Intracranial aneurysms: Difference between revisions
No edit summary |
|||
| (162 intermediate revisions by 7 users not shown) | |||
| Line 1: | Line 1: | ||
{{ | __NOTOC__ | ||
{{Infobox Disease | |||
| Name = {{PAGENAME}} | |||
| Image = Berry aneurysm in anterior cerebral artery.jpg | |||
| Caption = Berry aneurysm in anterior cerebral artery | |||
}} | }} | ||
{{SI}} | {{SI}} | ||
'''For patient information, click [[Intracranial aneurysms (patient information)|here]]''' | |||
{{Editor | {{CMG}}; '''Associate Editor-In-Chief:''' {{CZ}}, {{Fs}} | ||
{{SK}} Anterior cerebral artery aneurysm; anterior communicating artery aneurysm; aneurysm of anterior communicating artery; intracranial aneurysm; middle cerebral artery aneurysm; posterior cerebral artery aneurysm; posterior communicating artery aneurysm; brain aneurysm; giant intracranial aneurysm; aneurysm in the brain | |||
==Overview== | ==Overview== | ||
The catastrophic potential of intracranial aneurysms, [[arteriovenous malformation]]s (AVMs), and [[arteriovenous fistula]]s (AVFs) and the complexity of their pathogenesis have made them the subject of intense interest and study over the past 80 years. Advances in the ability to treat these lesions have been paralleled by rigorous research on their pathophysiology. An increase in the longevity of the population over the past century and improvements in imaging techniques contribute to more frequent encounters with these lesions by neurosurgeons and interventionists. Despite numerous clinical and laboratory research projects studying the pathophysiology of these lesions, much remains to be learned. In this chapter, we will discuss the pathophysiology of various types of intracranial aneurysms, as well as AVMs and AVFs. | |||
The catastrophic potential of intracranial aneurysms, arteriovenous | |||
==Berry Aneurysms== | ==Berry Aneurysms== | ||
''Main article: [[Intracranial berry aneurysm|Berry Aneurysm]]'' | |||
Berry | [[Berry aneurysm]]s arise at vessel bifurcations or curves. These aneurysms occur mostly between the ages of 40 and 70 years. The pathogenesis of berry aneurysms is multifactorial. Compelling evidence suggests that hemodynamic factors as well as degenerative histological changes in the parent vessel wall contribute to aneurysm formation. Early in the process of berry aneurysm formation, destruction and eventual loss of the media occur<ref name="Stehbens">Stehbens W. The pathogenesis of intracranial aneurysms. In: Tindall GT CP, Barrow DL, editor. The Practice of Neurosurgery. Baltimore: Williams and Wilkins; 1996. p. 1941-1952.</ref>. The internal elastic layer becomes disrupted and is eventually lost. | ||
The mechanisms by which these changes occur are not well understood but have been attributed in part to atherosclerotic changes. This weakening in the vessel wall sets the stage for hemodynamic forces to cause saccular dilation ( | The mechanisms by which these changes occur are not well understood but have been attributed in part to atherosclerotic changes. This weakening in the vessel wall sets the stage for hemodynamic forces to cause saccular dilation<ref name=""Stehbens2">Stehbens WE. Flow in glass models of arterial bifurcations and berry aneurysms at low Reynolds numbers. Q J Exp Physiol Cogn Med Sci 1975;60(3):181-192.</ref>. Reduced peripheral resistance in the intracranial circulation, along with more rapid blood flow, may be associated with an augmented pulse pressure, which can lead to saccular dilation<ref name="Stehbens">Stehbens W. The pathogenesis of intracranial aneurysms. In: Tindall GT CP, Barrow DL, editor. The Practice of Neurosurgery. Baltimore: Williams and Wilkins; 1996. p. 1941-1952.</ref>. Recent studies have demonstrated that hemodynamic stress in vascular walls can result in alterations in extracellular matrix organization<ref name="Kittelberger">Kittelberger R, Davis PF, Stehbens WE. Distribution of type IV collagen, laminin, nidogen and fibronectin in the haemodynamically stressed vascular wall. Histol Histopathol 1990;5(2):161-167.</ref>. Turbulent flow in aneurysmal sacs damages the endothelium and results in laminar necrosis of the wall and expansion of the aneurysm. If a small aneurysm does not rupture, partial healing occurs through mural thrombus formation followed by organization of the thrombus with scarring of the wall, invasion of fibroblasts, collagen formation, platelet aggregation, and deposition of fibrous material. Repeat hemorrhages can occur in the wall, leading to repetitive cycles of abnormal healing and aneurysm growth. Giant aneurysms are believed to form by these mechanisms<ref name="Steinberg">Steinberg GK CM. Morphology and structural pathology. In: Awad IA B, DL, editor. Giant Intracranial Aneurysms. Park Ridge: AANS; 1995. p. 1-11.</ref>. | ||
Several risk factors and associated conditions have been linked with intracranial aneurysm growth and rupture. Smoking has been associated with larger berry aneurysm size and multiple aneurysms ( | Several risk factors and associated conditions have been linked with intracranial aneurysm growth and rupture. Smoking has been associated with larger berry aneurysm size and multiple aneurysms<ref name="Qureshi 1">Qureshi AI, Suarez JI, Parekh PD, Sung G, Geocadin R, Bhardwaj A, et al. Risk factors for multiple intracranial aneurysms. Neurosurgery 1998;43(1):22-27.</ref> <ref name="Qureshi 2">Qureshi AI, Sung GY, Suri MF, Straw RN, Guterman LR, Hopkins LN. Factors associated with aneurysm size in patients with subarachnoid hemorrhage: effect of smoking and aneurysm location. Neurosurgery 2000;46(1):44-50.</ref> <ref name="Qureshi 3">Qureshi AI, Suri MF, Yahia AM, Suarez JI, Guterman LR, Hopkins LN, et al. Risk factors for subarachnoid hemorrhage. Neurosurgery 2001;49(3):607-613.</ref>. Alcohol abuse has been associated with aneurysm rupture<ref name="Qureshi 3">Qureshi AI, Suri MF, Yahia AM, Suarez JI, Guterman LR, Hopkins LN, et al. Risk factors for subarachnoid hemorrhage. Neurosurgery 2001;49(3):607-613.</ref>. The role of hypertension in aneurysm formation has been controversial in the literature. Hypertension as a direct cause of aneurysms has never been established; however, it is believed that hypertension may exacerbate a rupture when it occurs and may contribute to aneurysm growth. Several conditions have been associated with a greater propensity for berry aneurysms. These conditions include coarctation of the aorta, polycystic kidney disease, and various connective tissue disorders such as Ehlers-Danlos syndrome<ref name="Stehbens">Stehbens W. The pathogenesis of intracranial aneurysms. In: Tindall GT CP, Barrow DL, editor. The Practice of Neurosurgery. Baltimore: Williams and Wilkins; 1996. p. 1941-1952.</ref>. | ||
Ninety percent of symptomatic berry aneurysms occur in the anterior circulation and 10% in the posterior circulation. In a prospective autopsy study, the mean size of ruptured aneurysms was 8.6 mm and of unruptured was 4.7 mm | Ninety percent of symptomatic berry aneurysms occur in the anterior circulation and 10% in the posterior circulation. In a prospective autopsy study, the mean size of ruptured aneurysms was 8.6 mm and of unruptured was 4.7 mm<ref name="Chason">Chason J. Berry aneurysms of the circle of Willis: results of a planned autopsy study. Neurology 1958;8:41-44.</ref>. Eighty percent of symptomatic aneurysms are under 12 mm in size<ref name="Weir">Weir B. Intracranial aneurysms. In: Wilkins RH RS, editor. Neurosurgery: McGraw Hill; 1985. p. 1308-1329.</ref>. Multiple aneurysms occur in approximately 15% of cases<ref name="Suzuki">Suzuki J. Multiple aneurysms: treatment. In: Pia HW LC, Zierski J, editor. Cerebral aneurysms: advances in diagnosis and therapy. Berlin: Springer; 1979. p. 352-363.</ref>. Most aneurysm ruptures occur between the fourth and seventh decades<ref name="Weir">Weir B. Intracranial aneurysms. In: Wilkins RH RS, editor. Neurosurgery: McGraw Hill; 1985. p. 1308-1329.</ref>. Saccular aneurysms become symptomatic owing to rupture, mass effect, or embolic events. The precise pathophysiology of rupture is not yet clearly understood, but it is believed that structural and hemodynamic factors play a role. The pathophysiology of aneurysmal SAH is beyond the scope of this chapter. Subarachnoid hemorrhage is associated with severe morbidity and mortality. Vasospasm, stroke, hydrocephalus, and seizures are some of the neurological consequences. Overall, approximately 50% of patients who experience SAH die within the first month; and approximately 30% of survivors have moderate to severe disability<ref name="Hop">Hop JW, Rinkel GJ, Algra A, van Gijn J. Case-fatality rates and functional outcome after subarachnoid hemorrhage: a systematic review. Stroke 1997;28(3):660-664.</ref><ref name="Mayberg">Mayberg MR, Batjer HH, Dacey R, Diringer M, Haley EC, Heros RC, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage. A statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Circulation 1994;90(5):2592-2605.</ref><ref name="Bendok">Bendok BR, Getch CC, Malisch TW, Batjer HH. Treatment of aneurysmal subarachnoid hemorrhage. Semin Neurol 1998;18(4):521-531.</ref>. | ||
==Inflammatory Aneurysms== | ==Inflammatory Aneurysms== | ||
''Main article: [[Mycotic aneurysm|Mycotic Aneurysm]]'' | |||
There are two types of inflammatory aneurysms: | |||
* Bacterial aneurysms (which are often referred to erroneously as mycotic) | |||
* Fungal or true mycotic aneurysms | |||
A review by Frazee et al.<ref name="Frazee">Frazee JG, Cahan LD, Winter J. Bacterial intracranial aneurysms. J Neurosurg 1980;53(5):633-641.</ref> summarized the reported cases of bacterial aneurysms in the literature between 1954 and 1980. The age of the patients ranged from 7 months to 78 years (average age, 30 years). Most patients had a history of either congenital heart disease, recent dental work, pulmonary infection, or carious teeth. Historically, patients with bacterial endocarditis were believed to have a risk of 4 to 15% of developing an intracranial aneurysm<ref name="Bohmfalk">Bohmfalk GL, Story JL, Wissinger JP, Brown WE, Jr. Bacterial intracranial aneurysm. J Neurosurg 1978;48(3):369-382.</ref>. Improvements in treatment over the past 2 decades are most likely responsible for the significant reduction in these numbers today. Streptococcus is the most common cause of bacterial aneurysms, followed by Staphylococcus. Other less commonly reported infecting organisms include Neisseria, Enterococcus, and Pseudomonas<ref name="Stehbens">Stehbens W. The pathogenesis of intracranial aneurysms. In: Tindall GT CP, Barrow DL, editor. The Practice of Neurosurgery. Baltimore: Williams and Wilkins; 1996. p. 1941-1952.</ref>. In addition to their association with [[endocarditis]], bacterial aneurysms have been reported in conjunction with meningitis and cavernous sinus thrombophlebitis, as well as following cardiac valvular surgery and intravenous drug abuse. Inflammatory aneurysms typically occur on distal cerebral vessels. This fact is a distinguishing feature from the more common berry aneurysms, which are found proximally on the [[circle of Willis]]. | |||
Work on a canine model by Molinari et al. suggests that the pathophysiology of inflammatory aneurysms relates to the lodging of an infected embolus in a distal cerebral vessel<ref name="Molinari">Molinari GF, Smith L, Goldstein MN, Satran R. Pathogenesis of cerebral mycotic aneurysms. Neurology 1973;23(4):325-332.</ref>. This group lodged bacterial-laden clots in the distal cerebral vasculature, which caused aneurysm formation. In their model, aneurysms formed within 3 days of the embolus being lodged. In this model, antibiotic administration did not prevent aneurysm formation, but it did reduce aneurysm rupture rates. On the basis of this work and from analysis of pathological specimens, we know that a bacterial aneurysm results from a septic embolus becoming impacted in a small pial vessel and initiating an [[arteritis]]. This is followed by thrombosis, bacterial multiplication, invasion of the wall, and destruction of the internal elastic lamina and media<ref name="Stehbens">Stehbens W. The pathogenesis of intracranial aneurysms. In: Tindall GT CP, Barrow DL, editor. The Practice of Neurosurgery. Baltimore: Williams and Wilkins; 1996. p. 1941-1952.</ref>. Dilation and rupture can then occur as a result of unchecked hemodynamic stress on the vessel wall<ref name="Stehbens">Stehbens W. The pathogenesis of intracranial aneurysms. In: Tindall GT CP, Barrow DL, editor. The Practice of Neurosurgery. Baltimore: Williams and Wilkins; 1996. p. 1941-1952.</ref>. In clinical studies, bacterial aneurysms can shrink in size with antibiotic treatment, but increase in size and rupture can also occur<ref name="Venkatesh">Venkatesh SK, Phadke RV, Kalode RR, Kumar S, Jain VK. Intracranial infective aneurysms presenting with haemorrhage: an analysis of angiographic findings, management and outcome. Clin Radiol 2000;55(12):946-953.</ref><ref name="Pootrakul">Pootrakul A, Carter LP. Bacterial intracranial aneurysm: importance of sequential angiography. Surg Neurol 1982;17(6):429-431.</ref><ref name="Kovoor">Kovoor JM, Jayakumar PN, Srikanth SG, Sampath S. Intracranial infective aneurysms: angiographic evaluation with treatment. Neurol India 2001;49(3):262-266.</ref>. Subarachnoid hemorrhage from these aneurysms is associated with significant morbidity and mortality. Multiple aneurysms occur in approximately 20% of cases<ref name="Frazee">Frazee JG, Cahan LD, Winter J. Bacterial intracranial aneurysms. J Neurosurg 1980;53(5):633-641.</ref>. | |||
Fungal aneurysms are extremely rare. Hurst et al. identified 15 cases in their recent review of the literature that spanned the years from 1968 to 2001<ref name="Hurst">Hurst RW, Judkins A, Bolger W, Chu A, Loevner LA. Mycotic aneurysm and cerebral infarction resulting from fungal sinusitis: imaging and pathologic correlation. AJNR Am J Neuroradiol 2001;22(5):858-863.</ref>. Unlike bacterial aneurysms, these aneurysms occur more proximally on intracranial vessels. These aneurysms have been found in association with systemic fungal infections and immunosuppression, as well as fungal sinusitis<ref name="Hurst">Hurst RW, Judkins A, Bolger W, Chu A, Loevner LA. Mycotic aneurysm and cerebral infarction resulting from fungal sinusitis: imaging and pathologic correlation. AJNR Am J Neuroradiol 2001;22(5):858-863.</ref>. Like bacterial aneurysms, they can cause SAH and are associated with significant morbidity and mortality. Candidiasis, Aspergillus, and Penicillium are the most common causes of mycotic aneurysm<ref name="Stehbens">Stehbens W. The pathogenesis of intracranial aneurysms. In: Tindall GT CP, Barrow DL, editor. The Practice of Neurosurgery. Baltimore: Williams and Wilkins; 1996. p. 1941-1952.</ref>. | |||
==Traumatic Aneurysms== | |||
Traumatic intracerebral aneurysms occur after various types of head injury. They have been associated with closed head injury as well as penetrating injury. Common locations for these aneurysms are the pericallosal branch of the [[anterior cerebral artery]], the [[posterior cerebral artery]], and the [[middle cerebral artery]]<ref name="Stehbens">Stehbens W. The pathogenesis of intracranial aneurysms. In: Tindall GT CP, Barrow DL, editor. The Practice of Neurosurgery. Baltimore: Williams and Wilkins; 1996. p. 1941-1952.</ref>. Their rupture is associated with a 50% mortality rate. Their presence should be considered when there is an unexplained deterioration in the patient's clinical condition after head injury. The sac of a traumatic aneurysm may have an irregular contour and a neck may be absent<ref name="Weir">Weir B. Intracranial aneurysms. In: Wilkins RH RS, editor. Neurosurgery: McGraw Hill; 1985. p. 1308-1329.</ref>. | |||
==Dissecting Aneurysms== | |||
With modern imaging capability, intracranial dissecting aneurysms are being diagnosed with increasing frequency. Histopathologically, an arterial dissection occurs when a tear occurs in the intima and through the media, allowing blood to collect in the subadventitial space. Blood permeating the [[adventitia]] can cause a [[pseudoaneurysm]] and/ or [[subarachnoid hemorrhage]]. The collected blood can also cause compression of the parent artery, with resulting ischemia and infarction. Occasionally, blood permeates the media and intima in a retrograde fashion and forms a pseudo lumen. If flow is restored promptly, infarction may be avoided. Dissecting aneurysms occur most commonly on the middle cerebral artery, followed by the vertebral artery. When dissecting aneurysms rupture, there is a high incidence of rehemorrhage if the aneurysm is not treated. On the basis of a review of 260 cases, an overall mortality of 26% was found<ref name="Yamaura">Yamaura A. Nontraumatic intracranial arterial dissection: Natural history, diagnosis, and treatment. Contemp Neurosurg 1994;16(5):1-6.</ref>. | |||
==Aneurysms Associated with Arteriovenous Malformations (AVMs)== | |||
''Main article: [[Arteriovenous malformation|Arteriovenous Malformation]]'' | |||
The incidence of intracranial aneurysms is higher in patients with intracranial AVMs than in the general population. This incidence varies from 2.7 to 23% in the literature<ref name="Batjer">Batjer H, Suss RA, Samson D. Intracranial arteriovenous malformations associated with aneurysms. Neurosurgery 1986;18(1):29-35.</ref><ref name="Fisher">Fisher W. Concomitant intracranial aneurysms and arteriovenous malformations. In: Wilkins RH RS, editor. Neurosurgery. New York: McGraw Hill; 1996.</ref>. The quoted rates can be even higher when superselective catheterization is utilized for diagnostic angiography. Four types of aneurysms occur in association with AVMs: | |||
# Unassociated aneurysms: this type of aneurysm occurs on the [[circle of Willis]] in a location that is not associated hemodynamically with the AVM. | |||
# Proximal aneurysm: this type of aneurysm occurs on the proximal vessel (at the [[circle of Willis]]) that feeds the AVM. | |||
# Pedicle aneurysm: these aneurysm occur along AVM arterial feeders. | |||
# Intranidal aneurysms: these aneurysms occur within the AVM nidus (nucleus of the AVM) and are often the source of AVM hemorrhage. | |||
Some authors have argued that since AVMs are congenital, associated aneurysms are also congenital. However, most authors agree that the above aneurysms develop with time from hemodynamic stress (high-flow conditions). Some evidence supports this pathophysiological theory. In a study by Berenstein and colleagues<ref name="Berenstein">Berenstein A, Lasjaunias P. Surgical Neuroangiography. New York: Springer-Verlag; 1999, p. 1-88.</ref>, increasing age was positively correlated with the presence of an AVM- associated aneurysm: the combination was present in 8% of patients under 25 years, 24% of patients aged 25 to 49 years, and 37% of patients over the age of 50 years. Another finding that implicates high flow is the observation that aneurysms are more likely to be found in larger AVMs with high flow<ref name="Kondziolka">Kondziolka D, Nixon BJ, Lasjaunias P, Tucker WS, TerBrugge K, Spiegel SM. Cerebral arteriovenous malformations with associated arterial aneurysms: hemodynamic and therapeutic considerations. Can J Neurol Sci 1988;15(2):130-134.</ref> <ref name="Miyasaka">Miyasaka K, Wolpert SM, Prager RJ. The association of cerebral aneurysms, infundibula, and intracranial arteriovenous malformations. Stroke 1982;13(2):196-203.</ref>. It is believed that high flow and possibly turbulent flow predispose vessels to aneurysm formation. Of the subtypes of aneurysms listed above, all occur with increased frequency in patients with AVMs, with the exception of the fourth type, which occurs with the same frequency in the general population. As mentioned, these aneurysms are not associated hemodynamically with the AVM. | |||
The natural history of aneurysms associated with AVMs has not been clearly deciphered. Recent reports suggest that intranidal aneurysms may increase the hemorrhage risk of an AVM<ref name="Redekop">Redekop G, TerBrugge K, Montanera W, Willinsky R. Arterial aneurysms associated with cerebral arteriovenous malformations: classification, incidence, and risk of hemorrhage. J Neurosurg 1998;89(4):539-546.</ref>. Angiographic data on intranidal aneurysms should be viewed with caution since pseudoaneurysms in the nidus of ruptured AVMs can assume the appearance of an intranidal aneurysm. | |||
Misinterpretation can lead to the attribution of an artificially elevated risk of AVM hemorrhage associated with the presence of an intranidal aneurysm. The rate of hemorrhage of other aneurysms associated with AVMs has not been clearly defined. It is believed that the fourth type of associated aneurysm, those located on vessels unrelated to AVM feeders, have a hemorrhage rate similar to that associated with berry aneurysms in patients without AVMs. Anecdotal evidence suggests that AVM resection may pose a significant risk for rupture of proximal and pedicle aneurysms<ref name="Batjer">Batjer H, Suss RA, Samson D. Intracranial arteriovenous malformations associated with aneurysms. Neurosurgery 1986;18(1):29-35.</ref>. Only theoretical concerns have been raised about any acute hemorrhage risk of unrelated aneurysms in the face of AVM resection. AVM resection has been associated with a decrease in size or even disappearance of pedicle aneurysms when they are not treated at the time of AVM resection. This widely held belief has been recently called into question by a report on a large series of patients with AVMs and associated aneurysms<ref name="Redekop">Redekop G, TerBrugge K, Montanera W, Willinsky R. Arterial aneurysms associated with cerebral arteriovenous malformations: classification, incidence, and risk of hemorrhage. J Neurosurg 1998;89(4):539-546.</ref>. This report asserts that although this phenomenon does occur it does not do so consistently. | |||
==Neoplastic Aneurysms== | |||
These aneurysms result from tumor invasion of the vessel wall followed by tumor embolism<ref name="Burton">Burton C, Johnston J. Multiple cerebral aneurysms and cardiac myxoma. N Engl J Med 1970;282(1):35-36.</ref>. They usually occur as a result of a [[myxoma in the left atrium]]. The [[middle cerebral artery]] is most commonly involved. | |||
==Miliary Aneurysms of Charcot and Bouchard== | |||
''Main article: [[Charcot-Bouchard aneurysm|Charcot-Bouchard Aneurysm]]'' | |||
These aneurysms are small (300 to 1100 micrometers) aneurysms that occur on small branches of cerebral arteries in the basal ganglia, thalamus, pons, cerebellum, and cerebral cortex<ref name="Stehbens">Stehbens W. The pathogenesis of intracranial aneurysms. In: Tindall GT CP, Barrow DL, editor. The Practice of Neurosurgery. Baltimore: Williams and Wilkins; 1996. p. 1941-1952.</ref><ref name="Fisher 2">Fisher C. Cerebral miliary aneurysms in hypertension. Am J Pathol 1971;66:313-330.</ref>. They are thought to be associated with hypertension and are believed to be the cause of many hypertensive cerebral hemorrhages. | |||
==Fusiform Aneurysms== | |||
Fusiform aneurysms usually occur in large severely atherosclerotic and tortuous vessels. These associated findings are believed to play important roles in the pathophysiology of these lesions in humans. In a rabbit model, chronic bending of the artery produces transverse tears in the internal elastic lamina<ref name=""Stehbens2">Stehbens WE. Flow in glass models of arterial bifurcations and berry aneurysms at low Reynolds numbers. Q J Exp Physiol Cogn Med Sci 1975;60(3):181-192.</ref>. These tears affect other layers of the vessel wall and ultimately lead to vessel atrophy and weakness against hemodynamic stress. These aneurysms can cause mass effect or hemorrhage. | |||
==Intracranial AVMs== | |||
AVMs are congenital vascular malformations that appear between the fourth and eighth weeks of embryonic development<ref name="Fisher">Fisher W. Concomitant intracranial aneurysms and arteriovenous malformations. In: Wilkins RH RS, editor. Neurosurgery. New York: McGraw Hill; 1996.</ref>. At this stage, the primitive vascular network forms and differentiates into arteries, veins, and capillaries. Histologically, AVMs are masses of abnormal arteries and veins without a true capillary bed. The nidus of the AVM consists of tangled large vessels that lack an elastic layer in their walls. In compact AVMs, very little brain tissue resides within the nidus; and this tissue is usually gliotic. Occasionally, AVM tissue can be diffuse; and normal tissue can be found in its midst. Evidence suggests that AVMs can grow with time<ref name="Fisher">Fisher W. Concomitant intracranial aneurysms and arteriovenous malformations. In: Wilkins RH RS, editor. Neurosurgery. New York: McGraw Hill; 1996.</ref>. AVMs can cause harm by any or a combination of the following manifestations: | |||
* [[Rupture]] | |||
* Rupture of associated aneurysms | |||
* [[Seizure]]s | |||
* [[Ischemia]] from vascular steal | |||
The mechanism by which AVMs rupture is not clear. AVMs rupture at a rate of 2 to 4% per year. Vascular steal occurs when blood flow to the hemisphere preferentially goes through a high-flow AVM due to its low resistance circuit compared with the normal capillary bed. This results in ischemia in areas near the AVM. Ischemia from vascular steal is seen with large, high-flow AVMs. Histologically, vascular steal can be seen as gliosis, necrosis, and calcification. Clinically, steal can manifest as seizures, ischemic events, or infarction<ref name="Ondra">Ondra SL, Troupp H, George ED, Schwab K. The natural history of symptomatic arteriovenous malformations of the brain: a 24-year follow-up assessment. J Neurosurg 1990; 73(3): 387-391.</ref><ref name="Kondziolka">Kondziolka D, McLaughlin MR, Kestle JR. Simple risk predictions for arteriovenous malformation hemorrhage. Neurosurgery 1995;37(5):851-855.</ref>. | |||
Research over the past decade has been devoted to elucidating the role of angiogenic factors and their receptors in vascular malformation pathology<ref name="Uranishi">Uranishi R, Baev NI, Ng PY, Kim JH, Awad IA. Expression of endothelial cell angiogenesis receptors in human cerebrovascular malformations. Neurosurgery 2001;48(2):359-368.</ref><ref name="Wong 2">Wong JH, Awad IA, Kim JH. Ultrastructural pathological features of cerebrovascular malformations: a preliminary report. Neurosurgery 2000;46(6):1454-1459.</ref><ref name="Rothbart">Rothbart D, Awad IA, Lee J, Kim J, Harbaugh R, Criscuolo GR. Expression of angiogenic factors and structural proteins in central nervous system vascular malformations. Neurosurgery 1996;38(5):915-925.</ref>. These studies have postulated that angiogenesis plays a role in AVM pathophysiology. It has been shown, for example, that vascular endothelial growth factor (VEGF) is expressed in the subendothelial layer of AVMs<ref name="Rothbart">Rothbart D, Awad IA, Lee J, Kim J, Harbaugh R, Criscuolo GR. Expression of angiogenic factors and structural proteins in central nervous system vascular malformations. Neurosurgery 1996;38(5):915-925.</ref>. Understanding this biology may allow for modification of lesion behavior in the near future. | |||
===Spetzler-Martin Grading System=== | |||
<table border="1" cellspacing="0" cellpadding="3"><tr> | |||
<th colspan="2">Size</th> | |||
<th colspan="2">Eloquence of Adjacent Brain<font size="2"></font></th> | |||
<th colspan="2">Venous Drainage<font size="2"></font></th> | |||
</tr><tr><td>Small (<3 cm)</td><td align="center">1</td><td>Noneloquent</td><td align="center">0</td><td>Superficial only </td><td align="center">0</td></tr><tr><td>Medium (3-6 cm)</td><td align="center">2</td><td>Eloquent</td><td align="center">1</td><td>Deep component </td><td align="center">1</td></tr><tr><td>Large (>6 cm)</td><td align="center">3</td><td colspan="2" align="center">…</td><td colspan="2" align="center">…</td></tr></table> | |||
*Size: Measure the largest diameter of the nidus of the lesion on angiography.<br> | |||
*Eloquence: Eloquent areas include sensorimotor, language, visual, thalamus, hypothalamus, internal capsule, brain stem, cerebellar peduncles, and deep cerebellar nuclei.<br> | |||
*Venous drainage: The lesion is considered superficial only if all drainage is via the cortical drainage system. | |||
==Intracranial AVFs== | |||
Parenchymal AVFs of the brain consist of an immediate arteriovenous transition with no intervening nidus. These lesions are extremely rare; hence their pathophysiology is not well understood. Both embryological and traumatic etiologies are conceivable. Patients with these lesions present with headache, seizures, hemorrhage, or heart failure<ref name="Tomlinson">Tomlinson FH, Rufenacht DA, Sundt TM, Jr., Nichols DA, Fode NC. Arteriovenous fistulas of the brain and the spinal cord. J Neurosurg 1993;79(1):16-27.</ref><ref name="Bendok 2">Bendok BR, Getch CC, Frederiksen J, Batjer HH. Resection of a large arteriovenous fistula of the brain using low-flow deep hypothermic cardiopulmonary bypass: technical case report. Neurosurgery 1999;44(4):888-891.</ref>. When these lesions are complex, treatment can be technically difficult due to extremely high flow<ref name="Tomlinson">Tomlinson FH, Rufenacht DA, Sundt TM, Jr., Nichols DA, Fode NC. Arteriovenous fistulas of the brain and the spinal cord. J Neurosurg 1993;79(1):16-27.</ref><ref name="Bendok 2">Bendok BR, Getch CC, Frederiksen J, Batjer HH. Resection of a large arteriovenous fistula of the brain using low-flow deep hypothermic cardiopulmonary bypass: technical case report. Neurosurgery 1999;44(4):888-891.</ref>. Dural AVFs are pathological vascular channels located within the substance of the dura and usually involve the walls of a dural sinus or an adjacent cortical vein<ref name="Malek">Malek AM, Halbach VV, Higashida RT, Phatouros CC, Meyers PM, Dowd CF. Treatment of dural arteriovenous malformations and fistulas. Neurosurg Clin N Am 2000;11(1):147-166.</ref>. These fistulas most commonly involve the transverse, sigmoid, and cavernous sinuses. Rarely, other sinuses, such as the superior sagittal sinus and the petrosal sinus, can also be involved. | |||
The pathogenesis of dural AVF is believed to initiate with sinus thrombosis. Recanalization of the sinus then occurs through enlargement of microfistulas in the sinus wall. The initial sinus thrombosis leads to venous hypertension that if severe can result in reversal of flow in the sinus, with outflow being directed through cortical veins that become arterialized. This change in flow changes a fistula from a benign lesion to one that poses a risk for intracerebral hemorrhage. Interesting work has begun to link angiogenic growth factors, such as basic fibroblastic growth factor (b-FGF), with the development of dural AVFs<ref name="Malek">Malek AM, Halbach VV, Higashida RT, Phatouros CC, Meyers PM, Dowd CF. Treatment of dural arteriovenous malformations and fistulas. Neurosurg Clin N Am 2000;11(1):147-166.</ref>. | |||
Evidence suggests that hypoxia induced by venous congestion and elevated shear stress to which endothelium in the fistula is exposed can increase the production of angiogenic factors that can lead to the formation of new vessels that connect with the fistula. | |||
==Conclusions== | |||
It is our hope that this chapter will serve as a review on the pathophysiology of aneurysms, AVMs, and AVFs for practitioners and students of the neurointerventional field. A clear understanding of the pathophysiology of these vascular lesions is an important prerequisite to sound clinical decision-making. Education in this area can only be partially achieved with a chapter and must be constantly pursued by the practitioners of our young field. | |||
Although our knowledge regarding the pathophysiology of these lesions has expanded dramatically over the past 80 years, we are still only experiencing the dawn of our enlightenment. The molecular mechanisms by which these lesions arise and produce symptoms have just begun to be understood. Understanding these mechanisms as well as developing safer and more effective treatments are two key areas for research for the next decade. | |||
==Diagnosis== | |||
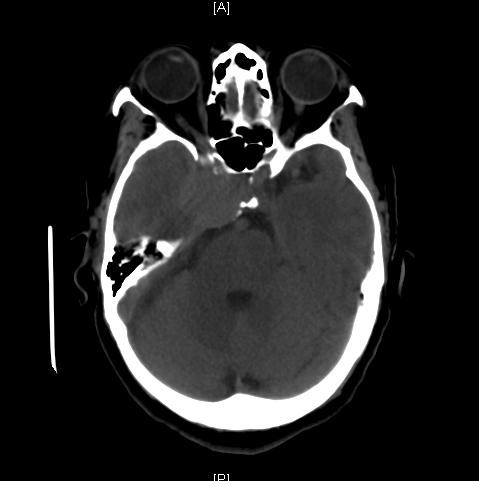
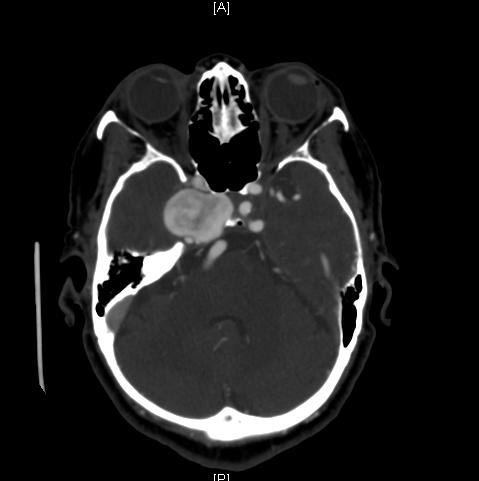
{{ | ===A Large Basilar Artery Aneurysm=== | ||
[http://www.radswiki.net Copyleft Images Courtesy of RadsWiki] | |||
<gallery> | |||
Image:Basilar-artery-aneurysm-01.jpg|CT: A large basilar artery aneurysm | |||
Image:Basilar-artery-aneurysm-02.jpg|CT: A large basilar artery aneurysm | |||
Image:Basilar-artery-aneurysm-03.jpg|CT: A large basilar artery aneurysm | |||
Image:Basilar-artery-aneurysm-04.jpg|CT: A large basilar artery aneurysm | |||
Image:Basilar-artery-aneurysm-05.jpg|Angiography: A large basilar artery aneurysm | |||
Image:Basilar-artery-aneurysm-06.jpg|Angiography: A large basilar artery aneurysm | |||
</gallery> | |||
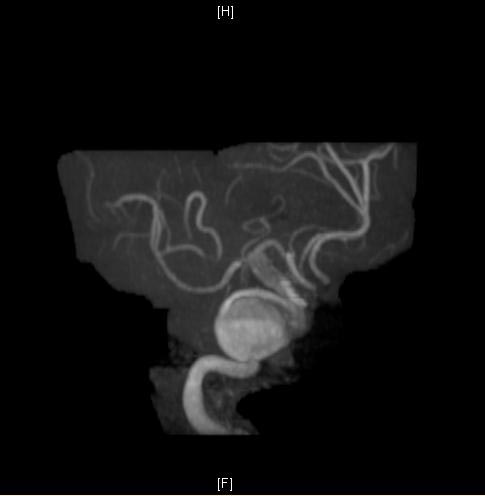
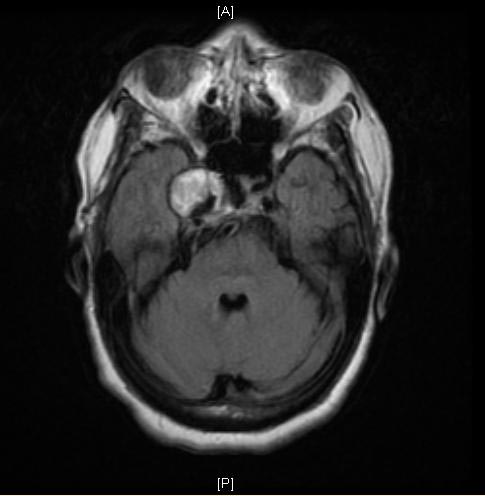
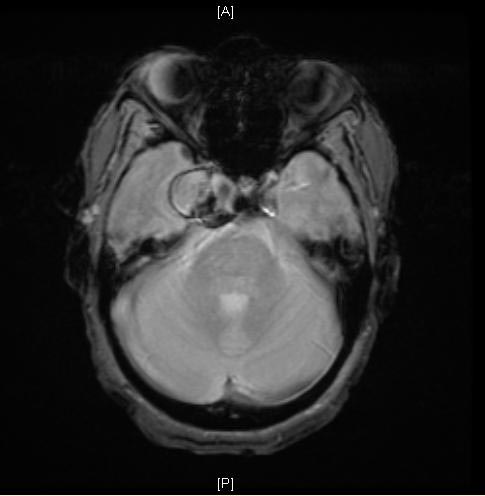
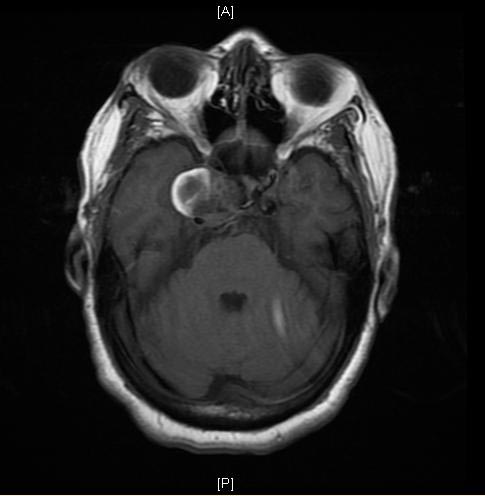
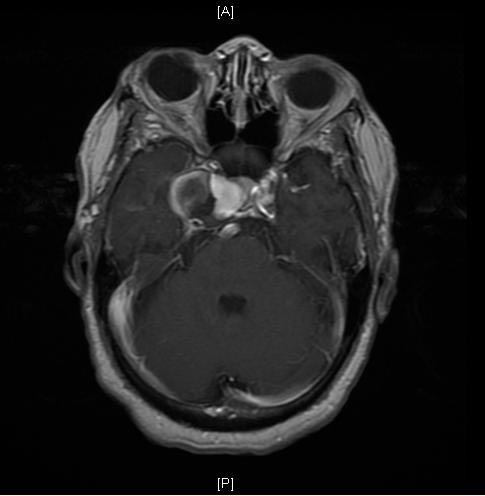
===A Large Cavernous Sinus Aneurysm=== | |||
[http://www.radswiki.net Copyleft Images courtesy of RadsWiki] | |||
<gallery> | |||
Image:Cavernous-sinus-aneurysm-001.jpg|MRI: A large cavernous sinus aneurysm | |||
Image:Cavernous-sinus-aneurysm-002.jpg|MRI: A large cavernous sinus aneurysm | |||
Image:Cavernous-sinus-aneurysm-003.jpg|MRI: A large cavernous sinus aneurysm | |||
Image:Cavernous-sinus-aneurysm-004.jpg|MRI: A large cavernous sinus aneurysm | |||
Image:Cavernous-sinus-aneurysm-005.jpg|MRI: A large cavernous sinus aneurysm | |||
</gallery> | |||
<gallery> | |||
Image:Cavernous-sinus-aneurysm-006.jpg|MRI: A large cavernous sinus aneurysm | |||
Image:Cavernous-sinus-aneurysm-007.jpg|MRI: A large cavernous sinus aneurysm | |||
Image:Cavernous-sinus-aneurysm-008.jpg|MRI: A large cavernous sinus aneurysm | |||
Image:Cavernous-sinus-aneurysm-009.jpg|MRI: A large cavernous sinus aneurysm | |||
</gallery> | |||
===Cerebral Vascular Malformations=== | |||
[http://www.radswiki.net Copyleft Images courtesy of RadsWiki] | |||
<gallery> | |||
Image:Arteriovenous malformation 1.jpg|[[Arteriovenous malformation]] | |||
Image:Cavernous-malformation-02.jpg|[[Cavernous malformation]] | |||
Image:Developmental-venous-anomaly-003.jpg|[[Developmental venous anomaly]] | |||
</gallery> | |||
==Differentiating intracranial aneurysm from Other Diseases== | |||
Intracranial aneurysmmust be differentiated from other diseases that cause [[seizure]], [[visual disturbance]], and [[constitutional]] [[symptoms]], such as: | |||
* [[Oligodendroglioma]] | |||
* [[Meningioma]] | |||
* [[Astrocytoma]] | |||
* [[Pituitary adenoma]] | |||
* [[Schwannoma]] | |||
* [[Primary central nervous system lymphoma|primary CNS lymphoma]] | |||
* [[Medulloblastoma]] | |||
* [[Ependymoma]] | |||
* [[Craniopharyngioma]] | |||
* [[Pinealoma]] | |||
* [[Arteriovenous malformation|AV malformation]] | |||
* [[Hemangioblastoma]] | |||
* [[Bacterial]] [[brain]] [[abscess]] | |||
* [[Tuberculosis]] | |||
* [[Toxoplasmosis]] | |||
* [[Hydatid cyst]] | |||
* [[CNS]] [[cryptococcosis]] | |||
* [[CNS]] [[aspergillosis]] | |||
* [[Brain metastasis]] | |||
For more information [[Astrocytoma differential diagnosis|click here]]. | |||
==Videos: Histopathology== | |||
===Histopathology: Arteriovenous Malformation (Pons)=== | |||
{{#ev:youtube|YcOqcu1xmFc}} | |||
===Histopathology: Arteriovenous Malformation (Brain)=== | |||
{{#ev:youtube|mZyNihzHysk}} | |||
==References== | |||
{{Reflist|2}} | |||
==Related Chapters == | |||
* [[Cerebral aneurysm|Cerebral Aneurysm]] | |||
* [[Arteriovenous malformation|Arteriovenous Malformation]] | |||
* [[Arteriovenous fistula|Arteriovenous Fistula]] | |||
* [[Aneurysm]] | |||
* [[Charcot-Bouchard aneurysm|Charcot-Bouchard Aneurysm]] | |||
* [[Intracranial berry aneurysm|Berry Aneurysm]] | |||
* [[Stroke]] | |||
* [[Subarachnoid hemorrhage|Subarachnoid Hemorrhage]] | |||
* [[International Subarachnoid Aneurysm Trial]] | |||
[[Category:Neurology]] | [[Category:Neurology]] | ||
[[Category:Neurosurgery]] | |||
[[Category:Disease]] | |||
[[Category:Mature chapter]] | |||
[[Category:Cardiology]] | [[Category:Cardiology]] | ||
[[Category:Emergency medicine]] | |||
{{WH}} | |||
{{ | {{WS}} | ||
{{ | |||
Latest revision as of 16:38, 31 January 2019
| Intracranial aneurysms | |
 | |
|---|---|
| Berry aneurysm in anterior cerebral artery |
For patient information, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2], Fahimeh Shojaei, M.D.
Synonyms and keywords: Anterior cerebral artery aneurysm; anterior communicating artery aneurysm; aneurysm of anterior communicating artery; intracranial aneurysm; middle cerebral artery aneurysm; posterior cerebral artery aneurysm; posterior communicating artery aneurysm; brain aneurysm; giant intracranial aneurysm; aneurysm in the brain
Overview
The catastrophic potential of intracranial aneurysms, arteriovenous malformations (AVMs), and arteriovenous fistulas (AVFs) and the complexity of their pathogenesis have made them the subject of intense interest and study over the past 80 years. Advances in the ability to treat these lesions have been paralleled by rigorous research on their pathophysiology. An increase in the longevity of the population over the past century and improvements in imaging techniques contribute to more frequent encounters with these lesions by neurosurgeons and interventionists. Despite numerous clinical and laboratory research projects studying the pathophysiology of these lesions, much remains to be learned. In this chapter, we will discuss the pathophysiology of various types of intracranial aneurysms, as well as AVMs and AVFs.
Berry Aneurysms
Main article: Berry Aneurysm
Berry aneurysms arise at vessel bifurcations or curves. These aneurysms occur mostly between the ages of 40 and 70 years. The pathogenesis of berry aneurysms is multifactorial. Compelling evidence suggests that hemodynamic factors as well as degenerative histological changes in the parent vessel wall contribute to aneurysm formation. Early in the process of berry aneurysm formation, destruction and eventual loss of the media occur[1]. The internal elastic layer becomes disrupted and is eventually lost.
The mechanisms by which these changes occur are not well understood but have been attributed in part to atherosclerotic changes. This weakening in the vessel wall sets the stage for hemodynamic forces to cause saccular dilation[2]. Reduced peripheral resistance in the intracranial circulation, along with more rapid blood flow, may be associated with an augmented pulse pressure, which can lead to saccular dilation[1]. Recent studies have demonstrated that hemodynamic stress in vascular walls can result in alterations in extracellular matrix organization[3]. Turbulent flow in aneurysmal sacs damages the endothelium and results in laminar necrosis of the wall and expansion of the aneurysm. If a small aneurysm does not rupture, partial healing occurs through mural thrombus formation followed by organization of the thrombus with scarring of the wall, invasion of fibroblasts, collagen formation, platelet aggregation, and deposition of fibrous material. Repeat hemorrhages can occur in the wall, leading to repetitive cycles of abnormal healing and aneurysm growth. Giant aneurysms are believed to form by these mechanisms[4].
Several risk factors and associated conditions have been linked with intracranial aneurysm growth and rupture. Smoking has been associated with larger berry aneurysm size and multiple aneurysms[5] [6] [7]. Alcohol abuse has been associated with aneurysm rupture[7]. The role of hypertension in aneurysm formation has been controversial in the literature. Hypertension as a direct cause of aneurysms has never been established; however, it is believed that hypertension may exacerbate a rupture when it occurs and may contribute to aneurysm growth. Several conditions have been associated with a greater propensity for berry aneurysms. These conditions include coarctation of the aorta, polycystic kidney disease, and various connective tissue disorders such as Ehlers-Danlos syndrome[1].
Ninety percent of symptomatic berry aneurysms occur in the anterior circulation and 10% in the posterior circulation. In a prospective autopsy study, the mean size of ruptured aneurysms was 8.6 mm and of unruptured was 4.7 mm[8]. Eighty percent of symptomatic aneurysms are under 12 mm in size[9]. Multiple aneurysms occur in approximately 15% of cases[10]. Most aneurysm ruptures occur between the fourth and seventh decades[9]. Saccular aneurysms become symptomatic owing to rupture, mass effect, or embolic events. The precise pathophysiology of rupture is not yet clearly understood, but it is believed that structural and hemodynamic factors play a role. The pathophysiology of aneurysmal SAH is beyond the scope of this chapter. Subarachnoid hemorrhage is associated with severe morbidity and mortality. Vasospasm, stroke, hydrocephalus, and seizures are some of the neurological consequences. Overall, approximately 50% of patients who experience SAH die within the first month; and approximately 30% of survivors have moderate to severe disability[11][12][13].
Inflammatory Aneurysms
Main article: Mycotic Aneurysm
There are two types of inflammatory aneurysms:
- Bacterial aneurysms (which are often referred to erroneously as mycotic)
- Fungal or true mycotic aneurysms
A review by Frazee et al.[14] summarized the reported cases of bacterial aneurysms in the literature between 1954 and 1980. The age of the patients ranged from 7 months to 78 years (average age, 30 years). Most patients had a history of either congenital heart disease, recent dental work, pulmonary infection, or carious teeth. Historically, patients with bacterial endocarditis were believed to have a risk of 4 to 15% of developing an intracranial aneurysm[15]. Improvements in treatment over the past 2 decades are most likely responsible for the significant reduction in these numbers today. Streptococcus is the most common cause of bacterial aneurysms, followed by Staphylococcus. Other less commonly reported infecting organisms include Neisseria, Enterococcus, and Pseudomonas[1]. In addition to their association with endocarditis, bacterial aneurysms have been reported in conjunction with meningitis and cavernous sinus thrombophlebitis, as well as following cardiac valvular surgery and intravenous drug abuse. Inflammatory aneurysms typically occur on distal cerebral vessels. This fact is a distinguishing feature from the more common berry aneurysms, which are found proximally on the circle of Willis.
Work on a canine model by Molinari et al. suggests that the pathophysiology of inflammatory aneurysms relates to the lodging of an infected embolus in a distal cerebral vessel[16]. This group lodged bacterial-laden clots in the distal cerebral vasculature, which caused aneurysm formation. In their model, aneurysms formed within 3 days of the embolus being lodged. In this model, antibiotic administration did not prevent aneurysm formation, but it did reduce aneurysm rupture rates. On the basis of this work and from analysis of pathological specimens, we know that a bacterial aneurysm results from a septic embolus becoming impacted in a small pial vessel and initiating an arteritis. This is followed by thrombosis, bacterial multiplication, invasion of the wall, and destruction of the internal elastic lamina and media[1]. Dilation and rupture can then occur as a result of unchecked hemodynamic stress on the vessel wall[1]. In clinical studies, bacterial aneurysms can shrink in size with antibiotic treatment, but increase in size and rupture can also occur[17][18][19]. Subarachnoid hemorrhage from these aneurysms is associated with significant morbidity and mortality. Multiple aneurysms occur in approximately 20% of cases[14].
Fungal aneurysms are extremely rare. Hurst et al. identified 15 cases in their recent review of the literature that spanned the years from 1968 to 2001[20]. Unlike bacterial aneurysms, these aneurysms occur more proximally on intracranial vessels. These aneurysms have been found in association with systemic fungal infections and immunosuppression, as well as fungal sinusitis[20]. Like bacterial aneurysms, they can cause SAH and are associated with significant morbidity and mortality. Candidiasis, Aspergillus, and Penicillium are the most common causes of mycotic aneurysm[1].
Traumatic Aneurysms
Traumatic intracerebral aneurysms occur after various types of head injury. They have been associated with closed head injury as well as penetrating injury. Common locations for these aneurysms are the pericallosal branch of the anterior cerebral artery, the posterior cerebral artery, and the middle cerebral artery[1]. Their rupture is associated with a 50% mortality rate. Their presence should be considered when there is an unexplained deterioration in the patient's clinical condition after head injury. The sac of a traumatic aneurysm may have an irregular contour and a neck may be absent[9].
Dissecting Aneurysms
With modern imaging capability, intracranial dissecting aneurysms are being diagnosed with increasing frequency. Histopathologically, an arterial dissection occurs when a tear occurs in the intima and through the media, allowing blood to collect in the subadventitial space. Blood permeating the adventitia can cause a pseudoaneurysm and/ or subarachnoid hemorrhage. The collected blood can also cause compression of the parent artery, with resulting ischemia and infarction. Occasionally, blood permeates the media and intima in a retrograde fashion and forms a pseudo lumen. If flow is restored promptly, infarction may be avoided. Dissecting aneurysms occur most commonly on the middle cerebral artery, followed by the vertebral artery. When dissecting aneurysms rupture, there is a high incidence of rehemorrhage if the aneurysm is not treated. On the basis of a review of 260 cases, an overall mortality of 26% was found[21].
Aneurysms Associated with Arteriovenous Malformations (AVMs)
Main article: Arteriovenous Malformation
The incidence of intracranial aneurysms is higher in patients with intracranial AVMs than in the general population. This incidence varies from 2.7 to 23% in the literature[22][23]. The quoted rates can be even higher when superselective catheterization is utilized for diagnostic angiography. Four types of aneurysms occur in association with AVMs:
- Unassociated aneurysms: this type of aneurysm occurs on the circle of Willis in a location that is not associated hemodynamically with the AVM.
- Proximal aneurysm: this type of aneurysm occurs on the proximal vessel (at the circle of Willis) that feeds the AVM.
- Pedicle aneurysm: these aneurysm occur along AVM arterial feeders.
- Intranidal aneurysms: these aneurysms occur within the AVM nidus (nucleus of the AVM) and are often the source of AVM hemorrhage.
Some authors have argued that since AVMs are congenital, associated aneurysms are also congenital. However, most authors agree that the above aneurysms develop with time from hemodynamic stress (high-flow conditions). Some evidence supports this pathophysiological theory. In a study by Berenstein and colleagues[24], increasing age was positively correlated with the presence of an AVM- associated aneurysm: the combination was present in 8% of patients under 25 years, 24% of patients aged 25 to 49 years, and 37% of patients over the age of 50 years. Another finding that implicates high flow is the observation that aneurysms are more likely to be found in larger AVMs with high flow[25] [26]. It is believed that high flow and possibly turbulent flow predispose vessels to aneurysm formation. Of the subtypes of aneurysms listed above, all occur with increased frequency in patients with AVMs, with the exception of the fourth type, which occurs with the same frequency in the general population. As mentioned, these aneurysms are not associated hemodynamically with the AVM.
The natural history of aneurysms associated with AVMs has not been clearly deciphered. Recent reports suggest that intranidal aneurysms may increase the hemorrhage risk of an AVM[27]. Angiographic data on intranidal aneurysms should be viewed with caution since pseudoaneurysms in the nidus of ruptured AVMs can assume the appearance of an intranidal aneurysm.
Misinterpretation can lead to the attribution of an artificially elevated risk of AVM hemorrhage associated with the presence of an intranidal aneurysm. The rate of hemorrhage of other aneurysms associated with AVMs has not been clearly defined. It is believed that the fourth type of associated aneurysm, those located on vessels unrelated to AVM feeders, have a hemorrhage rate similar to that associated with berry aneurysms in patients without AVMs. Anecdotal evidence suggests that AVM resection may pose a significant risk for rupture of proximal and pedicle aneurysms[22]. Only theoretical concerns have been raised about any acute hemorrhage risk of unrelated aneurysms in the face of AVM resection. AVM resection has been associated with a decrease in size or even disappearance of pedicle aneurysms when they are not treated at the time of AVM resection. This widely held belief has been recently called into question by a report on a large series of patients with AVMs and associated aneurysms[27]. This report asserts that although this phenomenon does occur it does not do so consistently.
Neoplastic Aneurysms
These aneurysms result from tumor invasion of the vessel wall followed by tumor embolism[28]. They usually occur as a result of a myxoma in the left atrium. The middle cerebral artery is most commonly involved.
Miliary Aneurysms of Charcot and Bouchard
Main article: Charcot-Bouchard Aneurysm
These aneurysms are small (300 to 1100 micrometers) aneurysms that occur on small branches of cerebral arteries in the basal ganglia, thalamus, pons, cerebellum, and cerebral cortex[1][29]. They are thought to be associated with hypertension and are believed to be the cause of many hypertensive cerebral hemorrhages.
Fusiform Aneurysms
Fusiform aneurysms usually occur in large severely atherosclerotic and tortuous vessels. These associated findings are believed to play important roles in the pathophysiology of these lesions in humans. In a rabbit model, chronic bending of the artery produces transverse tears in the internal elastic lamina[30]. These tears affect other layers of the vessel wall and ultimately lead to vessel atrophy and weakness against hemodynamic stress. These aneurysms can cause mass effect or hemorrhage.
Intracranial AVMs
AVMs are congenital vascular malformations that appear between the fourth and eighth weeks of embryonic development[23]. At this stage, the primitive vascular network forms and differentiates into arteries, veins, and capillaries. Histologically, AVMs are masses of abnormal arteries and veins without a true capillary bed. The nidus of the AVM consists of tangled large vessels that lack an elastic layer in their walls. In compact AVMs, very little brain tissue resides within the nidus; and this tissue is usually gliotic. Occasionally, AVM tissue can be diffuse; and normal tissue can be found in its midst. Evidence suggests that AVMs can grow with time[23]. AVMs can cause harm by any or a combination of the following manifestations:
The mechanism by which AVMs rupture is not clear. AVMs rupture at a rate of 2 to 4% per year. Vascular steal occurs when blood flow to the hemisphere preferentially goes through a high-flow AVM due to its low resistance circuit compared with the normal capillary bed. This results in ischemia in areas near the AVM. Ischemia from vascular steal is seen with large, high-flow AVMs. Histologically, vascular steal can be seen as gliosis, necrosis, and calcification. Clinically, steal can manifest as seizures, ischemic events, or infarction[31][25].
Research over the past decade has been devoted to elucidating the role of angiogenic factors and their receptors in vascular malformation pathology[32][33][34]. These studies have postulated that angiogenesis plays a role in AVM pathophysiology. It has been shown, for example, that vascular endothelial growth factor (VEGF) is expressed in the subendothelial layer of AVMs[34]. Understanding this biology may allow for modification of lesion behavior in the near future.
Spetzler-Martin Grading System
| Size | Eloquence of Adjacent Brain | Venous Drainage | |||
|---|---|---|---|---|---|
| Small (<3 cm) | 1 | Noneloquent | 0 | Superficial only | 0 |
| Medium (3-6 cm) | 2 | Eloquent | 1 | Deep component | 1 |
| Large (>6 cm) | 3 | … | … | ||
- Size: Measure the largest diameter of the nidus of the lesion on angiography.
- Eloquence: Eloquent areas include sensorimotor, language, visual, thalamus, hypothalamus, internal capsule, brain stem, cerebellar peduncles, and deep cerebellar nuclei.
- Venous drainage: The lesion is considered superficial only if all drainage is via the cortical drainage system.
Intracranial AVFs
Parenchymal AVFs of the brain consist of an immediate arteriovenous transition with no intervening nidus. These lesions are extremely rare; hence their pathophysiology is not well understood. Both embryological and traumatic etiologies are conceivable. Patients with these lesions present with headache, seizures, hemorrhage, or heart failure[35][36]. When these lesions are complex, treatment can be technically difficult due to extremely high flow[35][36]. Dural AVFs are pathological vascular channels located within the substance of the dura and usually involve the walls of a dural sinus or an adjacent cortical vein[37]. These fistulas most commonly involve the transverse, sigmoid, and cavernous sinuses. Rarely, other sinuses, such as the superior sagittal sinus and the petrosal sinus, can also be involved.
The pathogenesis of dural AVF is believed to initiate with sinus thrombosis. Recanalization of the sinus then occurs through enlargement of microfistulas in the sinus wall. The initial sinus thrombosis leads to venous hypertension that if severe can result in reversal of flow in the sinus, with outflow being directed through cortical veins that become arterialized. This change in flow changes a fistula from a benign lesion to one that poses a risk for intracerebral hemorrhage. Interesting work has begun to link angiogenic growth factors, such as basic fibroblastic growth factor (b-FGF), with the development of dural AVFs[37].
Evidence suggests that hypoxia induced by venous congestion and elevated shear stress to which endothelium in the fistula is exposed can increase the production of angiogenic factors that can lead to the formation of new vessels that connect with the fistula.
Conclusions
It is our hope that this chapter will serve as a review on the pathophysiology of aneurysms, AVMs, and AVFs for practitioners and students of the neurointerventional field. A clear understanding of the pathophysiology of these vascular lesions is an important prerequisite to sound clinical decision-making. Education in this area can only be partially achieved with a chapter and must be constantly pursued by the practitioners of our young field.
Although our knowledge regarding the pathophysiology of these lesions has expanded dramatically over the past 80 years, we are still only experiencing the dawn of our enlightenment. The molecular mechanisms by which these lesions arise and produce symptoms have just begun to be understood. Understanding these mechanisms as well as developing safer and more effective treatments are two key areas for research for the next decade.
Diagnosis
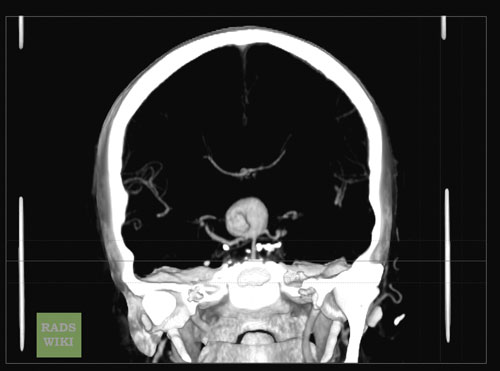
A Large Basilar Artery Aneurysm
Copyleft Images Courtesy of RadsWiki
-

CT: A large basilar artery aneurysm
-

CT: A large basilar artery aneurysm
-

CT: A large basilar artery aneurysm
-
CT: A large basilar artery aneurysm
-
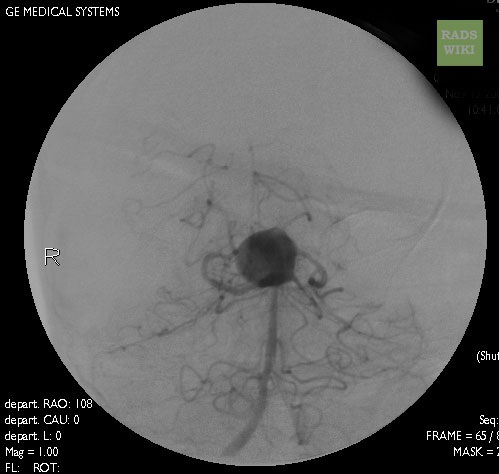
Angiography: A large basilar artery aneurysm
-
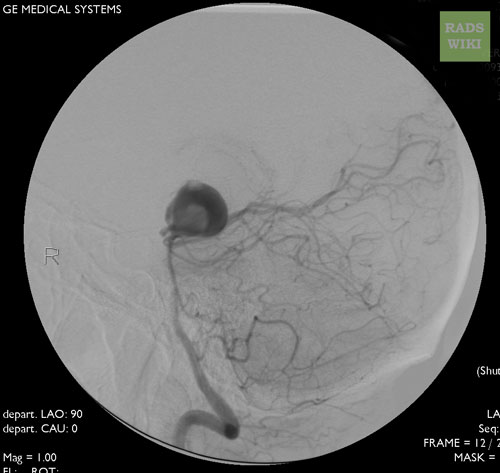
Angiography: A large basilar artery aneurysm






A Large Cavernous Sinus Aneurysm
Copyleft Images courtesy of RadsWiki
-
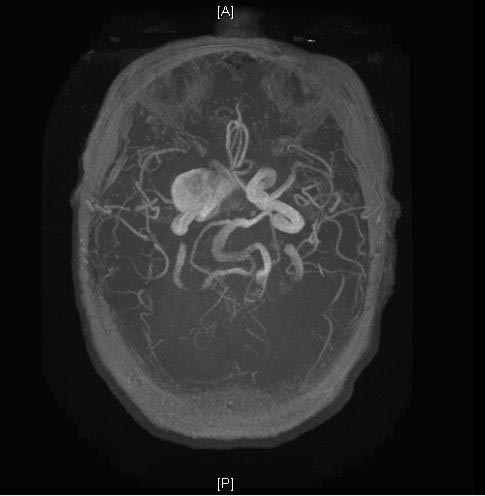
MRI: A large cavernous sinus aneurysm
-
MRI: A large cavernous sinus aneurysm
-

MRI: A large cavernous sinus aneurysm
-
MRI: A large cavernous sinus aneurysm
-
MRI: A large cavernous sinus aneurysm





-
MRI: A large cavernous sinus aneurysm
-
MRI: A large cavernous sinus aneurysm
-
MRI: A large cavernous sinus aneurysm
-
MRI: A large cavernous sinus aneurysm




Cerebral Vascular Malformations
Copyleft Images courtesy of RadsWiki



Differentiating intracranial aneurysm from Other Diseases
Intracranial aneurysmmust be differentiated from other diseases that cause seizure, visual disturbance, and constitutional symptoms, such as:
- Oligodendroglioma
- Meningioma
- Astrocytoma
- Pituitary adenoma
- Schwannoma
- primary CNS lymphoma
- Medulloblastoma
- Ependymoma
- Craniopharyngioma
- Pinealoma
- AV malformation
- Hemangioblastoma
- Bacterial brain abscess
- Tuberculosis
- Toxoplasmosis
- Hydatid cyst
- CNS cryptococcosis
- CNS aspergillosis
- Brain metastasis
For more information click here.
Videos: Histopathology
Histopathology: Arteriovenous Malformation (Pons)
{{#ev:youtube|YcOqcu1xmFc}}
Histopathology: Arteriovenous Malformation (Brain)
{{#ev:youtube|mZyNihzHysk}}
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 Stehbens W. The pathogenesis of intracranial aneurysms. In: Tindall GT CP, Barrow DL, editor. The Practice of Neurosurgery. Baltimore: Williams and Wilkins; 1996. p. 1941-1952.
- ↑ Stehbens WE. Flow in glass models of arterial bifurcations and berry aneurysms at low Reynolds numbers. Q J Exp Physiol Cogn Med Sci 1975;60(3):181-192.
- ↑ Kittelberger R, Davis PF, Stehbens WE. Distribution of type IV collagen, laminin, nidogen and fibronectin in the haemodynamically stressed vascular wall. Histol Histopathol 1990;5(2):161-167.
- ↑ Steinberg GK CM. Morphology and structural pathology. In: Awad IA B, DL, editor. Giant Intracranial Aneurysms. Park Ridge: AANS; 1995. p. 1-11.
- ↑ Qureshi AI, Suarez JI, Parekh PD, Sung G, Geocadin R, Bhardwaj A, et al. Risk factors for multiple intracranial aneurysms. Neurosurgery 1998;43(1):22-27.
- ↑ Qureshi AI, Sung GY, Suri MF, Straw RN, Guterman LR, Hopkins LN. Factors associated with aneurysm size in patients with subarachnoid hemorrhage: effect of smoking and aneurysm location. Neurosurgery 2000;46(1):44-50.
- ↑ 7.0 7.1 Qureshi AI, Suri MF, Yahia AM, Suarez JI, Guterman LR, Hopkins LN, et al. Risk factors for subarachnoid hemorrhage. Neurosurgery 2001;49(3):607-613.
- ↑ Chason J. Berry aneurysms of the circle of Willis: results of a planned autopsy study. Neurology 1958;8:41-44.
- ↑ 9.0 9.1 9.2 Weir B. Intracranial aneurysms. In: Wilkins RH RS, editor. Neurosurgery: McGraw Hill; 1985. p. 1308-1329.
- ↑ Suzuki J. Multiple aneurysms: treatment. In: Pia HW LC, Zierski J, editor. Cerebral aneurysms: advances in diagnosis and therapy. Berlin: Springer; 1979. p. 352-363.
- ↑ Hop JW, Rinkel GJ, Algra A, van Gijn J. Case-fatality rates and functional outcome after subarachnoid hemorrhage: a systematic review. Stroke 1997;28(3):660-664.
- ↑ Mayberg MR, Batjer HH, Dacey R, Diringer M, Haley EC, Heros RC, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage. A statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Circulation 1994;90(5):2592-2605.
- ↑ Bendok BR, Getch CC, Malisch TW, Batjer HH. Treatment of aneurysmal subarachnoid hemorrhage. Semin Neurol 1998;18(4):521-531.
- ↑ 14.0 14.1 Frazee JG, Cahan LD, Winter J. Bacterial intracranial aneurysms. J Neurosurg 1980;53(5):633-641.
- ↑ Bohmfalk GL, Story JL, Wissinger JP, Brown WE, Jr. Bacterial intracranial aneurysm. J Neurosurg 1978;48(3):369-382.
- ↑ Molinari GF, Smith L, Goldstein MN, Satran R. Pathogenesis of cerebral mycotic aneurysms. Neurology 1973;23(4):325-332.
- ↑ Venkatesh SK, Phadke RV, Kalode RR, Kumar S, Jain VK. Intracranial infective aneurysms presenting with haemorrhage: an analysis of angiographic findings, management and outcome. Clin Radiol 2000;55(12):946-953.
- ↑ Pootrakul A, Carter LP. Bacterial intracranial aneurysm: importance of sequential angiography. Surg Neurol 1982;17(6):429-431.
- ↑ Kovoor JM, Jayakumar PN, Srikanth SG, Sampath S. Intracranial infective aneurysms: angiographic evaluation with treatment. Neurol India 2001;49(3):262-266.
- ↑ 20.0 20.1 Hurst RW, Judkins A, Bolger W, Chu A, Loevner LA. Mycotic aneurysm and cerebral infarction resulting from fungal sinusitis: imaging and pathologic correlation. AJNR Am J Neuroradiol 2001;22(5):858-863.
- ↑ Yamaura A. Nontraumatic intracranial arterial dissection: Natural history, diagnosis, and treatment. Contemp Neurosurg 1994;16(5):1-6.
- ↑ 22.0 22.1 Batjer H, Suss RA, Samson D. Intracranial arteriovenous malformations associated with aneurysms. Neurosurgery 1986;18(1):29-35.
- ↑ 23.0 23.1 23.2 Fisher W. Concomitant intracranial aneurysms and arteriovenous malformations. In: Wilkins RH RS, editor. Neurosurgery. New York: McGraw Hill; 1996.
- ↑ Berenstein A, Lasjaunias P. Surgical Neuroangiography. New York: Springer-Verlag; 1999, p. 1-88.
- ↑ 25.0 25.1 Kondziolka D, Nixon BJ, Lasjaunias P, Tucker WS, TerBrugge K, Spiegel SM. Cerebral arteriovenous malformations with associated arterial aneurysms: hemodynamic and therapeutic considerations. Can J Neurol Sci 1988;15(2):130-134.
- ↑ Miyasaka K, Wolpert SM, Prager RJ. The association of cerebral aneurysms, infundibula, and intracranial arteriovenous malformations. Stroke 1982;13(2):196-203.
- ↑ 27.0 27.1 Redekop G, TerBrugge K, Montanera W, Willinsky R. Arterial aneurysms associated with cerebral arteriovenous malformations: classification, incidence, and risk of hemorrhage. J Neurosurg 1998;89(4):539-546.
- ↑ Burton C, Johnston J. Multiple cerebral aneurysms and cardiac myxoma. N Engl J Med 1970;282(1):35-36.
- ↑ Fisher C. Cerebral miliary aneurysms in hypertension. Am J Pathol 1971;66:313-330.
- ↑ Stehbens WE. Flow in glass models of arterial bifurcations and berry aneurysms at low Reynolds numbers. Q J Exp Physiol Cogn Med Sci 1975;60(3):181-192.
- ↑ Ondra SL, Troupp H, George ED, Schwab K. The natural history of symptomatic arteriovenous malformations of the brain: a 24-year follow-up assessment. J Neurosurg 1990; 73(3): 387-391.
- ↑ Uranishi R, Baev NI, Ng PY, Kim JH, Awad IA. Expression of endothelial cell angiogenesis receptors in human cerebrovascular malformations. Neurosurgery 2001;48(2):359-368.
- ↑ Wong JH, Awad IA, Kim JH. Ultrastructural pathological features of cerebrovascular malformations: a preliminary report. Neurosurgery 2000;46(6):1454-1459.
- ↑ 34.0 34.1 Rothbart D, Awad IA, Lee J, Kim J, Harbaugh R, Criscuolo GR. Expression of angiogenic factors and structural proteins in central nervous system vascular malformations. Neurosurgery 1996;38(5):915-925.
- ↑ 35.0 35.1 Tomlinson FH, Rufenacht DA, Sundt TM, Jr., Nichols DA, Fode NC. Arteriovenous fistulas of the brain and the spinal cord. J Neurosurg 1993;79(1):16-27.
- ↑ 36.0 36.1 Bendok BR, Getch CC, Frederiksen J, Batjer HH. Resection of a large arteriovenous fistula of the brain using low-flow deep hypothermic cardiopulmonary bypass: technical case report. Neurosurgery 1999;44(4):888-891.
- ↑ 37.0 37.1 Malek AM, Halbach VV, Higashida RT, Phatouros CC, Meyers PM, Dowd CF. Treatment of dural arteriovenous malformations and fistulas. Neurosurg Clin N Am 2000;11(1):147-166.