De Quervain's thyroiditis other diagnostic studies: Difference between revisions
(Created page with "__NOTOC__ {{De Quervain's thyroiditis }} {{CMG}} {{MMF}} ==Overview== ==References== {{reflist|2}}") |
m (Bot: Removing from Primary care) |
||
| (41 intermediate revisions by 4 users not shown) | |||
| Line 1: | Line 1: | ||
__NOTOC__ | __NOTOC__ | ||
{{De Quervain's thyroiditis }} | {{De Quervain's thyroiditis }} | ||
{{CMG}} {{MMF}} | {{CMG}}; {{AE}} {{MMF}} | ||
==Overview== | ==Overview== | ||
The histological analysis in de Quervain's thyroiditis may show the destruction of the follicular [[epithelium]], loss of the follicular integrity, and infiltration of [[inflammatory cells]]. [[FNA|Fine needle aspiration cytology]] helps to differentiate between the [[Thyroid nodule|benign]] and [[Thyroid nodule|malignant nodules]]. | |||
==Other Diagnostic Studies== | |||
===Microscopic Pathology=== | |||
Microscopic findings suggesting [[de Quervain's thyroiditis]] are as followings:<ref name="pmid12608662">{{cite journal |vauthors=Kojima M, Nakamura S, Oyama T, Sugihara S, Sakata N, Masawa N |title=Cellular composition of subacute thyroiditis. an immunohistochemical study of six cases |journal=Pathol. Res. Pract. |volume=198 |issue=12 |pages=833–7 |year=2002 |pmid=12608662 |doi=10.1078/0344-0338-00344 |url=}}</ref> | |||
*[[Granuloma]] comprises of [[colloid]], small [[Lymphocyte|lymphocytes]], [[neutrophil]]<nowiki/>s, and [[Macrophage|macrophages]] with or without epithelioid features | |||
*Destruction of the follicular [[epithelium]] | |||
*Loss of the follicular integrity | |||
*Patchy distribution of [[Granulomas|non-caseous granulomas]] | |||
===Fine needle aspiration cytology=== | |||
[[Needle aspiration biopsy|Fine needle aspiration]] is usually done under [[ultrasound]] guidance and the sample is sent for [[cytology]]. It helps to differentiate [[Thyroid nodule|benign thyroid nodules]] from the [[malignant]] lesions.<ref name="urlThyroiditis — NEJM">{{cite web |url=http://www.nejm.org/doi/full/10.1056/NEJMra021194 |title=Thyroiditis — NEJM |format= |work= |accessdate=}}</ref><ref name="pmid12727961">{{cite journal |vauthors=Fatourechi V, Aniszewski JP, Fatourechi GZ, Atkinson EJ, Jacobsen SJ |title=Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study |journal=J. Clin. Endocrinol. Metab. |volume=88 |issue=5 |pages=2100–5 |year=2003 |pmid=12727961 |doi=10.1210/jc.2002-021799 |url=}}</ref> | |||
==Gallery== | |||
<gallery> | |||
Image:Subacute thyroiditis - intermed mag.jpg|center|thumb|250px|'''Histology of De Quervain's thyroiditis; Granuloma'''<SMALL><SMALL> (By Nephron - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=18491382)</SMALL></SMALL> | |||
Image:Subacute thyroiditis - high mag.jpg|center|thumb|250px|'''Histology of De Quervain's thyroiditis; Granuloma'''<SMALL><SMALL> (By Nephron - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=18491421)</SMALL></SMALL> | |||
Image:Subacute thyroiditis - very high mag.jpg|center|thumb|250px|'''Histology of De Quervain's thyroiditis; Granuloma'''<SMALL><SMALL> (By Nephron - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=18491421)</SMALL></SMALL> | |||
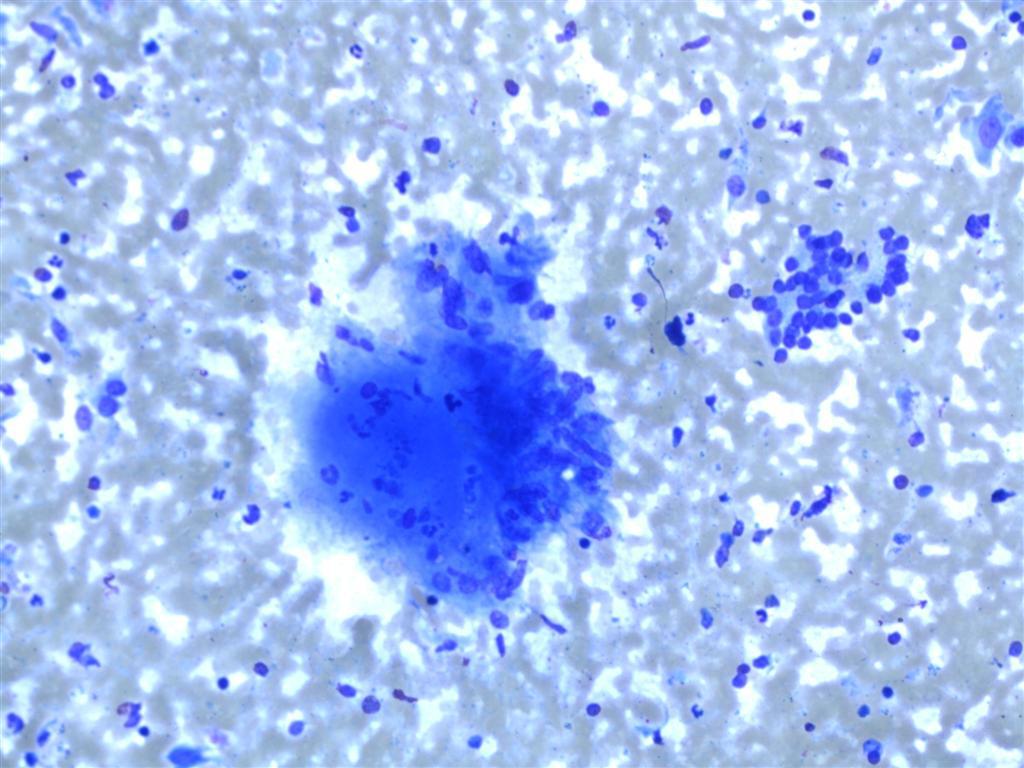
Image:Subacute-de-quervains-thyroiditis (3).jpg|center|thumb|250px|'''FNA smear of De Quervain's thyroiditis; '''Inflammatory rich smear with giant cells and probable granulomata.<SMALL><SMALL> (Case courtesy of Dr Andrew Ryan, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/17052">rID: 17052</a>)]])</SMALL></SMALL> | |||
Image:Subacute-de-quervains-thyroiditis (4).jpg|center|thumb|250px|'''FNA smear of De Quervain's thyroiditis; '''; Cluster of epithelioid histiocytes with associated inflammatory cells and debris and group of benign follicular epithelial cells.<SMALL><SMALL> (Case courtesy of Dr Andrew Ryan, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/17052">rID: 17052</a>)</SMALL></SMALL> | |||
</gallery> | |||
==References== | ==References== | ||
{{reflist|2}} | {{reflist|2}} | ||
| |||
[[Category:Medicine]] | |||
[[Category:Endocrinology]] | |||
[[Category:Up-To-Date]] | |||
Latest revision as of 21:14, 29 July 2020
|
De Quervain's thyroiditis Microchapters |
|
Differentiating De Quervain's thyroiditis from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Furqan M M. M.B.B.S[2]
Overview
The histological analysis in de Quervain's thyroiditis may show the destruction of the follicular epithelium, loss of the follicular integrity, and infiltration of inflammatory cells. Fine needle aspiration cytology helps to differentiate between the benign and malignant nodules.
Other Diagnostic Studies
Microscopic Pathology
Microscopic findings suggesting de Quervain's thyroiditis are as followings:[1]
- Granuloma comprises of colloid, small lymphocytes, neutrophils, and macrophages with or without epithelioid features
- Destruction of the follicular epithelium
- Loss of the follicular integrity
- Patchy distribution of non-caseous granulomas
Fine needle aspiration cytology
Fine needle aspiration is usually done under ultrasound guidance and the sample is sent for cytology. It helps to differentiate benign thyroid nodules from the malignant lesions.[2][3]
Gallery
-
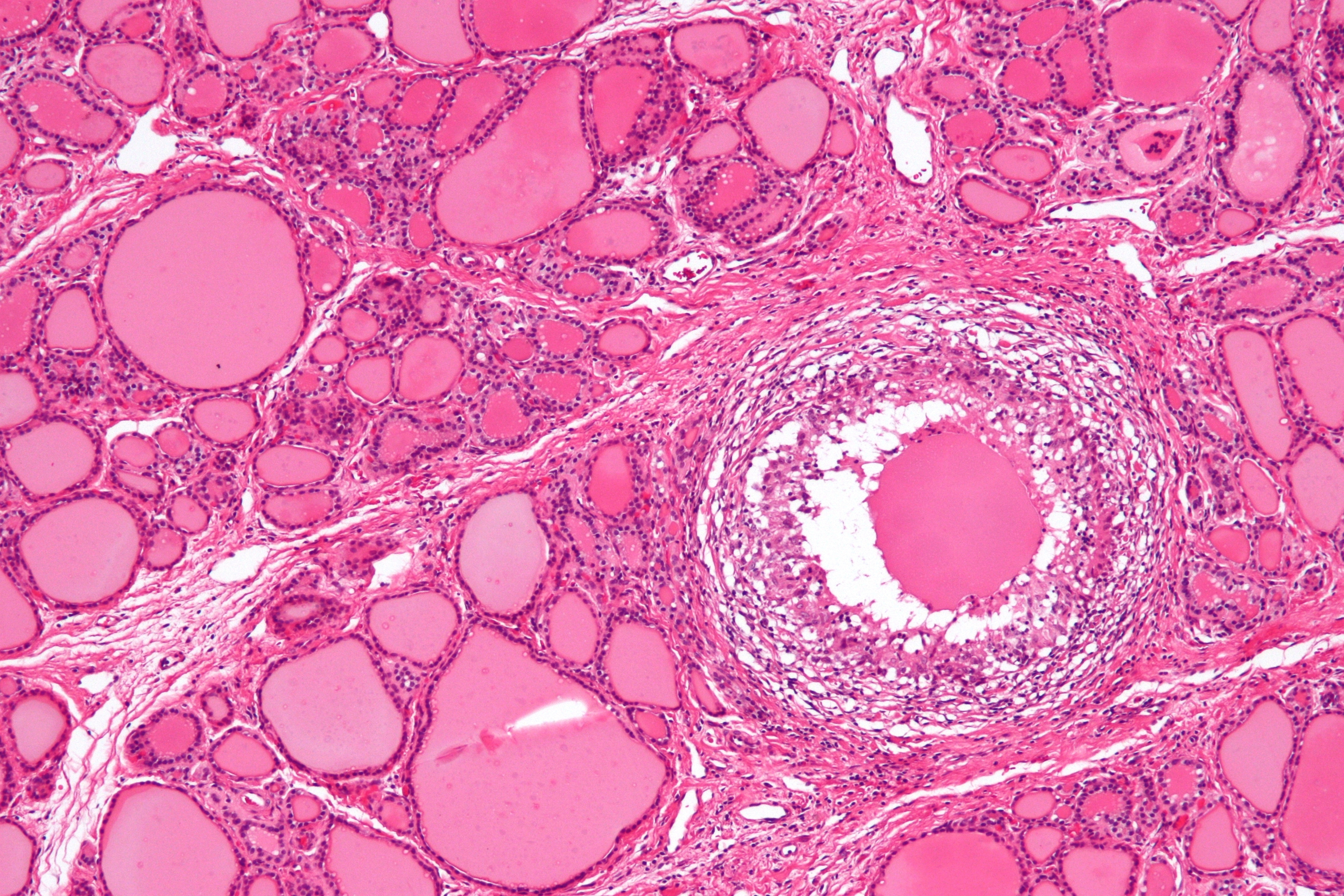
Histology of De Quervain's thyroiditis; Granuloma (By Nephron - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=18491382)
-
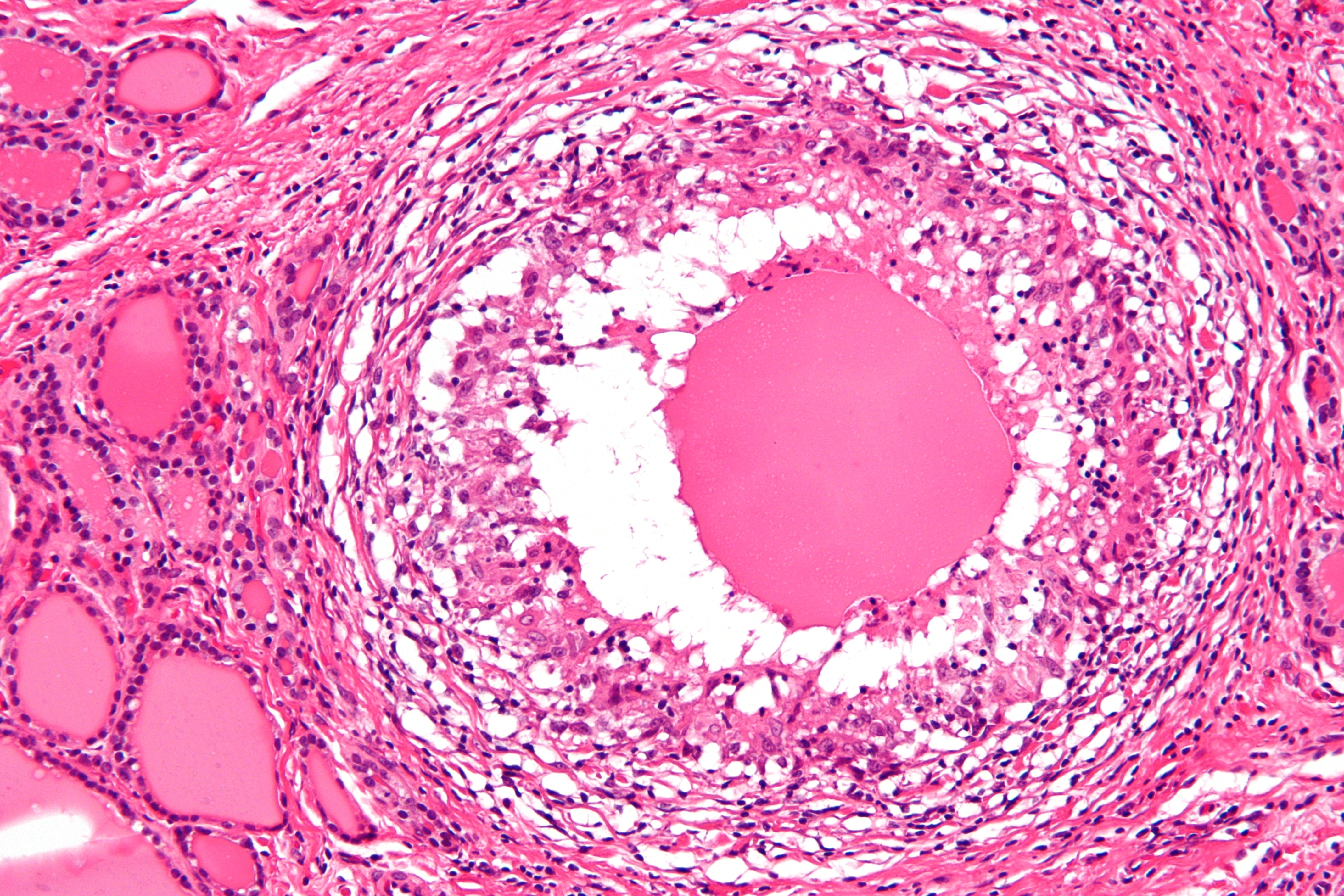
Histology of De Quervain's thyroiditis; Granuloma (By Nephron - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=18491421)
-
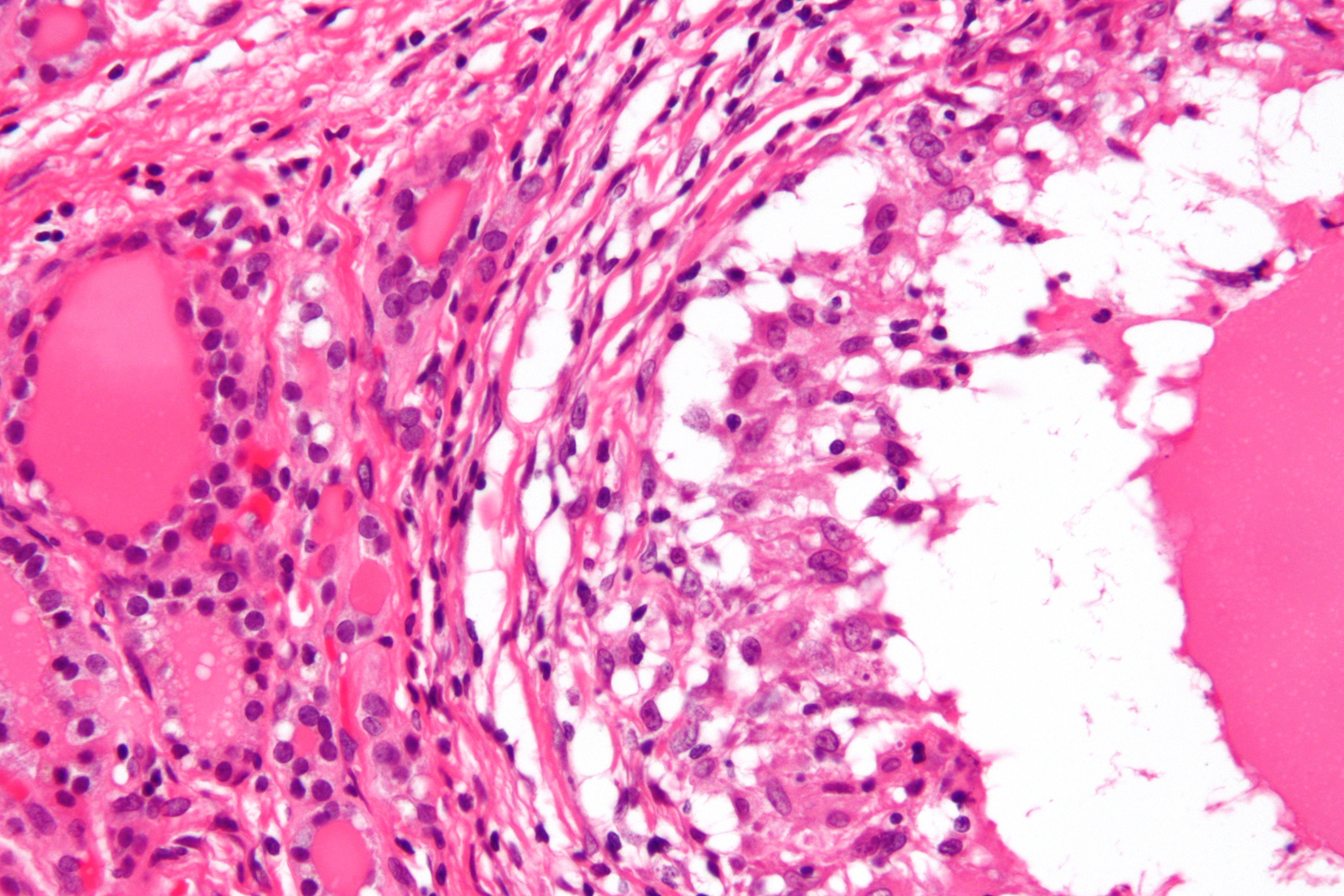
Histology of De Quervain's thyroiditis; Granuloma (By Nephron - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=18491421)
-
![FNA smear of De Quervain's thyroiditis; Inflammatory rich smear with giant cells and probable granulomata. (Case courtesy of Dr Andrew Ryan, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/17052">rID: 17052</a>)]])](/images/1/1c/Subacute-de-quervains-thyroiditis_%283%29.jpg)
FNA smear of De Quervain's thyroiditis; Inflammatory rich smear with giant cells and probable granulomata. (Case courtesy of Dr Andrew Ryan, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/17052">rID: 17052</a>)]])
-
FNA smear of De Quervain's thyroiditis; ; Cluster of epithelioid histiocytes with associated inflammatory cells and debris and group of benign follicular epithelial cells. (Case courtesy of Dr Andrew Ryan, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/17052">rID: 17052</a>)



![FNA smear of De Quervain's thyroiditis; Inflammatory rich smear with giant cells and probable granulomata. (Case courtesy of Dr Andrew Ryan, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/17052">rID: 17052</a>)]])](/index.php/File:Subacute-de-quervains-thyroiditis_(3).jpg)
.jpg)
References
- ↑ Kojima M, Nakamura S, Oyama T, Sugihara S, Sakata N, Masawa N (2002). "Cellular composition of subacute thyroiditis. an immunohistochemical study of six cases". Pathol. Res. Pract. 198 (12): 833–7. doi:10.1078/0344-0338-00344. PMID 12608662.
- ↑ "Thyroiditis — NEJM".
- ↑ Fatourechi V, Aniszewski JP, Fatourechi GZ, Atkinson EJ, Jacobsen SJ (2003). "Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted County, Minnesota, study". J. Clin. Endocrinol. Metab. 88 (5): 2100–5. doi:10.1210/jc.2002-021799. PMID 12727961.