Glioblastoma multiforme: Difference between revisions
Varun Kumar (talk | contribs) No edit summary |
Varun Kumar (talk | contribs) No edit summary |
||
| Line 1: | Line 1: | ||
__NOTOC__ | __NOTOC__ | ||
'''For patient information, click [[Brain tumor (patient information)|here]]''' | |||
{{DiseaseDisorder infobox | | {{DiseaseDisorder infobox | | ||
Name = Glioblastoma multiforme | | Name = Glioblastoma multiforme | | ||
Revision as of 20:06, 4 August 2011
For patient information, click here Template:DiseaseDisorder infobox
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Glioblastoma multiforme (GBM), also known as grade 4 astrocytoma, is the most common and aggressive type of primary brain tumor, accounting for 52% of all primary brain tumor cases and 20% of all intracranial tumors. Despite being the most prevalent form of primary brain tumor, GBMs occur in only 2-3 cases per 100,000 people in Europe and North America.
Treatment can involve chemotherapy, radiotherapy, and surgery, all of which are acknowledged as palliative measures, meaning that they do not provide a cure. The five-year survival rate of the disease has remained unchanged over the past 30 years and stands at less than three percent. Even with complete surgical resection of the tumor, combined with the best available treatment, the survival rate for GBM remains very low.
-
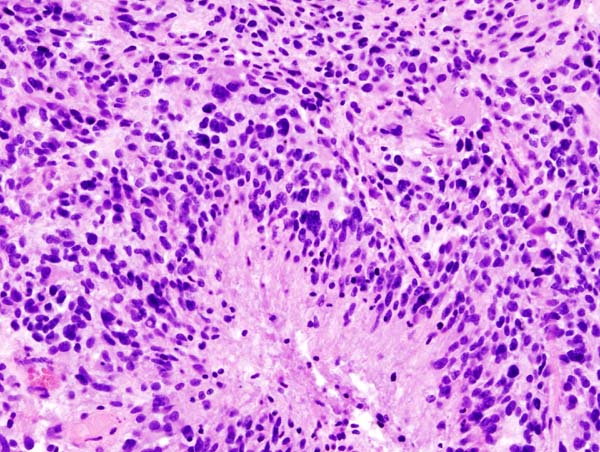
Glioblastoma (histology slide)
-
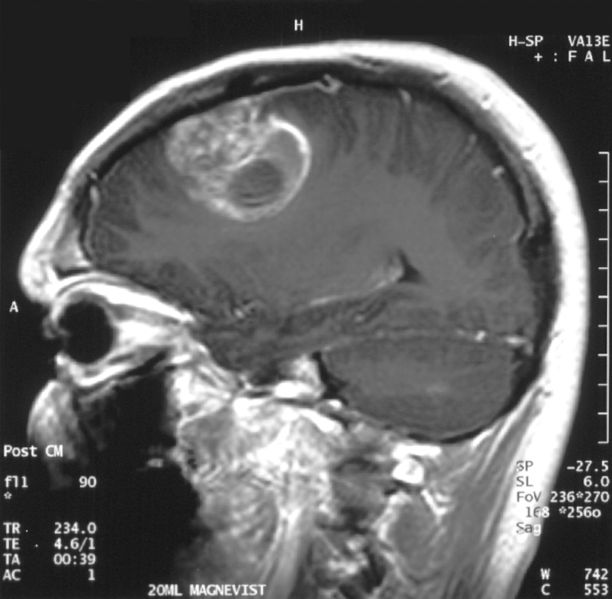
Image 1b. Sagittal MRI with contrast of a glioblastoma WHO grade IV in a 15-year-old boy
.jpg)

Causes
Almost all cases of GBM are sporadic, without a familial predilection, although chromosomal aberrations such as PTEN mutation, and p53 mutation are commonly seen in these tumors. Growth factor aberrant signaling associated with EGFR, and PDGF are also seen.
Pathogenesis
Glioblastomas multiforme are characterized by the presence of small areas of necrotizing tissue that is surrounded by highly-anaplastic cells (pseudopalisading necrosis). This characteristic, as well as the presence of hyperplastic blood vessels, differentiates the tumor from Grade 3 astrocytomas, which do not have these features. Although glioblastoma multiforme can be formed from lower-grade astrocytomas, post-mortem autopsies have revealed that most glioblastomas multiforme are not caused by previous lesions in the brain
Unlike oligodendrogliomas, glioblastomas multiforme can form in either the gray matter or the white matter of the brain; but most GBM arises from the deep white matter and quickly infiltrate the brain, often becoming very large before producing symptoms. The tumor may extend to the meningeal or ventricular wall, leading to the high protein content of cerebrospinal fluid (CSF) (> 100 mg/dL), as well as an occasional pleocytosis of 10 to 100 cells, mostly lymphocytes. Malignant cells carried in the CSF may spread to the spinal cord or cause meningeal gliomatosis. However, metastasis of GBM beyond the central nervous system is extremely rare. About 50% of GBM occupy more than one lobe of a hemisphere or are bilateral. Tumors of this type usually arise from the cerebrum and may exhibit the classic infiltrate across the corpus callosum, producing a butterfly (bilateral) glioma.
The tumor may take on a variety of appearances, depending on the amount of hemorrhage, necrosis, or its age. A CT scan will usually show a nonhomogeneous mass with a hypointense center and a variable ring of enhancement surrounded by edema. Part of a lateral ventricle is usually deformed, and both lateral and third ventricles may be displaced.
Symptoms
Although common symptoms of the disease include seizure, nausea and vomiting, headache, and hemiparesis, the single most prevalent symptom is a progressive memory, personality, or neurological deficit due to temporal and frontal lobe involvement. The kind of symptoms produced depends highly on the location of the tumor, more so than on its pathological properties. The tumor can start producing symptoms quickly, but occasionally is asymptomatic until it reaches an enormous size. See Symptoms section in:
Diagnosis
Diagnosis of a suspected GBM on CT or MRI should rest on a stereotactic biopsy or by a craniotomy, which can, at the same time, remove as much tumor as possible. Although the entire tumor can never be removed, in theory due to its multicentricity and diffuse character, partial resection ("debulking") can still prolong survival slightly.
Treatment
Treatment of primary brain tumors and brain metastases consists of both symptomatic and palliative therapies.
Symptomatic therapy
Supportive treatment focuses on relieving symptoms and improving the patient’s neurologic function. The primary supportive agents are anticonvulsants and corticosteroids.
- Anticonvulsants are administered to the ~25% of patients who have a seizure. Prospective studies have failed to show the efficacy for prophylactic anticonvulsants. Those receiving phenytoin concurrent with radiation may have serious skin reactions such as erythema multiforme and Stevens-Johnson syndrome.
- Corticosteroids, usually dexamethasone given 4 to 10 mg every 4 to 6 h, can reduce peritumoral edema (through rearrangement of the blood-brain barrier), diminishing mass effect and lowering intracranial pressure, with a decrease in headache or drowsiness.
Palliative therapy
Palliative treatment usually is done to achieve a longer survival time, albeit only a slight increase [see below]. It includes surgery, radiation therapy, and chemotherapy.
A maximally feasible resection with maximal tumor-free margins ("debulking") is usually performed along with external beam radiation and chemotherapy. Total cranial irradiation (4500 cGy) with a boosted dose (1500 to 2000 cGy) at the site of the tumor can increase survival by 5 months [see below]. The addition of the chemotherapeutic agent carmustine (BiCNU) alone increases survival slightly. Most oncologists prefer a combination chemotherapy consisting of procarbazine, lomustine, and vincristine (PCV regimen). Another combination includes carboplatin and cisplatin. Their efficacy is limited, and toxicity, particularly with the PCV regimen, can be considerable. Despite initial studies suggesting the superiority of PCV over BiCNU, there are now clear data demonstrating no benefit of PCV over BiCNU in either glioblastoma or anaplastic astrocytoma patients. Brachytherapy (implantation of radioactive beads or needles) and high-dose focus radiotherapy (stereotactic radiosurgery) have not shown to increase survival times.
In a large phase III trial, implantation of BiCNU-impregnated wafers - trade name Gliadel Wafers - at the time of primary resection, improved median survival to 13.9 months, compared with only 11.6 months for placebo wafers (P = .03), in newly-diagnosed patients with malignant glioma.[1] Despite initial treatment, virtually all malignant gliomas recur. At relapse, patients may benefit from re-resection, focal radiotherapy techniques (such as radiosurgery), and different chemotherapeutic agents. Depending upon which chemotherapeutic agent was used at initial treatment, temozolomide, procarbazine, or a nitrosourea would be a reasonable conventional choice at recurrence. Clinical trials employing signal transduction inhibitors, epidermal growth factor receptor inhibitors, or antiangiogenic agents may also be available at tumor relapse.
The use of temozolomide alongside radiotherapy has shown survival benefit,[2] and is currently considered the standard of care by the National Cancer Institute.[3]
In recent studies, the antimalarial drug chloroquine has been shown to increase mid-term survival when given in combination with conventional therapy.[4][5][6] Further research in this area needs to be done.
Another possible therapy technique is to use viruses to attack the cancer.[7]
A recent paper titled reported on the treatment of glioblastoma multiforme with photodynamic therapy at Melbourne Royal Infirmary, Australia since 1986.[8] Five year survival rates were over 30% with some patients surviving over 10 years.
Yet another recent - but still experimental - therapy approach is the treatment using nanoparticles. [9] These consist of an iron oxide core as well as a cover facilitating the infiltration of the particles into the cancer cells. The particles are injected directly into the tumor. The tumor enriched with the iron oxide particles is then repeatedly warmed via alternating magnetic fields to above 46 degrees Celsius. In animal models, considerably-improved survival terms arose[10]; however, at present there are not any results from efficacy studies in man yet, but results are expected to be published later this year.
Recurrences
Tumor recurrence after surgery or radiation is almost inevitable, usually within 2 cm of the original site, and 10% may develop new lesions at distant sites. Reoperation or brachytherapy has been attempted, with uncertain results.[11][12] The most aggressive therapy, a second surgery and chemotherapy, is, in general, used in those under 40 years of age whose original operation was many months earlier. If the PCV regimen has not been used, it may be tried; else, the newer agent temozolomide may be used. However, these regimens usually only increase the symptom-free interval, rather than prolong survival.
Prognosis
The median survival time from the time of diagnosis without any treatment is 3 months. Increasing age (> 60 years of age) carries a worse prognostic risk. Death is usually due to cerebral edema or increased intracranial pressure.
With standard treatment (radiotherapy, chemotherapy (such as temozolomide), and surgery), the median survival is approximately 14 months.[13] Less than 10% of these patients survive past 5 years.
A study published in 2007 reported the 2-year survival at 27.3%, 3-year survival 16.7% and 4 year survival 12.9%.14
Is Long-Term Survival in Glioblastoma Possible? Updated Results of the EORTC/NCIC Phase III Randomized Trial on Radiotherapy (RT) and Concomitant and Adjuvant Temozolomide (TMZ) versus RT Alone R. Mirimanoff , W. Mason , M. Van den Bent , R. Kortmann , M. Taphoorn , A. Brandes , S. Villa , G. Cairncrosss , T. Gorlia , R. Stupp International Journal of Radiation Oncology * Biology * Physics- November 2007 1 (Vol. 69, Issue 3, Page S2, DOI: 10.1016/j.ijrobp.2007.07.004) http://www.redjournal.org/article/PIIS036030160701187X/fulltext
References
- ↑ Westphal M, Hilt DC, Bortey E; et al. (2003). "A phase 3 trial of local chemotherapy with biodegradable carmustine (BCNU) wafers (Gliadel wafers) in patients with primary malignant glioma". Neuro-oncology. 5 (2): 79–88. doi:10.1215/S1522-8517-02-00023-6. PMID 12672279.
- ↑ Stupp R, Mason WP, van den Bent MJ; et al. (2005). "Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma". N. Engl. J. Med. 352 (10): 987–96. doi:10.1056/NEJMoa043330. PMID 15758009.
- ↑ "Temozolomide Plus Radiation Helps Brain Cancer - National Cancer Institute". Retrieved 2007-09-15.
- ↑ Sotelo J, Briceño E, López-González MA (2006). "Adding chloroquine to conventional treatment for glioblastoma multiforme: a randomized, double-blind, placebo-controlled trial". Ann. Intern. Med. 144 (5): 337–43. PMID 16520474.
- ↑ Toler SM, Noe D, Sharma A (2006). "Selective enhancement of cellular oxidative stress by chloroquine: implications for the treatment of glioblastoma multiforme". Neurosurgical focus. 21 (6): E10. PMID 17341043.
- ↑ Briceño E, Calderon A, Sotelo J (2007). "Institutional experience with chloroquine as an adjuvant to the therapy for glioblastoma multiforme". Surgical neurology. 67 (4): 388–91. doi:10.1016/j.surneu.2006.08.080. PMID 17350410.
- ↑ Hoffmann D, Wildner O (2007). "Comparison of herpes simplex virus- and conditionally replicative adenovirus-based vectors for glioblastoma treatment". Cancer Gene Ther. 14 (7): 627–39. doi:10.1038/sj.cgt.7701055. PMID 17479104.
- ↑ Stylli SS, Kaye AH, MacGregor L, Howes M, Rajendra P (2005). "Photodynamic therapy of high grade glioma - long term survival". Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 12 (4): 389–98. doi:10.1016/j.jocn.2005.01.006. PMID 15925768.
- ↑ Maier-Hauff et al.: Intracranial thermotherapy using magnetic nanoparticles combined with external beam radiotherapy: results of a feasibility study on patients with glioblastoma multiforme. J Neurooncol. 2007 Jan;81(1):53-60. PMID 16773216
- ↑ Jordan et al.:The effect of thermotherapy using magnetic nanoparticles on rat malignant glioma. J Neurooncol. 2006 May;78(1):7-14. PMID 16314937
- ↑ Welsh J, Sanan A, Gabayan AJ; et al. (2007). "GliaSite brachytherapy boost as part of initial treatment of glioblastoma multiforme: a retrospective multi-institutional pilot study". Int. J. Radiat. Oncol. Biol. Phys. 68 (1): 159–65. doi:10.1016/j.ijrobp.2006.11.053. PMID 17331666.
- ↑ Chen AM, Chang S, Pouliot J; et al. (2007). "Phase I Trial of Gross Total Resection, Permanent Iodine-125 Brachytherapy, and Hyperfractionated Radiotherapy for Newly Diagnosed Glioblastoma Multiforme". doi:10.1016/j.ijrobp.2007.03.061. PMID 17512132.
- ↑ Stupp R, Mason W, van den Bent M, Weller M, Fisher B, Taphoorn M, Belanger K, Brandes A, Marosi C, Bogdahn U, Curschmann J, Janzer R, Ludwin S, Gorlia T, Allgeier A, Lacombe D, Cairncross J, Eisenhauer E, Mirimanoff R (2005). "Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma". N Engl J Med. 352 (10): 987–96. PMID 15758009.
Additional reading
External links
- National Cancer Institute Clinical Trials
- North America Brain Tumor Coalition
- German Brain Tumor Association
- Glioblastoma multiforme - A new Viro-therapy developed at the Hebrew University - An IsraCast article
- Emedicine.com article on glioblastoma multiforme
- Young Adults Surviving Glioblastoma support group
- A Glioblastoma Multiforme Foundation
- Glioblastoma Images MedPix Medical Image Database
Template:Nervous tissue tumors Template:SIB
de:Glioblastom it:Glioblastoma multiforme la:Glioblastoma multiforme no:Glioblastoma multiforme