title=Gene expression analysis of lung cancer |journal=Eur Rev Med Pharmacol Sci |volume=18 |issue=2 |pages=217–28 |year=2014 |pmid=24488911 |doi= |url=}}</ref> | * Squamous cell carcinoma of the lung is a [[diploid]] or hyperdiploid [[aneuploid]] neoplasm with mean chromosome numbers in the triploid range.<ref name="pmid24488911">{{cite journal |vauthors=Shi WY, Liu KD, Xu SG, Zhang JT, Yu LL, Xu KQ, Zhang TF |title=Gene expression analysis of lung cancer |journal=Eur Rev Med Pharmacol Sci |volume=18 |issue=2 |pages=217–28 |year=2014 |pmid=24488911 |doi= |url=}}</ref> | ||
* In squamous cell carcinoma of the lung, there is a multitude of alterations with amplifications of the telomeric 3q region | * In squamous cell carcinoma of the lung, there is a multitude of alterations with amplifications of the telomeric 3q region. | ||
* Gain of 3q24-qter is present in the majority of squamous cell carcinomas of the lung | * Gain of 3q24-qter is present in the majority of squamous cell carcinomas of the lung. | ||
* Disruption of normal [[p53 gene]] is frequent in squamous cell carcinoma of the lung<ref name="pmid24488911">{{cite journal |vauthors=Shi WY, Liu KD, Xu SG, Zhang JT, Yu LL, Xu KQ, Zhang TF |title=Gene expression analysis of lung cancer |journal=Eur Rev Med Pharmacol Sci |volume=18 |issue=2 |pages=217–28 |year=2014 |pmid=24488911 |doi= |url=}}</ref> | * Disruption of normal [[p53 gene]] is frequent in squamous cell carcinoma of the lung.<ref name="pmid24488911">{{cite journal |vauthors=Shi WY, Liu KD, Xu SG, Zhang JT, Yu LL, Xu KQ, Zhang TF |title=Gene expression analysis of lung cancer |journal=Eur Rev Med Pharmacol Sci |volume=18 |issue=2 |pages=217–28 |year=2014 |pmid=24488911 |doi= |url=}}</ref> | ||
==Genetics== | ==Genetics== | ||
* Development of squamous cell carcinoma of the lung is the result of multiple [[genetic mutation]]s. | * Development of squamous cell carcinoma of the lung is the result of multiple [[genetic mutation]]s. | ||
* Genetic mutations play an important role in the treatment selection for squamous cell carcinoma of the lung. | * Genetic mutations play an important role in the treatment selection for squamous cell carcinoma of the lung. | ||
* [[Genes]] involved in the pathogenesis of squamous cell carcinoma | * [[Genes]] involved in the pathogenesis of squamous cell carcinoma include the following:<ref name="pmid24488911">{{cite journal |vauthors=Shi WY, Liu KD, Xu SG, Zhang JT, Yu LL, Xu KQ, Zhang TF |title=Gene expression analysis of lung cancer |journal=Eur Rev Med Pharmacol Sci |volume=18 |issue=2 |pages=217–28 |year=2014 |pmid=24488911 |doi= |url=}}</ref> | ||
:*[[EGFR]] | :*[[EGFR|''EGFR'']] | ||
::*84% of squamous cell carcinomas of the lung are positive for EGFR | ::*84% of squamous cell carcinomas of the lung are positive for ''EGFR'' | ||
:*EML-4 | :*''EML-4'' | ||
:*[[ALK-1|ALK]] | :*[[ALK-1|''ALK'']] | ||
:*[[KRAS]] | :*[[KRAS|''KRAS'']] | ||
::*30% of squamous cell carcinomas of the lung are positive for KRAS | ::*30% of squamous cell carcinomas of the lung are positive for ''KRAS'' | ||
:*[[HER2/neu|HER2]] | :*[[HER2/neu|''HER2'']] | ||
::*Rare in squamous cell carcinomas of the lung | ::*Rare in squamous cell carcinomas of the lung | ||
==Associated Conditions== | ==Associated Conditions== | ||
*Conditions associated with squamous cell carcinoma of the lung | *Conditions associated with squamous cell carcinoma of the lung include:<ref name="pmid24488911">{{cite journal |vauthors=Shi WY, Liu KD, Xu SG, Zhang JT, Yu LL, Xu KQ, Zhang TF |title=Gene expression analysis of lung cancer |journal=Eur Rev Med Pharmacol Sci |volume=18 |issue=2 |pages=217–28 |year=2014 |pmid=24488911 |doi= |url=}}</ref> | ||
:*[[Pancoast tumor]] | :*[[Pancoast tumor]] | ||
:*[[Horner's syndrome]] | :*[[Horner's syndrome]] | ||
==Gross Pathology== | ==Gross Pathology== | ||
*On gross pathology, findings associated with squamous cell carcinoma of the lung | *On gross pathology, findings associated with squamous cell carcinoma of the lung include:<ref name="pathology">Non small cell lung cancer. Libre Pathology. http://librepathology.org/wiki/Non-small_cell_lung_carcinoma Accessed on February 22, 2016 </ref> | ||
:* | :*Lung mas that is usually centrally located | ||
:*Invasion of peribronchial soft-tissue, lymph nodes, and lung parenchyma | :*Invasion of peribronchial soft-tissue, lymph nodes, and lung parenchyma | ||
:* | :*Large mass causing compression of pulmonary artery and vein | ||
:*[[Cavitation|Central cavitation]] | |||
:* | |||
==Microscopic Pathology== | ==Microscopic Pathology== | ||
*On microscopic pathology, findings associated with squamous cell carcinoma of the lung | *On microscopic pathology, findings associated with squamous cell carcinoma of the lung include:<ref name="pathology">Non small cell lung cancer. Libre Pathology. http://librepathology.org/wiki/Non-small_cell_lung_carcinoma Accessed on February 22, 2016 </ref> | ||
:*Central nucleus | :*Central nucleus | ||
:*Dense appearing cytoplasm, usually eosinophilic | :*Dense appearing cytoplasm, usually eosinophilic | ||
| Line 56: | Line 54: | ||
:*Intracellular bridges (classic feature) | :*Intracellular bridges (classic feature) | ||
*On inmunohistochemistry, findings associated with squamous cell carcinoma of the lung | *On inmunohistochemistry, findings associated with squamous cell carcinoma of the lung include:<ref name="pmid16107574">{{cite journal |vauthors=Miller YE |title=Pathogenesis of lung cancer: 100 year report |journal=Am. J. Respir. Cell Mol. Biol. |volume=33 |issue=3 |pages=216–23 |year=2005 |pmid=16107574 |pmc=2715312 |doi=10.1165/rcmb.2005-0158OE |url=}}</ref> | ||
:*Presence of p63 and high-molecular weight keratins for squamous cell carcinoma | :*Presence of p63 and high-molecular weight keratins for squamous cell carcinoma | ||
:*Other squamous immunomarkers include CK5/6, CEA, 34BE12, TTF-1, and CK7 | :*Other squamous immunomarkers include CK5/6, CEA, 34BE12, TTF-1, and CK7 | ||
:*Differentiation of squamous cell carcinoma of the lung from adenocarcinoma is vital as response to cytotoxic and biological agents will differ | :*Differentiation of squamous cell carcinoma of the lung from adenocarcinoma on biopsy is vital as response to cytotoxic and biological agents will greatly differ | ||
==Gallery== | ==Gallery== | ||
Revision as of 19:06, 25 April 2016
|
Squamous Cell Carcinoma of the Lung Microchapters |
|
Differentiating Squamous Cell Carcinoma of the Lung from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Squamous cell carcinoma of the lung pathophysiology On the Web |
|
American Roentgen Ray Society Images of Squamous cell carcinoma of the lung pathophysiology |
|
Squamous cell carcinoma of the lung pathophysiology in the news |
|
Blogs on Squamous cell carcinoma of the lung pathophysiology |
|
Directions to Hospitals Treating Squamous cell carcinoma of the lung |
|
Risk calculators and risk factors for Squamous cell carcinoma of the lung pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Maria Fernanda Villarreal, M.D. [2]
Overview
Squamous cell carcinoma of the lung arises from the epithelial cells of the lung of the central bronchi to terminal alveoli, which are normally involved in the protection of the airways. The pathological irritation caused by cigarette smoke causes the mucus-secreting ciliated pseudostratified columnar respiratory epithelial cells that line the airways to be replaced by stratified squamous epithelium. Squamous cell carcinoma of the lung has a central location and usually appears as a hiliar or perihiliar mass. Squamous cell carcinoma of the lung is a rapidly growing cancer which may metastasize to various organs of the body. Genes involved in the pathogenesis of squamous cell carcinoma include several oncogenes, such as: EGFR, EML-4, KRAS, HER2, and ALK.[1] On gross pathology, findings include central necrosis, cavitation, and invasion of peribronchial soft tissue. On microscopic histopathological analysis squamous cell carcinoma of the lung demonstrate large polygonal malignant cells containing keratin and intercellular bridges.[2] On inmunohistochemistry, findings associated with squamous cell carcinoma of the lung include the presence of p53 and high-molecular weight keratins for squamous cell carcinoma. Other squamous immunomarkers, include: CK5/6, CEA, 34BE12, TTF-1, and CK7.[2]
Pathogenesis
- Squamous cell carcinoma of the lung arises from bronchial epithelial cell damage (usually related with active smoking).
- Pathological irritation caused by cigarette smoke causes the mucus-secreting ciliated pseudostratified columnar respiratory epithelial cells that line the airways to be replaced by stratified squamous epithelium.
- The squamous metaplasia is then followed by epithelial dysplasia, which consists of an expansion of immature cells with a corresponding decrease in the number and location of mature cells.
- Dysplasia is often indicative of an early neoplastic process in squamous cell carcinoma of the lung.
- Squamous cell carcinoma of the lung has a central location and usually appears as a hiliar or perihiliar mass.
- Squamous cell carcinoma of the lung is a rapidly growing cancer which may metastasize to various organs of the body.
- Basaloid lung cell carcinoma is the most aggressive subtype of squamous cell carcinoma of the lung.
Molecular Pathogenesis
- Squamous cell carcinoma of the lung is a diploid or hyperdiploid aneuploid neoplasm with mean chromosome numbers in the triploid range.[3]
- In squamous cell carcinoma of the lung, there is a multitude of alterations with amplifications of the telomeric 3q region.
- Gain of 3q24-qter is present in the majority of squamous cell carcinomas of the lung.
- Disruption of normal p53 gene is frequent in squamous cell carcinoma of the lung.[3]
Genetics
- Development of squamous cell carcinoma of the lung is the result of multiple genetic mutations.
- Genetic mutations play an important role in the treatment selection for squamous cell carcinoma of the lung.
- Genes involved in the pathogenesis of squamous cell carcinoma include the following:[3]
-
- 84% of squamous cell carcinomas of the lung are positive for EGFR
- 30% of squamous cell carcinomas of the lung are positive for KRAS
- Rare in squamous cell carcinomas of the lung
Associated Conditions
- Conditions associated with squamous cell carcinoma of the lung include:[3]
Gross Pathology
- On gross pathology, findings associated with squamous cell carcinoma of the lung include:[4]
- Lung mas that is usually centrally located
- Invasion of peribronchial soft-tissue, lymph nodes, and lung parenchyma
- Large mass causing compression of pulmonary artery and vein
- Central cavitation
Microscopic Pathology
- On microscopic pathology, findings associated with squamous cell carcinoma of the lung include:[4]
- Central nucleus
- Dense appearing cytoplasm, usually eosinophilic
- Small nucleolus
- Intracellular bridges (classic feature)
- On inmunohistochemistry, findings associated with squamous cell carcinoma of the lung include:[2]
- Presence of p63 and high-molecular weight keratins for squamous cell carcinoma
- Other squamous immunomarkers include CK5/6, CEA, 34BE12, TTF-1, and CK7
- Differentiation of squamous cell carcinoma of the lung from adenocarcinoma on biopsy is vital as response to cytotoxic and biological agents will greatly differ
Gallery
-

Gross pathology: bronchial squamous lung cell cancer
-
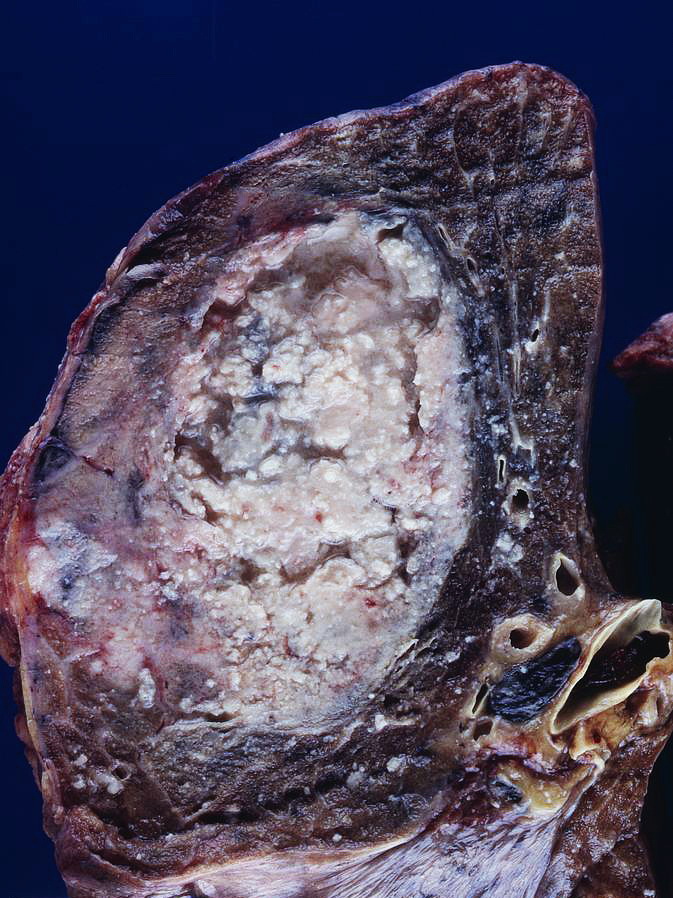
Gross pathology: Squamous lung cell cancer
-
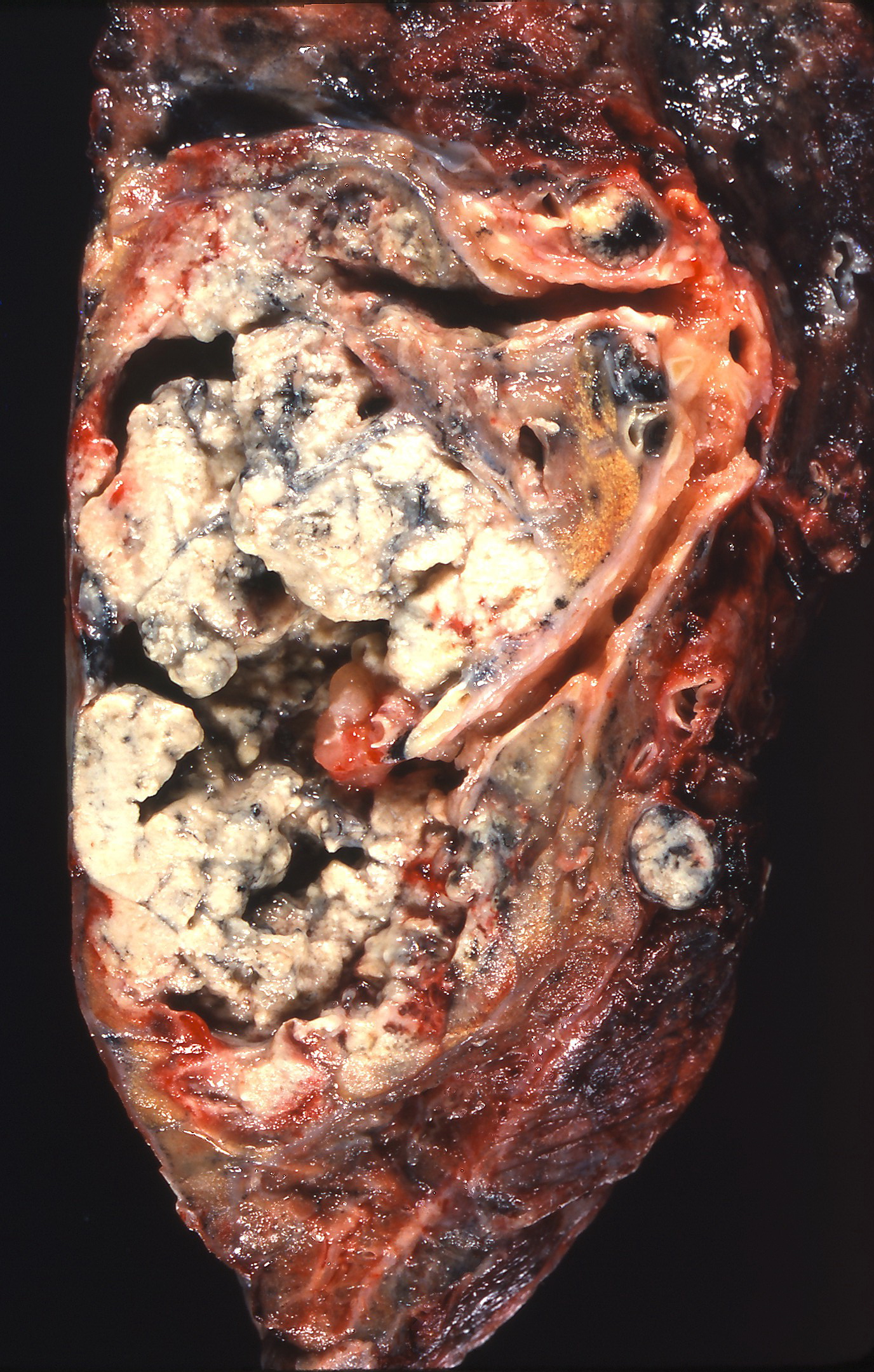
Gross pathology: cavitation, squamous lung cell cancer
-
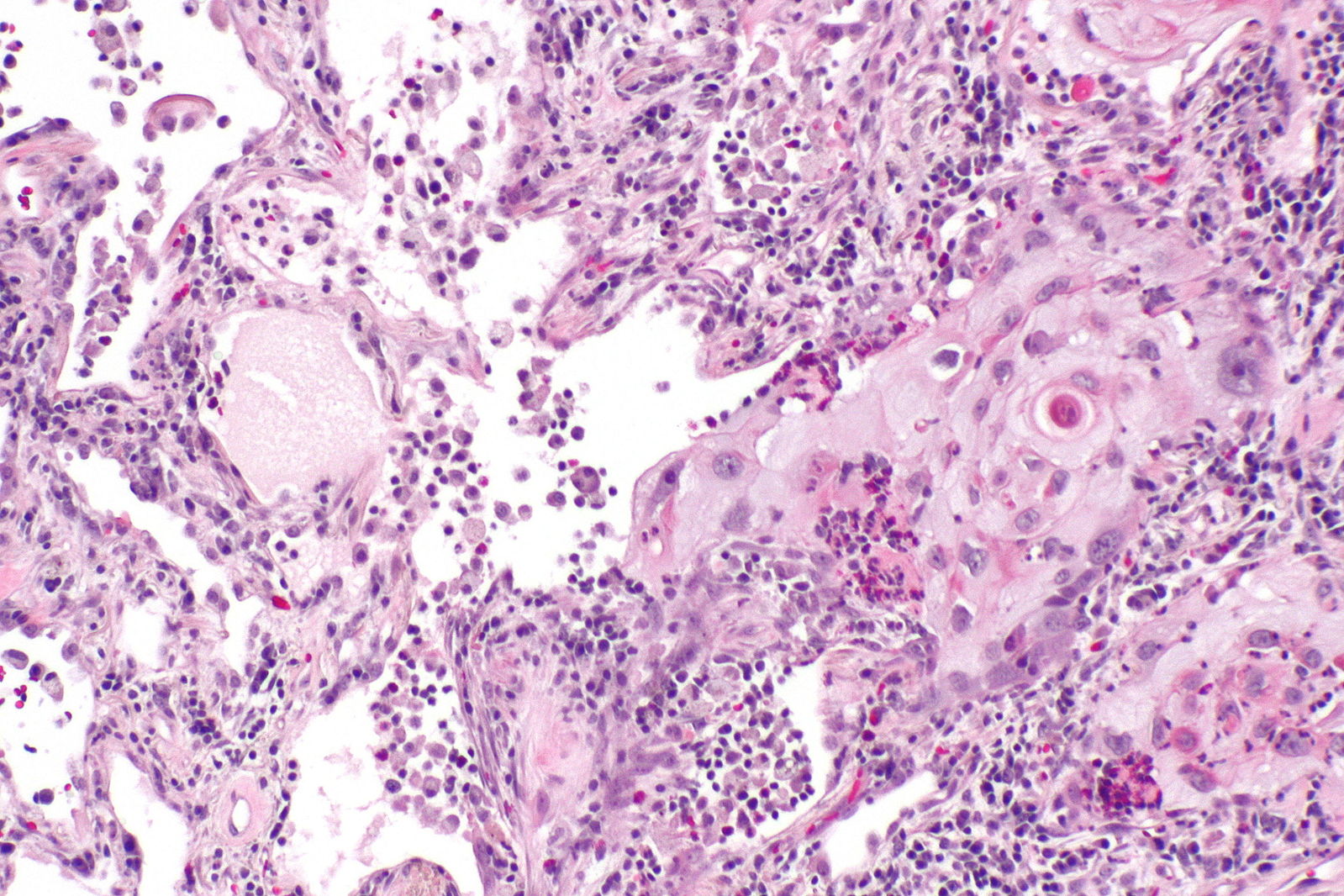
Micropathology: Squamous cell carcinoma of the lung. H&E stain
-
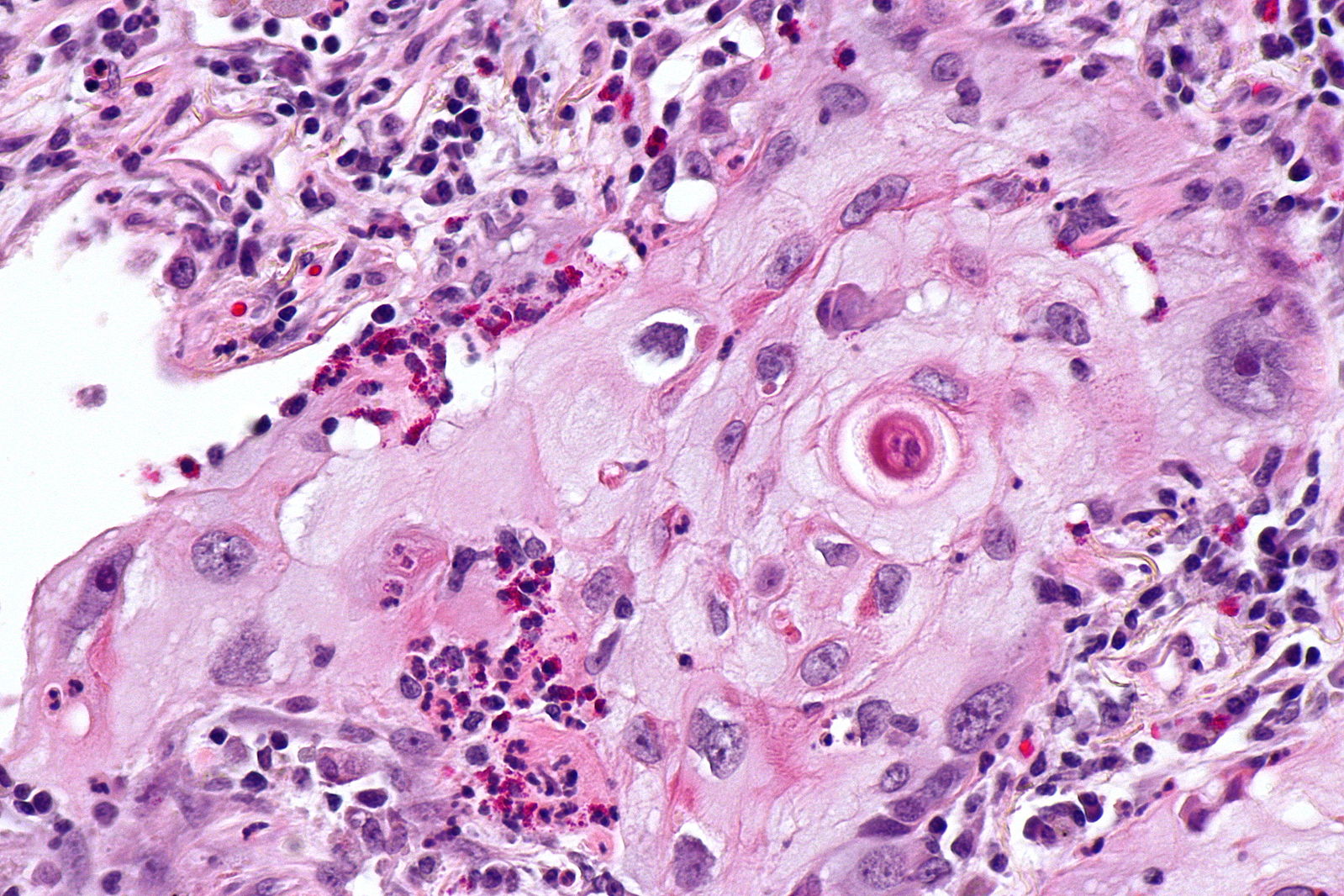
Micropathology: Squamous cell carcinoma of the lung. H&E stain





References
- ↑ Heist RS, Sequist LV, Engelman JA (2012). "Genetic changes in squamous cell lung cancer: a review". J Thorac Oncol. 7 (5): 924–33. doi:10.1097/JTO.0b013e31824cc334. PMC 3404741. PMID 22722794.
- ↑ 2.0 2.1 2.2 Miller YE (2005). "Pathogenesis of lung cancer: 100 year report". Am. J. Respir. Cell Mol. Biol. 33 (3): 216–23. doi:10.1165/rcmb.2005-0158OE. PMC 2715312. PMID 16107574.
- ↑ 3.0 3.1 3.2 3.3 Shi WY, Liu KD, Xu SG, Zhang JT, Yu LL, Xu KQ, Zhang TF (2014). "Gene expression analysis of lung cancer". Eur Rev Med Pharmacol Sci. 18 (2): 217–28. PMID 24488911.
- ↑ 4.0 4.1 Non small cell lung cancer. Libre Pathology. http://librepathology.org/wiki/Non-small_cell_lung_carcinoma Accessed on February 22, 2016