Mixed connective tissue disease: Difference between revisions
Tamar Sifri (talk | contribs) |
No edit summary |
||
| Line 1: | Line 1: | ||
__NOTOC__ | __NOTOC__ | ||
{{SI}} | {{SI}} | ||
{{CMG}}; | {{CMG}}; {{AE}} {{CZ}}, {{JH}} | ||
{{SK}} MCTD; mixed connective tissue disorder; Sharp's syndrome | {{SK}} MCTD; mixed connective tissue disorder; Sharp's syndrome | ||
==Overview== | ==Overview== | ||
'''Mixed connective tissue disease''' ('''MCTD''') or ''Sharp's syndrome'' is a human [[autoimmune disease]] in which the [[immune system]] attacks the body. MCTD combines features of [[polymyositis]], [[systemic lupus erythematosus]], and [[systemic scleroderma]] and is thus considered an [[overlap syndrome]]. MCTD commonly causes [[arthritis|joint pain/swelling]], [[Raynaud phenomenon]], [[myositis|muscle inflammation]], and [[sclerodactyly|scarring of the skin of the hand]]. It does not typically cause [[kidney]] disease or [[seizure]]s. Distinguishing laboratory characteristics are a positive, speckled [[anti-nuclear antibody]] and an [[anti-U1-RNP antibody]].<ref>Venables PJ. ''Mixed connective tissue disease.'' Lupus. 2006;15(3):132-7. PMID 1663436</ref> | '''Mixed connective tissue disease''' ('''MCTD''') or ''Sharp's syndrome'' is a human [[autoimmune disease]] in which the [[immune system]] attacks the body. MCTD combines features of [[polymyositis]], [[systemic lupus erythematosus]], and [[systemic scleroderma]] and is thus considered an [[overlap syndrome]]. MCTD commonly causes [[arthritis|joint pain/swelling]], [[Raynaud phenomenon]], [[myositis|muscle inflammation]], and [[sclerodactyly|scarring of the skin of the hand]]. It does not typically cause [[kidney]] disease or [[seizure]]s. Distinguishing laboratory characteristics are a positive, speckled [[anti-nuclear antibody]] and an [[anti-U1-RNP antibody]].<ref>Venables PJ. ''Mixed connective tissue disease.'' Lupus. 2006;15(3):132-7. PMID 1663436</ref> | ||
| Line 17: | Line 18: | ||
</gallery> | </gallery> | ||
</div> | </div> | ||
===Mixed Connective Tissue | ==Historical Perspective== | ||
==Classification== | |||
==Pathophysiology== | |||
*Associated Conditions: | |||
**[[Systemic lupus erythematosus]]–like findings | |||
***[[Polyarthritis]] | |||
***[[Lymphadenopathy]] | |||
***Facial [[erythema]] | |||
***[[Pericarditis]] or [[pleuritis]] | |||
***[[Leukopenia]] (<4,000/mm3) or thrombocytopenia (<100,000/mm3) | |||
**[[Scleroderma|Progressive Systemic Sclerosis]] –like findings | |||
***[[Sclerodactyly]] | |||
***[[Pulmonary fibrosis]], restrictive changes of the lung (forced vital capacity <80% of predicted), or reduced carbon monoxide diffusing capacity (<70% of predicted) | |||
**[[Polymyositis]]-like findings | |||
==Causes== | |||
==Differentiating Mixed Connective Tissue Disease from other Diseases== | |||
==Epidemiology and Demographics== | |||
===Age=== | |||
===Gender=== | |||
===Race=== | |||
==Risk Factors== | |||
== | ==Natural History, Complications and Prognosis== | ||
Cardiovascular abnormalities associated with mixed connective tissue disease are rare. Presence of any of the complications listed below indicates unfavorable prognosis; | Cardiovascular abnormalities associated with mixed connective tissue disease are rare. Presence of any of the complications listed below indicates unfavorable prognosis; | ||
*Acute [[pericarditis]] and/or [[pericardial effusion]], | *Acute [[pericarditis]] and/or [[pericardial effusion]], | ||
| Line 56: | Line 74: | ||
</div> | </div> | ||
==Physical examination== | ==Diagnosis== | ||
===Diagnostic Criteria=== | |||
===Symptoms=== | |||
*[[Raynaud’s phenomenon]] | |||
*Swollen fingers or hands | |||
*Muscle weakness | |||
===Physical examination=== | |||
===Gallery=== | ====Gallery==== | ||
====Trunk==== | =====Trunk===== | ||
<gallery> | <gallery> | ||
| Line 68: | Line 92: | ||
</gallery> | </gallery> | ||
====Extremities==== | =====Extremities===== | ||
<gallery> | <gallery> | ||
| Line 77: | Line 101: | ||
</gallery> | </gallery> | ||
===Laboratory Findings=== | |||
*Elevated serum level of muscle enzymes (creatine kinase) | |||
*MCTD is characterized by anti–U1 small nuclear RNP positivity. | |||
===Imaging Findings=== | |||
**Myogenic pattern on electromyogram | |||
===Other Diagnostic Studies=== | |||
**Hypomotility or dilatation of esophagus | |||
== References == | == References == | ||
{{reflist|2}} | {{reflist|2}} | ||
Revision as of 15:38, 6 July 2016
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2], Jesus Rosario Hernandez, M.D. [3]
Synonyms and keywords: MCTD; mixed connective tissue disorder; Sharp's syndrome
Overview
Mixed connective tissue disease (MCTD) or Sharp's syndrome is a human autoimmune disease in which the immune system attacks the body. MCTD combines features of polymyositis, systemic lupus erythematosus, and systemic scleroderma and is thus considered an overlap syndrome. MCTD commonly causes joint pain/swelling, Raynaud phenomenon, muscle inflammation, and scarring of the skin of the hand. It does not typically cause kidney disease or seizures. Distinguishing laboratory characteristics are a positive, speckled anti-nuclear antibody and an anti-U1-RNP antibody.[1]
Pathophysiology
There are no specific histologic findings that aid in the diagnosis of Mixed Connective Tissue Disorder as a separate autoimmune disease. For example, nephritis in MCTD is usually indistinguishable from lupus nephritis.
-
 Fibrous Pericarditis in MCTD
Fibrous Pericarditis in MCTD -
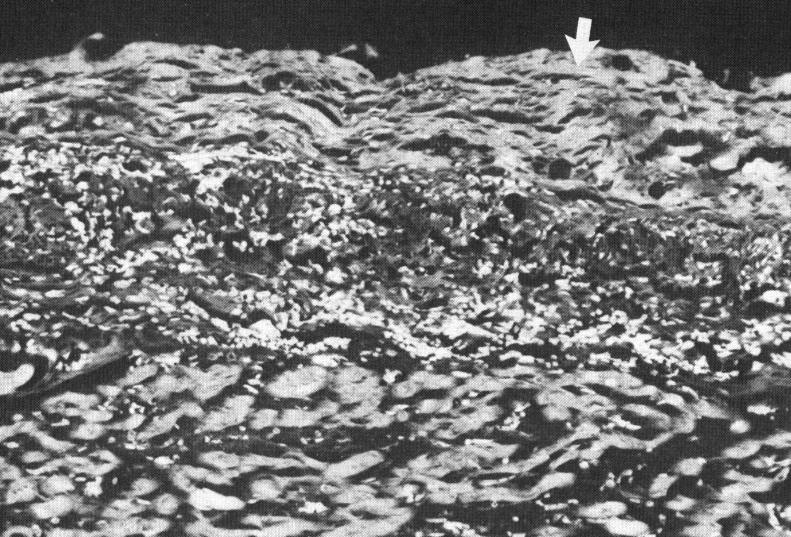
 Cellular aggregates in perivascular space and adjacent myocardium
Cellular aggregates in perivascular space and adjacent myocardium -
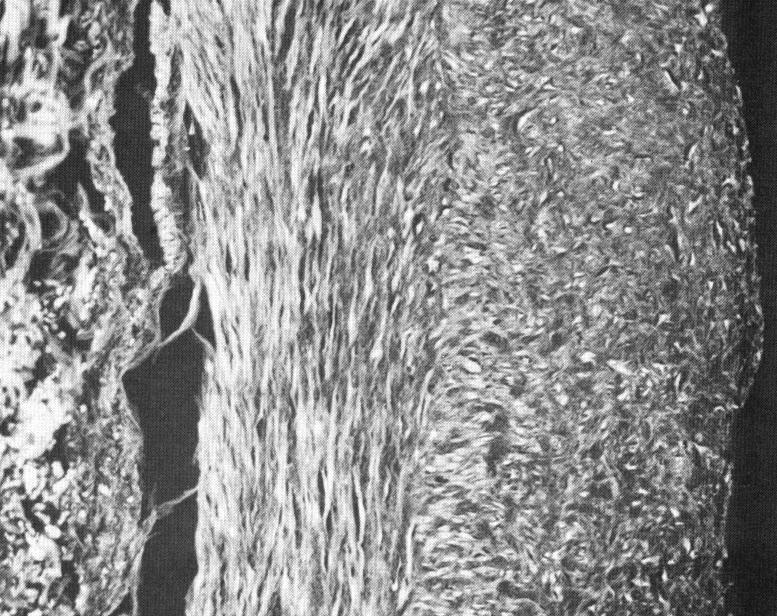 Cross Section of Intramural Coronary Artery
Cross Section of Intramural Coronary Artery -
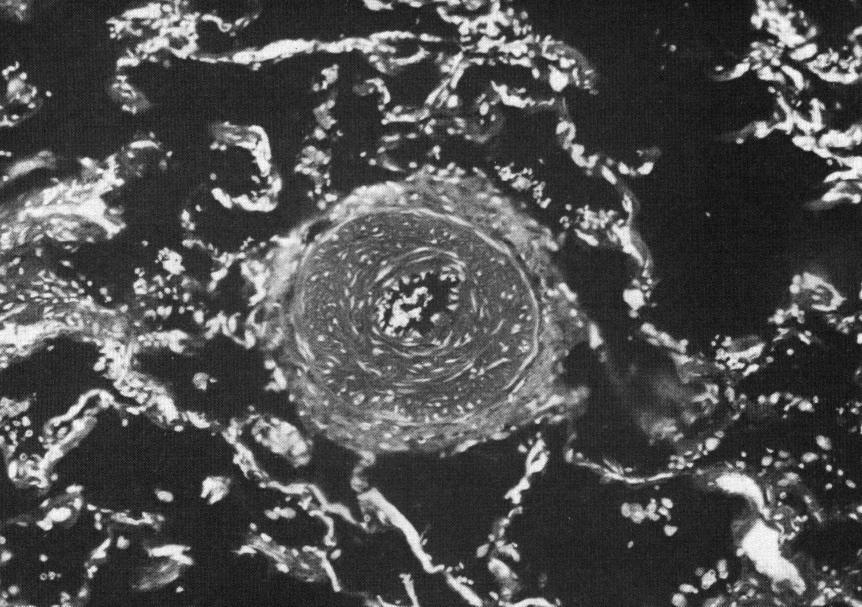 Small pulmonary artery in patient with MCTD and pulmnonary hypertension
Small pulmonary artery in patient with MCTD and pulmnonary hypertension




Historical Perspective
Classification
Pathophysiology
- Associated Conditions:
- Systemic lupus erythematosus–like findings
- Polyarthritis
- Lymphadenopathy
- Facial erythema
- Pericarditis or pleuritis
- Leukopenia (<4,000/mm3) or thrombocytopenia (<100,000/mm3)
- Progressive Systemic Sclerosis –like findings
- Sclerodactyly
- Pulmonary fibrosis, restrictive changes of the lung (forced vital capacity <80% of predicted), or reduced carbon monoxide diffusing capacity (<70% of predicted)
- Polymyositis-like findings
- Systemic lupus erythematosus–like findings
Causes
Differentiating Mixed Connective Tissue Disease from other Diseases
Epidemiology and Demographics
Age
Gender
Race
Risk Factors
Natural History, Complications and Prognosis
Cardiovascular abnormalities associated with mixed connective tissue disease are rare. Presence of any of the complications listed below indicates unfavorable prognosis;
- Acute pericarditis and/or pericardial effusion,
- Mitral valve prolapse,
- Intimal hyperplasia of coronary arteries,
- Perivascular and myocardial leukocytic infiltrates,
- Pulmonary hypertension.
- Coronary Artery Disease (although it is rarer, ACS may occur secondary to vascular changes and underlying CAD. The youngest patient with MCTD and ACS in literature was 18 years old)[2]
-
 A teenager with MCTD presented as ACS before PCI
A teenager with MCTD presented as ACS before PCI -
 A teenager with MCTD presented as ACS post PCI
A teenager with MCTD presented as ACS post PCI


Diagnosis
Diagnostic Criteria
Symptoms
- Raynaud’s phenomenon
- Swollen fingers or hands
- Muscle weakness
Physical examination
Gallery
Trunk

Extremities


Laboratory Findings
- Elevated serum level of muscle enzymes (creatine kinase)
- MCTD is characterized by anti–U1 small nuclear RNP positivity.
Imaging Findings
- Myogenic pattern on electromyogram
Other Diagnostic Studies
- Hypomotility or dilatation of esophagus