Cardiogenic shock pathophysiology: Difference between revisions
No edit summary |
|||
| (10 intermediate revisions by one other user not shown) | |||
| Line 1: | Line 1: | ||
__NOTOC__ | __NOTOC__ | ||
{{Cardiogenic shock}} | {{Cardiogenic shock}} | ||
{{CMG}}; {{AE}} {{JS}} {{sali}} | {{CMG}}; {{AE}} [[User:Mohammad Salih|Mohammad Salih, MD.]] {{JS}} {{sali}} | ||
==Overview== | ==Overview== | ||
The pathophysiology of [[cardiogenic]] [[shock]] is complex and not fully understood. Ischemia to the [[myocardium]] causes derangement to both [[systolic]] and [[diastolic]] left ventricular function, resulting in a profound [[depression]] of [[myocardial contractility]]. This, in turn, leads to a potentially [[catastrophic]] and [[vicious]] spiral of reduced [[cardiac output]] and low [[blood pressure]], perpetuating further [[coronary ischemia]] and impairment of [[contractility]]. Several [[physiologic]] compensatory processes ensue. These include:The activation of the sympathetic system leading to peripheral [[vasoconstriction]] which may improve [[coronary]] perfusion at the cost of increased [[afterload]], and | |||
[[Tachycardia]] which increases [[myocardial]] oxygen demand and subsequently worsens [[myocardial]] ischemia.These compensatory mechanisms are subsequently counteracted by [[pathologic]] [[vasodilation]] that occurs from the release of potent systemic [[inflammatory]] markers such as [[interleukin-1]], [[tumor necrosis factor]] a, and [[interleukin-6]]. Additionally, higher levels of [[nitric oxide]] and [[peroxynitrite]] are released, which also contribute to [[pathologic]] [[vasodilation]] and are known to be [[cardiotoxic]]. Unless interrupted by adequate treatment measures, this self-perpetuating cycle leads to global [[hypoperfusion]] and the inability to effectively meet the [[metabolic]] demands of the tissues, progressing to [[multiorgan]] failure and eventually [[death]]. | |||
==Pathophysiology== | ==Pathophysiology== | ||
| Line 25: | Line 25: | ||
==The downward "Spiral" of Cardiogenic shock== | ==The downward "Spiral" of Cardiogenic shock== | ||
*Cardiac dysfunction in patients with cardiogenic shock is usually initiated by myocardial infarction or ischemia. | *[[Cardiac dysfunction]] in patients with [[cardiogenic shock]] is usually initiated by [[myocardial infarction]] or [[ischemia]]. | ||
*The myocardial dysfunction resulting from ischemia worsens that ischemia, creating a downward spiral. | *The [[myocardial dysfunction]] resulting from [[ischemia]] worsens that ischemia, creating a downward spiral. | ||
*When a critical mass of left ventricular myocardium is ischemic or necrotic and fails to pump, stroke volume and cardiac output decrease. | *When a critical mass of [[left ventricular]] [[myocardium]] is [[ischemic]] or [[necrotic]] and fails to pump, [[stroke volume]] and [[cardiac output]] decrease. | ||
*Myocardial perfusion, which depends on the pressure gradient between the coronary arterial system and the left ventricle. | *Myocardial perfusion, which depends on the pressure gradient between the [[coronary]] arterial system and the [[left ventricle]]. | ||
*The duration of diastole, is compromised by hypotension and tachycardia. Which in turn, exacerbates ischemia. | *The duration of diastole, is compromised by hypotension and tachycardia. Which in turn, exacerbates ischemia. | ||
*The increased ventricular diastolic pressures caused by pump failure further reduce coronary perfusion pressure, and the additional wall stress elevates myocardial oxygen requirements, further worsening ischemia. | *The increased [[ventricular diastolic pressures]] caused by pump failure further reduce [[coronary perfusion pressure]], and the additional wall stress elevates myocardial oxygen requirements, further worsening ischemia. | ||
*Decreased cardiac output also compromises systemic perfusion, which can lead to lactic acidosis and further compromise of systolic performance. | *Decreased cardiac output also compromises systemic perfusion, which can lead to lactic acidosis and further compromise of systolic performance. | ||
*The pathologic process begins with [[myocardial]] [[ischemia]] leading to an abnormal function of the [[cardiac muscle]]. | *The pathologic process begins with [[myocardial]] [[ischemia]] leading to an abnormal function of the [[cardiac muscle]]. | ||
| Line 73: | Line 73: | ||
==Ventricular Septal and Free Wall Rupture== | ==Ventricular Septal and Free Wall Rupture== | ||
*[[Ventricular septal rupture]] and [[free wall rupture]], which constitute two entities of [[cardiac rupture]], represent the second most common cause of death in patients with acute [[myocardial infarction]], during hospital stay.<ref name="pmid19064683">{{cite journal| author=Figueras J, Alcalde O, Barrabés JA, Serra V, Alguersuari J, Cortadellas J et al.| title=Changes in hospital mortality rates in 425 patients with acute ST-elevation myocardial infarction and cardiac rupture over a 30-year period. | journal=Circulation | year= 2008 | volume= 118 | issue= 25 | pages= 2783-9 | pmid=19064683 | doi=10.1161/CIRCULATIONAHA.108.776690 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=19064683 }} </ref><ref name="pmid8626938">{{cite journal| author=Becker RC, Gore JM, Lambrew C, Weaver WD, Rubison RM, French WJ et al.| title=A composite view of cardiac rupture in the United States National Registry of Myocardial Infarction. | journal=J Am Coll Cardiol | year= 1996 | volume= 27 | issue= 6 | pages= 1321-6 | pmid=8626938 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=8626938 }} </ref><ref name="pmid9973029">{{cite journal| author=Becker RC, Hochman JS, Cannon CP, Spencer FA, Ball SP, Rizzo MJ et al.| title=Fatal cardiac rupture among patients treated with thrombolytic agents and adjunctive thrombin antagonists: observations from the Thrombolysis and Thrombin Inhibition in Myocardial Infarction 9 Study. | journal=J Am Coll Cardiol | year= 1999 | volume= 33 | issue= 2 | pages= 479-87 | pmid=9973029 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=9973029 }} </ref> | *[[Ventricular septal rupture]] and [[free wall rupture]], which constitute two entities of [[cardiac rupture]], represent the second most common cause of death in patients with acute [[myocardial infarction]], during hospital stay.<ref name="pmid19064683">{{cite journal| author=Figueras J, Alcalde O, Barrabés JA, Serra V, Alguersuari J, Cortadellas J et al.| title=Changes in hospital mortality rates in 425 patients with acute ST-elevation myocardial infarction and cardiac rupture over a 30-year period. | journal=Circulation | year= 2008 | volume= 118 | issue= 25 | pages= 2783-9 | pmid=19064683 | doi=10.1161/CIRCULATIONAHA.108.776690 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=19064683 }} </ref><ref name="pmid8626938">{{cite journal| author=Becker RC, Gore JM, Lambrew C, Weaver WD, Rubison RM, French WJ et al.| title=A composite view of cardiac rupture in the United States National Registry of Myocardial Infarction. | journal=J Am Coll Cardiol | year= 1996 | volume= 27 | issue= 6 | pages= 1321-6 | pmid=8626938 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=8626938 }} </ref><ref name="pmid9973029">{{cite journal| author=Becker RC, Hochman JS, Cannon CP, Spencer FA, Ball SP, Rizzo MJ et al.| title=Fatal cardiac rupture among patients treated with thrombolytic agents and adjunctive thrombin antagonists: observations from the Thrombolysis and Thrombin Inhibition in Myocardial Infarction 9 Study. | journal=J Am Coll Cardiol | year= 1999 | volume= 33 | issue= 2 | pages= 479-87 | pmid=9973029 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=9973029 }} </ref> | ||
*Ventricular septal rupture in the SHOCK registry, it accounted for 4.6% of the cases of cardiogenic shock.<ref name="pmid10985706">{{cite journal| author=Hochman JS, Buller CE, Sleeper LA, Boland J, Dzavik V, Sanborn TA et al.| title=Cardiogenic shock complicating acute myocardial infarction--etiologies, management and outcome: a report from the SHOCK Trial Registry. SHould we emergently revascularize Occluded Coronaries for cardiogenic shocK? | journal=J Am Coll Cardiol | year= 2000 | volume= 36 | issue= 3 Suppl A | pages= 1063-70 | pmid=10985706 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10985706 }} </ref> | |||
*The most recent registries show that [[ventricular septal rupture]] generally develops within the first 16 to 24 hours post-[[MI]] and has the following characteristics:<ref name="pmid10985712">{{cite journal| author=Thompson CR, Buller CE, Sleeper LA, Antonelli TA, Webb JG, Jaber WA et al.| title=Cardiogenic shock due to acute severe mitral regurgitation complicating acute myocardial infarction: a report from the SHOCK Trial Registry. SHould we use emergently revascularize Occluded Coronaries in cardiogenic shocK? | journal=J Am Coll Cardiol | year= 2000 | volume= 36 | issue= 3 Suppl A | pages= 1104-9 | pmid=10985712 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10985712 }} </ref><ref name="pmid10618300">{{cite journal| author=Crenshaw BS, Granger CB, Birnbaum Y, Pieper KS, Morris DC, Kleiman NS et al.| title=Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial infarction. GUSTO-I (Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries) Trial Investigators. | journal=Circulation | year= 2000 | volume= 101 | issue= 1 | pages= 27-32 | pmid=10618300 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10618300 }} </ref><ref name="pmid7020978">{{cite journal| author=Radford MJ, Johnson RA, Daggett WM, Fallon JT, Buckley MJ, Gold HK et al.| title=Ventricular septal rupture: a review of clinical and physiologic features and an analysis of survival. | journal=Circulation | year= 1981 | volume= 64 | issue= 3 | pages= 545-53 | pmid=7020978 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=7020978 }} </ref><ref name="pmid2803872">{{cite journal| author=Skehan JD, Carey C, Norrell MS, de Belder M, Balcon R, Mills PG| title=Patterns of coronary artery disease in post-infarction ventricular septal rupture. | journal=Br Heart J | year= 1989 | volume= 62 | issue= 4 | pages= 268-72 | pmid=2803872 | doi= | pmc=PMC1277362 | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=2803872 }} </ref><ref name="pmid13836145">{{cite journal| author=SWITHINBANK JM| title=Perforation of the interventricular septum in myocardial infarction. | journal=Br Heart J | year= 1959 | volume= 21 | issue= | pages= 562-6 | pmid=13836145 | doi= | pmc=PMC1017615 | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=13836145 }} </ref><ref name="NgYeghiazarians2011">{{cite journal|last1=Ng|first1=R.|last2=Yeghiazarians|first2=Y.|title=Post Myocardial Infarction Cardiogenic Shock: A Review of Current Therapies|journal=Journal of Intensive Care Medicine|volume=28|issue=3|year=2011|pages=151–165|issn=0885-0666|doi=10.1177/0885066611411407}}</ref><ref>{{cite book | last = Cohn | first = Lawrence | title = Cardiac surgery in the adult | publisher = McGraw-Hill Medical | location = New York | year = 2012 | isbn = 978-0-07-163310-9 }}</ref><ref name="NgYeghiazarians2011">{{cite journal|last1=Ng|first1=R.|last2=Yeghiazarians|first2=Y.|title=Post Myocardial Infarction Cardiogenic Shock: A Review of Current Therapies|journal=Journal of Intensive Care Medicine|volume=28|issue=3|year=2011|pages=151–165|issn=0885-0666|doi=10.1177/0885066611411407}}</ref><ref name="pmid8354804">{{cite journal| author=Oliva PB, Hammill SC, Edwards WD| title=Cardiac rupture, a clinically predictable complication of acute myocardial infarction: report of 70 cases with clinicopathologic correlations. | journal=J Am Coll Cardiol | year= 1993 | volume= 22 | issue= 3 | pages= 720-6 | pmid=8354804 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=8354804 }} </ref><ref name="pmid10985714">{{cite journal| author=Slater J, Brown RJ, Antonelli TA, Menon V, Boland J, Col J et al.| title=Cardiogenic shock due to cardiac free-wall rupture or tamponade after acute myocardial infarction: a report from the SHOCK Trial Registry. Should we emergently revascularize occluded coronaries for cardiogenic shock? | journal=J Am Coll Cardiol | year= 2000 | volume= 36 | issue= 3 Suppl A | pages= 1117-22 | pmid=10985714 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10985714 }} </ref> | |||
*According to the SHOCK trial data, this type of rupture had 55% of [[mortality rate]] within the first 30 days.<ref name="pmid10985714">{{cite journal| author=Slater J, Brown RJ, Antonelli TA, Menon V, Boland J, Col J et al.| title=Cardiogenic shock due to cardiac free-wall rupture or tamponade after acute myocardial infarction: a report from the SHOCK Trial Registry. Should we emergently revascularize occluded coronaries for cardiogenic shock? | journal=J Am Coll Cardiol | year= 2000 | volume= 36 | issue= 3 Suppl A | pages= 1117-22 | pmid=10985714 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10985714 }} </ref> [[Free wall rupture]] may also be classified as ''simple'' or ''complex''. It may occur either on the anterior or the lateral and posterior [[left ventricular]] walls.<ref name="pmid10985714">{{cite journal| author=Slater J, Brown RJ, Antonelli TA, Menon V, Boland J, Col J et al.| title=Cardiogenic shock due to cardiac free-wall rupture or tamponade after acute myocardial infarction: a report from the SHOCK Trial Registry. Should we emergently revascularize occluded coronaries for cardiogenic shock? | journal=J Am Coll Cardiol | year= 2000 | volume= 36 | issue= 3 Suppl A | pages= 1117-22 | pmid=10985714 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10985714 }} </ref><ref name="pmid19064683">{{cite journal| author=Figueras J, Alcalde O, Barrabés JA, Serra V, Alguersuari J, Cortadellas J et al.| title=Changes in hospital mortality rates in 425 patients with acute ST-elevation myocardial infarction and cardiac rupture over a 30-year period. | journal=Circulation | year= 2008 | volume= 118 | issue= 25 | pages= 2783-9 | pmid=19064683 | doi=10.1161/CIRCULATIONAHA.108.776690 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=19064683 }} </ref> These last two are thought to [[rupture]] easier, however, because of the higher proportion of anterior [[MI]]s, they are seen less frequently.<ref name="NgYeghiazarians2011">{{cite journal|last1=Ng|first1=R.|last2=Yeghiazarians|first2=Y.|title=Post Myocardial Infarction Cardiogenic Shock: A Review of Current Therapies|journal=Journal of Intensive Care Medicine|volume=28|issue=3|year=2011|pages=151–165|issn=0885-0666|doi=10.1177/0885066611411407}}</ref> | |||
*The [[rupture]] may present with different types of courses: | |||
**''Acute'' - the patient generally feels acute onset of [[chest pain]], developing [[cardiac tamponade]], [[hemodynamic|hemodynamical]] collapse and [[sudden death]]. Because of the rapid course of this type, it is usually not controlled with current therapies.<ref name="pmid10768896">{{cite journal| author=Figueras J, Cortadellas J, Soler-Soler J| title=Left ventricular free wall rupture: clinical presentation and management. | journal=Heart | year= 2000 | volume= 83 | issue= 5 | pages= 499-504 | pmid=10768896 | doi= | pmc=PMC1760810 | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10768896 }} </ref><ref>{{cite book | last = Cohn | first = Lawrence | title = Cardiac surgery in the adult | publisher = McGraw-Hill Medical | location = New York | year = 2012 | isbn = 007163312X }}</ref> | |||
**''Subacute'' - this type generally results in smaller and contained [[rupture|ruptures]]. These may be stabilized by the formation of a [[clot]] or [[fibrinous]] [[pericardial]] [[adhesions]] for a short period of time. Therapeutical measures must be applied urgently.<ref>{{cite book | last = Cohn | first = Lawrence | title = Cardiac surgery in the adult | publisher = McGraw-Hill Medical | location = New York | year = 2012 | isbn = 007163312X }}</ref><ref name="pmid2803872">{{cite journal| author=Skehan JD, Carey C, Norrell MS, de Belder M, Balcon R, Mills PG| title=Patterns of coronary artery disease in post-infarction ventricular septal rupture. | journal=Br Heart J | year= 1989 | volume= 62 | issue= 4 | pages= 268-72 | pmid=2803872 | doi= | pmc=PMC1277362 | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=2803872 }} </ref> | |||
**''Chronic'' - less frequently associated with cardiogenic shock. | |||
==Inflammation and Hemodynamics== | |||
*Studies like the ''SHOCK trial'' show that not all patients follow this classic paradigm, since:<ref name="pmid10460813">{{cite journal| author=Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD et al.| title=Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. | journal=N Engl J Med | year= 1999 | volume= 341 | issue= 9 | pages= 625-34 | pmid=10460813 | doi=10.1056/NEJM199908263410901 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10460813 }} </ref><ref name="pmid12538428">{{cite journal| author=Picard MH, Davidoff R, Sleeper LA, Mendes LA, Thompson CR, Dzavik V et al.| title=Echocardiographic predictors of survival and response to early revascularization in cardiogenic shock. | journal=Circulation | year= 2003 | volume= 107 | issue= 2 | pages= 279-84 | pmid=12538428 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=12538428 }} </ref><ref name="pmid16043684">{{cite journal| author=Kohsaka S, Menon V, Lowe AM, Lange M, Dzavik V, Sleeper LA et al.| title=Systemic inflammatory response syndrome after acute myocardial infarction complicated by cardiogenic shock. | journal=Arch Intern Med | year= 2005 | volume= 165 | issue= 14 | pages= 1643-50 | pmid=16043684 | doi=10.1001/archinte.165.14.1643 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16043684 }} </ref> | |||
Studies like the ''SHOCK trial'' show that not all patients follow this classic paradigm, since:<ref name="pmid10460813">{{cite journal| author=Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD et al.| title=Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. | journal=N Engl J Med | year= 1999 | volume= 341 | issue= 9 | pages= 625-34 | pmid=10460813 | doi=10.1056/NEJM199908263410901 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10460813 }} </ref><ref name="pmid12538428">{{cite journal| author=Picard MH, Davidoff R, Sleeper LA, Mendes LA, Thompson CR, Dzavik V et al.| title=Echocardiographic predictors of survival and response to early revascularization in cardiogenic shock. | journal=Circulation | year= 2003 | volume= 107 | issue= 2 | pages= 279-84 | pmid=12538428 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=12538428 }} </ref><ref name="pmid16043684">{{cite journal| author=Kohsaka S, Menon V, Lowe AM, Lange M, Dzavik V, Sleeper LA et al.| title=Systemic inflammatory response syndrome after acute myocardial infarction complicated by cardiogenic shock. | journal=Arch Intern Med | year= 2005 | volume= 165 | issue= 14 | pages= 1643-50 | pmid=16043684 | doi=10.1001/archinte.165.14.1643 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16043684 }} </ref> | |||
*The range of elevation of [[systemic vascular resistance]] in this trial was wide, suggesting that the compensatory [[vasoconstriction]] wasn't a rule in every patient; | *The range of elevation of [[systemic vascular resistance]] in this trial was wide, suggesting that the compensatory [[vasoconstriction]] wasn't a rule in every patient; | ||
*The mean [[ejection fraction]] was also moderately decreased in this trial, showing that other mechanisms besides [[cardiac failure]] were present; | *The mean [[ejection fraction]] was also moderately decreased in this trial, showing that other mechanisms besides [[cardiac failure]] were present; | ||
*Some of the patients had [[leukocytosis]] and [[fever]], which along with the decreased [[systemic vascular resistance]] suggested [[SIRS]]. | *Some of the patients had [[leukocytosis]] and [[fever]], which along with the decreased [[systemic vascular resistance]] suggested [[SIRS]]. | ||
These facts have introduced the concept that [[myocardial infarction]] may cause [[SIRS]] and that [[inflammation]] plays an important part in the development and persistence of cardiogenic shock, contributing to [[myocardial]] dysfunction and [[vasodilation]]. The possibility of developing [[SIRS]] raises with the increasing permanence in cardiogenic shock.<ref name="ReynoldsHochman2008">{{cite journal|last1=Reynolds|first1=H. R.|last2=Hochman|first2=J. S.|title=Cardiogenic Shock: Current Concepts and Improving Outcomes|journal=Circulation|volume=117|issue=5|year=2008|pages=686–697|issn=0009-7322|doi=10.1161/CIRCULATIONAHA.106.613596}}</ref><ref name="Hochman2003">{{cite journal|last1=Hochman|first1=J. S.|title=Cardiogenic Shock Complicating Acute Myocardial Infarction: Expanding the Paradigm|journal=Circulation|volume=107|issue=24|year=2003|pages=2998–3002|issn=0009-7322|doi=10.1161/01.CIR.0000075927.67673.F2}}</ref><ref name="pmid10636626">{{cite journal| author=Brunkhorst FM, Clark AL, Forycki ZF, Anker SD| title=Pyrexia, procalcitonin, immune activation and survival in cardiogenic shock: the potential importance of bacterial translocation. | journal=Int J Cardiol | year= 1999 | volume= 72 | issue= 1 | pages= 3-10 | pmid=10636626 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10636626 }} </ref> | *These facts have introduced the concept that [[myocardial infarction]] may cause [[SIRS]] and that [[inflammation]] plays an important part in the development and persistence of cardiogenic shock, contributing to [[myocardial]] dysfunction and [[vasodilation]]. | ||
*The possibility of developing [[SIRS]] raises with the increasing permanence in cardiogenic shock.<ref name="ReynoldsHochman2008">{{cite journal|last1=Reynolds|first1=H. R.|last2=Hochman|first2=J. S.|title=Cardiogenic Shock: Current Concepts and Improving Outcomes|journal=Circulation|volume=117|issue=5|year=2008|pages=686–697|issn=0009-7322|doi=10.1161/CIRCULATIONAHA.106.613596}}</ref><ref name="Hochman2003">{{cite journal|last1=Hochman|first1=J. S.|title=Cardiogenic Shock Complicating Acute Myocardial Infarction: Expanding the Paradigm|journal=Circulation|volume=107|issue=24|year=2003|pages=2998–3002|issn=0009-7322|doi=10.1161/01.CIR.0000075927.67673.F2}}</ref><ref name="pmid10636626">{{cite journal| author=Brunkhorst FM, Clark AL, Forycki ZF, Anker SD| title=Pyrexia, procalcitonin, immune activation and survival in cardiogenic shock: the potential importance of bacterial translocation. | journal=Int J Cardiol | year= 1999 | volume= 72 | issue= 1 | pages= 3-10 | pmid=10636626 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10636626 }} </ref> | |||
At the time of the [[cardiac]] injury, the [[myocardium]] releases into [[circulation]] [[cytokines]], particularly during the first 24 to 72 hours after the [[MI]] | *At the time of the [[cardiac]] injury, the [[myocardium]] releases into [[circulation]] [[cytokines]], particularly during the first 24 to 72 hours after the [[MI]]. *These will induce the [[enzyme]] [[nitric oxide synthase]], thereby increasing the level of [[nitric oxide]], which will be responsible for [[vasodilation]] and worsening of [[hypotension]], further jeopardizing [[left ventricle]] performance.<ref>{{Cite book | last1 = Hasdai | first1 = David. | title = Cardiogenic shock : diagnosis and treatmen | date = 2002 | publisher = Humana Press | location = Totowa, N.J. | isbn = 1-58829-025-5 | pages = }}</ref><ref name="NeumannOtt1995">{{cite journal|last1=Neumann|first1=F.-J.|last2=Ott|first2=I.|last3=Gawaz|first3=M.|last4=Richardt|first4=G.|last5=Holzapfel|first5=H.|last6=Jochum|first6=M.|last7=Schomig|first7=A.|title=Cardiac Release of Cytokines and Inflammatory Responses in Acute Myocardial Infarction|journal=Circulation|volume=92|issue=4|year=1995|pages=748–755|issn=0009-7322|doi=10.1161/01.CIR.92.4.748}}</ref><ref name="Shah2000">{{cite journal|last1=Shah|first1=A|title=Inducible nitric oxide synthase and cardiovascular disease|journal=Cardiovascular Research|volume=45|issue=1|year=2000|pages=148–155|issn=00086363|doi=10.1016/S0008-6363(99)00316-8}}</ref><ref name="pmid11489778">{{cite journal| author=Feng Q, Lu X, Jones DL, Shen J, Arnold JM| title=Increased inducible nitric oxide synthase expression contributes to myocardial dysfunction and higher mortality after myocardial infarction in mice. | journal=Circulation | year= 2001 | volume= 104 | issue= 6 | pages= 700-4 | pmid=11489778 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11489778 }} </ref><ref name="pmid10736276">{{cite journal| author=Cotter G, Kaluski E, Blatt A, Milovanov O, Moshkovitz Y, Zaidenstein R et al.| title=L-NMMA (a nitric oxide synthase inhibitor) is effective in the treatment of cardiogenic shock. | journal=Circulation | year= 2000 | volume= 101 | issue= 12 | pages= 1358-61 | pmid=10736276 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10736276 }} </ref><ref name="pmid17133844">{{cite journal| author=Kaluski E, Hendler A, Blatt A, Uriel N| title=Nitric oxide synthase inhibitors in post-myocardial infarction cardiogenic shock--an update. | journal=Clin Cardiol | year= 2006 | volume= 29 | issue= 11 | pages= 482-8 | pmid=17133844 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=17133844 }} </ref> [[NO]] may also form a toxic radical, called [[peroxynitrite]], when combined with [[superoxide]], affecting [[myocardial]] [[contractility]].<ref name="pmid10926876">{{cite journal| author=Ferdinandy P, Danial H, Ambrus I, Rothery RA, Schulz R| title=Peroxynitrite is a major contributor to cytokine-induced myocardial contractile failure. | journal=Circ Res | year= 2000 | volume= 87 | issue= 3 | pages= 241-7 | pmid=10926876 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10926876 }} </ref> | ||
Other [[circulatory]] factors, such as [[procalcitonin]], [[complement]] and [[CRP]], have been reported in some studies to contribute to the development of [[SIRS]] in cardiogenic shock.<ref name="pmid12925454">{{cite journal| author=Granger CB, Mahaffey KW, Weaver WD, Theroux P, Hochman JS, Filloon TG et al.| title=Pexelizumab, an anti-C5 complement antibody, as adjunctive therapy to primary percutaneous coronary intervention in acute myocardial infarction: the COMplement inhibition in Myocardial infarction treated with Angioplasty (COMMA) trial. | journal=Circulation | year= 2003 | volume= 108 | issue= 10 | pages= 1184-90 | pmid=12925454 | doi=10.1161/01.CIR.0000087447.12918.85 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=12925454 }} </ref><ref name="pmid17200474">{{cite journal| author=APEX AMI Investigators. Armstrong PW, Granger CB, Adams PX, Hamm C, Holmes D et al.| title=Pexelizumab for acute ST-elevation myocardial infarction in patients undergoing primary percutaneous coronary intervention: a randomized controlled trial. | journal=JAMA | year= 2007 | volume= 297 | issue= 1 | pages= 43-51 | pmid=17200474 | doi=10.1001/jama.297.1.43 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=17200474 }} </ref> | *Among these released [[cytokines]] during cardiogenic shock, are [[interleukin-6]] and [[tumor necrosis factor]]. | ||
Besides the aforementioned macrocirculatory changes in cardiogenic shock, which may also be seen in [[septic shock]], it is important to mention that [[microcirculation|microcirculatory]] abnormalities, caused in part by the [[inflammatory]] cascades, play an important part in the [[pathogenesis]] of [[organ failure]] as well.<ref name="pmid14691425">{{cite journal| author=De Backer D, Creteur J, Dubois MJ, Sakr Y, Vincent JL| title=Microvascular alterations in patients with acute severe heart failure and cardiogenic shock. | journal=Am Heart J | year= 2004 | volume= 147 | issue= 1 | pages= 91-9 | pmid=14691425 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=14691425 }} </ref><ref name="pmid12091178">{{cite journal| author=De Backer D, Creteur J, Preiser JC, Dubois MJ, Vincent JL| title=Microvascular blood flow is altered in patients with sepsis. | journal=Am J Respir Crit Care Med | year= 2002 | volume= 166 | issue= 1 | pages= 98-104 | pmid=12091178 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=12091178 }} </ref><ref name="pmid17095120">{{cite journal| author=Trzeciak S, Dellinger RP, Parrillo JE, Guglielmi M, Bajaj J, Abate NL et al.| title=Early microcirculatory perfusion derangements in patients with severe sepsis and septic shock: relationship to hemodynamics, oxygen transport, and survival. | journal=Ann Emerg Med | year= 2007 | volume= 49 | issue= 1 | pages= 88-98, 98.e1-2 | pmid=17095120 | doi=10.1016/j.annemergmed.2006.08.021 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=17095120 }} </ref> | *[[IL-6]],is specific [[cytokine]] is correlated with the degree of [[organ failure]] and therefore [[mortality]].<ref name="pmid16775569">{{cite journal| author=Geppert A, Dorninger A, Delle-Karth G, Zorn G, Heinz G, Huber K| title=Plasma concentrations of interleukin-6, organ failure, vasopressor support, and successful coronary revascularization in predicting 30-day mortality of patients with cardiogenic shock complicating acute myocardial infarction. | journal=Crit Care Med | year= 2006 | volume= 34 | issue= 8 | pages= 2035-42 | pmid=16775569 | doi=10.1097/01.CCM.0000228919.33620.D9 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16775569 }} </ref> | ||
*These [[inflammatory]] mediators, among other actions, are responsible for the release of [[BNP]], which makes the levels of [[BNP]] good markers, not only for the level of [[inflammation]], but also to evaluate [[hemodynamic]] decompensation.<ref name="pmid16763507">{{cite journal| author=Rudiger A, Gasser S, Fischler M, Hornemann T, von Eckardstein A, Maggiorini M| title=Comparable increase of B-type natriuretic peptide and amino-terminal pro-B-type natriuretic peptide levels in patients with severe sepsis, septic shock, and acute heart failure. | journal=Crit Care Med | year= 2006 | volume= 34 | issue= 8 | pages= 2140-4 | pmid=16763507 | doi=10.1097/01.CCM.0000229144.97624.90 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16763507 }} </ref> | |||
*Other [[circulatory]] factors, such as [[procalcitonin]], [[complement]] and [[CRP]], have been reported in some studies to contribute to the development of [[SIRS]] in cardiogenic shock.<ref name="pmid12925454">{{cite journal| author=Granger CB, Mahaffey KW, Weaver WD, Theroux P, Hochman JS, Filloon TG et al.| title=Pexelizumab, an anti-C5 complement antibody, as adjunctive therapy to primary percutaneous coronary intervention in acute myocardial infarction: the COMplement inhibition in Myocardial infarction treated with Angioplasty (COMMA) trial. | journal=Circulation | year= 2003 | volume= 108 | issue= 10 | pages= 1184-90 | pmid=12925454 | doi=10.1161/01.CIR.0000087447.12918.85 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=12925454 }} </ref><ref name="pmid17200474">{{cite journal| author=APEX AMI Investigators. Armstrong PW, Granger CB, Adams PX, Hamm C, Holmes D et al.| title=Pexelizumab for acute ST-elevation myocardial infarction in patients undergoing primary percutaneous coronary intervention: a randomized controlled trial. | journal=JAMA | year= 2007 | volume= 297 | issue= 1 | pages= 43-51 | pmid=17200474 | doi=10.1001/jama.297.1.43 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=17200474 }} </ref> | |||
*Besides the aforementioned macrocirculatory changes in cardiogenic shock, which may also be seen in [[septic shock]], it is important to mention that [[microcirculation|microcirculatory]] abnormalities, caused in part by the [[inflammatory]] cascades, play an important part in the [[pathogenesis]] of [[organ failure]] as well.<ref name="pmid14691425">{{cite journal| author=De Backer D, Creteur J, Dubois MJ, Sakr Y, Vincent JL| title=Microvascular alterations in patients with acute severe heart failure and cardiogenic shock. | journal=Am Heart J | year= 2004 | volume= 147 | issue= 1 | pages= 91-9 | pmid=14691425 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=14691425 }} </ref><ref name="pmid12091178">{{cite journal| author=De Backer D, Creteur J, Preiser JC, Dubois MJ, Vincent JL| title=Microvascular blood flow is altered in patients with sepsis. | journal=Am J Respir Crit Care Med | year= 2002 | volume= 166 | issue= 1 | pages= 98-104 | pmid=12091178 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=12091178 }} </ref><ref name="pmid17095120">{{cite journal| author=Trzeciak S, Dellinger RP, Parrillo JE, Guglielmi M, Bajaj J, Abate NL et al.| title=Early microcirculatory perfusion derangements in patients with severe sepsis and septic shock: relationship to hemodynamics, oxygen transport, and survival. | journal=Ann Emerg Med | year= 2007 | volume= 49 | issue= 1 | pages= 88-98, 98.e1-2 | pmid=17095120 | doi=10.1016/j.annemergmed.2006.08.021 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=17095120 }} </ref> | |||
===Iatrogenic Cardiogenic Shock=== | ===Iatrogenic Cardiogenic Shock=== | ||
An important number of patients in cardiogenic shock complicating [[myocardial infarction]] (around 3/4), develop it after hospital admission.<ref name="pmid16046651">{{cite journal| author=Babaev A, Frederick PD, Pasta DJ, Every N, Sichrovsky T, Hochman JS et al.| title=Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock. | journal=JAMA | year= 2005 | volume= 294 | issue= 4 | pages= 448-54 | pmid=16046651 | doi=10.1001/jama.294.4.448 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16046651 }} </ref><ref name="Jeger2006">{{cite journal|last1=Jeger|first1=R. V.|title=Emergency revascularization in patients with cardiogenic shock on admission: a report from the SHOCK trial and registry|journal=European Heart Journal|volume=27|issue=6|year=2006|pages=664–670|issn=0195-668X|doi=10.1093/eurheartj/ehi729}}</ref> In some of these patients, it is reported that the development of [[shock]], particularly in high risk patients, is related to the use of certain classes of medications, used to treat the [[MI]]. These include:<ref name="pmid15976786">{{cite journal| author=Meine TJ, Roe MT, Chen AY, Patel MR, Washam JB, Ohman EM et al.| title=Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. | journal=Am Heart J | year= 2005 | volume= 149 | issue= 6 | pages= 1043-9 | pmid=15976786 | doi=10.1016/j.ahj.2005.02.010 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=15976786 }} </ref><ref name="pmid7661937">{{cite journal| author=| title=ISIS-4: a randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58,050 patients with suspected acute myocardial infarction. ISIS-4 (Fourth International Study of Infarct Survival) Collaborative Group. | journal=Lancet | year= 1995 | volume= 345 | issue= 8951 | pages= 669-85 | pmid=7661937 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=7661937 }} </ref><ref name="pmid9631869">{{cite journal| author=| title=Indications for ACE inhibitors in the early treatment of acute myocardial infarction: systematic overview of individual data from 100,000 patients in randomized trials. ACE Inhibitor Myocardial Infarction Collaborative Group. | journal=Circulation | year= 1998 | volume= 97 | issue= 22 | pages= 2202-12 | pmid=9631869 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=9631869 }} </ref><ref name="pmid16271643">{{cite journal| author=Chen ZM, Pan HC, Chen YP, Peto R, Collins R, Jiang LX et al.| title=Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. | journal=Lancet | year= 2005 | volume= 366 | issue= 9497 | pages= 1622-32 | pmid=16271643 | doi=10.1016/S0140-6736(05)67661-1 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16271643 }} [http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16646603 Review in: ACP J Club. 2006 May-Jun;144(3):58-9] [http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=17213104 Review in: Evid Based Med. 2006 Jun;11(3):82-3] </ref> | *An important number of patients in cardiogenic shock complicating [[myocardial infarction]] (around 3/4), develop it after hospital admission.<ref name="pmid16046651">{{cite journal| author=Babaev A, Frederick PD, Pasta DJ, Every N, Sichrovsky T, Hochman JS et al.| title=Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock. | journal=JAMA | year= 2005 | volume= 294 | issue= 4 | pages= 448-54 | pmid=16046651 | doi=10.1001/jama.294.4.448 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16046651 }} </ref><ref name="Jeger2006">{{cite journal|last1=Jeger|first1=R. V.|title=Emergency revascularization in patients with cardiogenic shock on admission: a report from the SHOCK trial and registry|journal=European Heart Journal|volume=27|issue=6|year=2006|pages=664–670|issn=0195-668X|doi=10.1093/eurheartj/ehi729}}</ref> | ||
*In some of these patients, it is reported that the development of [[shock]], particularly in high risk patients, is related to the use of certain classes of medications, used to treat the [[MI]]. These include:<ref name="pmid15976786">{{cite journal| author=Meine TJ, Roe MT, Chen AY, Patel MR, Washam JB, Ohman EM et al.| title=Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. | journal=Am Heart J | year= 2005 | volume= 149 | issue= 6 | pages= 1043-9 | pmid=15976786 | doi=10.1016/j.ahj.2005.02.010 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=15976786 }} </ref><ref name="pmid7661937">{{cite journal| author=| title=ISIS-4: a randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58,050 patients with suspected acute myocardial infarction. ISIS-4 (Fourth International Study of Infarct Survival) Collaborative Group. | journal=Lancet | year= 1995 | volume= 345 | issue= 8951 | pages= 669-85 | pmid=7661937 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=7661937 }} </ref><ref name="pmid9631869">{{cite journal| author=| title=Indications for ACE inhibitors in the early treatment of acute myocardial infarction: systematic overview of individual data from 100,000 patients in randomized trials. ACE Inhibitor Myocardial Infarction Collaborative Group. | journal=Circulation | year= 1998 | volume= 97 | issue= 22 | pages= 2202-12 | pmid=9631869 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=9631869 }} </ref><ref name="pmid16271643">{{cite journal| author=Chen ZM, Pan HC, Chen YP, Peto R, Collins R, Jiang LX et al.| title=Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. | journal=Lancet | year= 2005 | volume= 366 | issue= 9497 | pages= 1622-32 | pmid=16271643 | doi=10.1016/S0140-6736(05)67661-1 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16271643 }} [http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16646603 Review in: ACP J Club. 2006 May-Jun;144(3):58-9] [http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=17213104 Review in: Evid Based Med. 2006 Jun;11(3):82-3] </ref> | |||
*[[Beta-blockers]] | *[[Beta-blockers]] | ||
*[[ACE inhibitor]]s | *[[ACE inhibitor]]s | ||
*[[Morphine]] | *[[Morphine]] | ||
*[[Diuretics]] (As a cause or aggravating factor. This is due to the fact that [[pulmonary edema]] is a common [[complication]] of cardiogenic shock, leading to a decrease of circulating [[plasma]] volume, particularly in patients with prior [[heart failure]]. After the administration of high-dose [[diuretics]], the [[plasma]] volume will further decline) | *[[Diuretics]] (As a cause or aggravating factor. This is due to the fact that [[pulmonary edema]] is a common [[complication]] of cardiogenic shock, leading to a decrease of circulating [[plasma]] volume, particularly in patients with prior [[heart failure]]. | ||
*After the administration of high-dose [[diuretics]], the [[plasma]] volume will further decline) | |||
*Excess fluid administration (In the case of [[right ventricular myocardial infarction]], the excess volume loading in these patients may also contribute to the development of [[shock]]) | *Excess fluid administration (In the case of [[right ventricular myocardial infarction]], the excess volume loading in these patients may also contribute to the development of [[shock]]) | ||
==Histopathological Findings Of myocardial infarction and plaque rupture== | |||
http://www.peir.net Images courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] | |||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
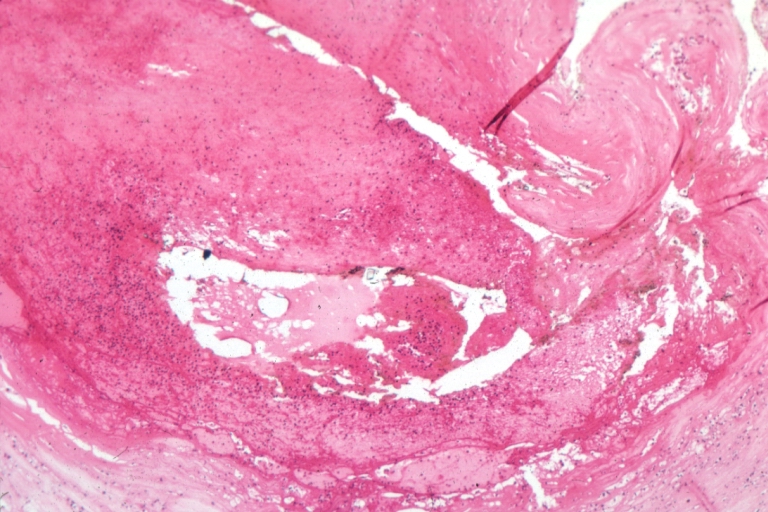
Image:Plaque rupture 1.jpg|Coronary artery: Atherosclerosis: Micro H&E med mag; A good example of plaque rupture with thrombosis. | |||
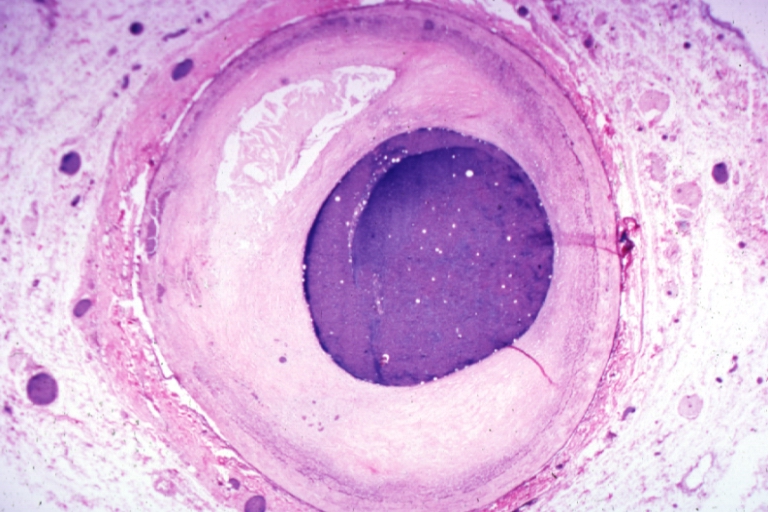
Image:Plaque rupture 2.jpg|Right coronary artery: Ruptured Plaque: Micro low mag H&E; Ruptured plaque with foam cell lesion (near rupture site). | |||
</gallery> | |||
</div> | |||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
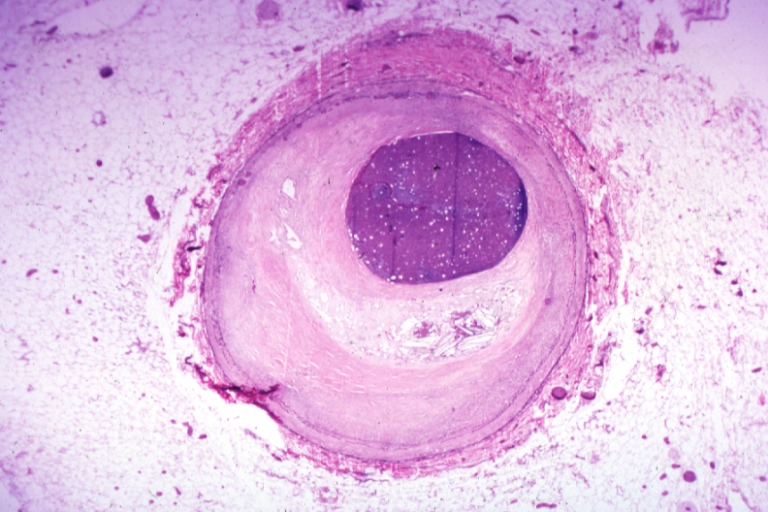
Image:Plaque rupture 3.jpg|Right coronary artery: Atherosclerosis Plaque Ruptured with Thrombus: Micro low mag H&E; an excellent view of ruptured plaque with thrombus and some old fibrin in it. | |||
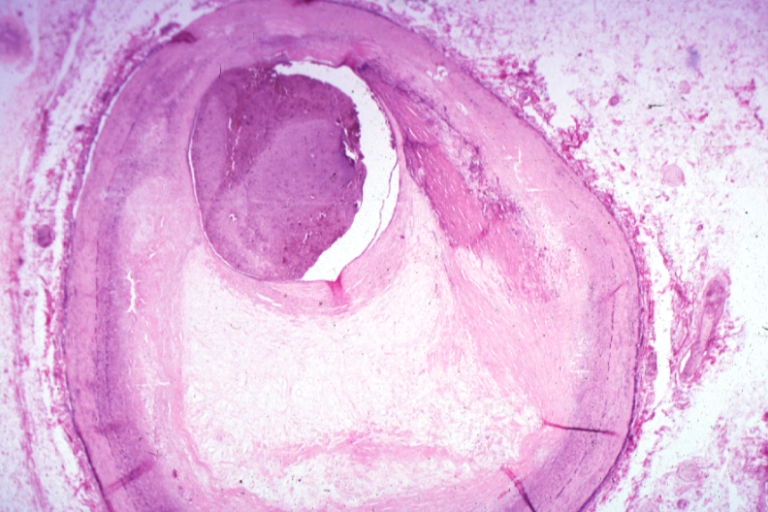
Image:Plaque rupture 4.jpg|Right coronary artery: Atherosclerosis Plaque Ruptured with Thrombus: Micro low mag trichrome. | |||
</gallery> | |||
</div> | |||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
Image:Plaque rupture 5.jpg|Right coronary artery: Atherosclerosis Plaque Ruptured: Micro low mag H&E; large plaque with hemorrhage; (an excellent example of hemorrhage). | |||
Image:Plaque 1.jpg|Coronary artery: Atherosclerosis: Micro H&E low mag injected artery fairly typical uncomplicated atheromatous plaque | |||
</gallery> | |||
</div> | |||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
Image:Plaque 2.jpg|Coronary artery: Atherosclerosis: Micro H&E low mag, injected artery has typical fibrous plaque with small hemorrhage in atheroma. | |||
Image:Plaque 3.jpg|Coronary artery: Atherosclerosis: Micro H&E low mag, injected artery is a very good example of marked lumen stenosis due to typical fibrous plaque with calcification | |||
</gallery> | |||
</div> | |||
==References== | ==References== | ||
Latest revision as of 00:57, 12 March 2020
|
Cardiogenic Shock Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Cardiogenic shock pathophysiology On the Web |
|
American Roentgen Ray Society Images of Cardiogenic shock pathophysiology |
|
Risk calculators and risk factors for Cardiogenic shock pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammad Salih, MD. João André Alves Silva, M.D. [2] Syed Musadiq Ali M.B.B.S.[3]
Overview
The pathophysiology of cardiogenic shock is complex and not fully understood. Ischemia to the myocardium causes derangement to both systolic and diastolic left ventricular function, resulting in a profound depression of myocardial contractility. This, in turn, leads to a potentially catastrophic and vicious spiral of reduced cardiac output and low blood pressure, perpetuating further coronary ischemia and impairment of contractility. Several physiologic compensatory processes ensue. These include:The activation of the sympathetic system leading to peripheral vasoconstriction which may improve coronary perfusion at the cost of increased afterload, and Tachycardia which increases myocardial oxygen demand and subsequently worsens myocardial ischemia.These compensatory mechanisms are subsequently counteracted by pathologic vasodilation that occurs from the release of potent systemic inflammatory markers such as interleukin-1, tumor necrosis factor a, and interleukin-6. Additionally, higher levels of nitric oxide and peroxynitrite are released, which also contribute to pathologic vasodilation and are known to be cardiotoxic. Unless interrupted by adequate treatment measures, this self-perpetuating cycle leads to global hypoperfusion and the inability to effectively meet the metabolic demands of the tissues, progressing to multiorgan failure and eventually death.
Pathophysiology
- The most common insult for cardiogenic shock is left ventricular pump failure in the setting of acute myocardial infarction.
- It usually takes a considerable area of infarcted myocardium (around 40%) to lead to cardiogenic shock.
- A smaller infarct may also originate this condition in a patient with a previously compromised ventricle function.
- There may also be other etiologies, other parts of the circulatory system may contribute, either alone or in combination, with inadequate compensation, or additional defects for this shock of cardiac origin, such as:[1]
- Systolic Left Ventricular Dysfunction - acute myocardial infarction, CHF, Cardiomyopathy, Coronary artery bypass grafting, Myocarditis, Myocardial contusion and Hypophosphatemia
- Diastolic Left Ventricular Dysfunction - Ischemia
- Obstruction of Left Ventricular Outflow, with Increased Afterload - Aortic stenosis, Hypertrophic Cardiomyopathy, Coarctation of the Aorta and Malignant Hypertension
- Reversal of flow into the left ventricle - Acute aortic insufficiency and endocarditis
- Inadequate left ventricular filling due to mechanical causes - Tamponade and pulmonary embolism
- Inadequate left ventricular filling due to inadequate filling time - Tachycardia and tachycardia-mediated cardiomyopathy
- Conduction abnormalities - Atrioventricular block and sinus bradycardia
- Mechanical defect - VSD and left ventricle free wall rupture
- Right ventricular failure - Pulmonary embolism and hypoxic pulmonary vasoconstriction[1]
The downward "Spiral" of Cardiogenic shock
- Cardiac dysfunction in patients with cardiogenic shock is usually initiated by myocardial infarction or ischemia.
- The myocardial dysfunction resulting from ischemia worsens that ischemia, creating a downward spiral.
- When a critical mass of left ventricular myocardium is ischemic or necrotic and fails to pump, stroke volume and cardiac output decrease.
- Myocardial perfusion, which depends on the pressure gradient between the coronary arterial system and the left ventricle.
- The duration of diastole, is compromised by hypotension and tachycardia. Which in turn, exacerbates ischemia.
- The increased ventricular diastolic pressures caused by pump failure further reduce coronary perfusion pressure, and the additional wall stress elevates myocardial oxygen requirements, further worsening ischemia.
- Decreased cardiac output also compromises systemic perfusion, which can lead to lactic acidosis and further compromise of systolic performance.
- The pathologic process begins with myocardial ischemia leading to an abnormal function of the cardiac muscle.
- This abnormality worsens the initial ischemia, which then deteriorates even further the ventricular function, creating the so called "downward spiral".[2]
- When ischemia reaches a point that the left ventricular myocardium fails to pump properly, parameters like stroke volume and cardiac output will therefore decrease.
- The pressure gradient produced between the pressure within the coronary arteries and the left ventricle, along with the duration of the diastole, dictate myocardial perfusion.
- This will be compromised by the hypotension and the tachycardia, worsening the myocardial ischemia and the perfusion of other vital organs.
- The fact that the heart is the only organ that benefits from a low blood pressure, as afterload decreases, makes these hemodynamical changes both beneficial and detrimental.
- The pump failure will then decrease the ability to push the blood out of the ventricle, thereby increasing the ventricular diastolic pressures.
- This will not only reduce the coronary perfusion pressure, as it will also increase the ventricle wall stress, so that the myocardial oxygen requirements will also raise, consequently propagating the ischemia.[2][1][3]
- cardiac pump failure and hypoperfusion of the peripheral tissues is that this last one, leads to the release of catecholamines.
- Catecholamines such as norepinephrine, will increase the heart's contractility and peripheral blood flow, by causing constriction of arterioles, together with angiotensin II, to maintain perfusion, however, this will also increase the heart's oxygen demand and have proarrhythmic and myocardiotoxic consequences.
- The increased SVR coupled with the low cardiac output will lead to an even more pronounced reduction of tissue perfusion.[1]
- The ischemia generated by all these processes increases the diastolic stiffness of the ventricle wall and this, along with the left ventricular dysfunction, will increase the left atrial pressure. The increased left atrial pressure will propagate through the pulmonary veins, generating pulmonary congestion, which by decreasing oxygen exchanges, leads to hypoxia.
- The hypoxia will further worsen the ischemia of the myocardium and the pulmonary congestion will propagate its effect through the pulmonary arteries to the right ventricle, hence jeopardizing its performance.
- Once myocardial function is affected, the body will put in motion compensatory mechanisms to try to increase the cardiac output. These include:[4]
- Tachycardia and increased contractility through sympathetic stimulation
- Activation of the renin/angiotensin/aldosterone system, leading to fluid retention and consequently increased preload
- These compensatory mechanisms eventually become maladaptive seeing that:[1][5]
- Tachycardia and increased contractility will increase cardiac muscle oxygen demand, thereby exacerbating the initial ischemia;
- Vasoconstriction, as a response to impaired cardiac output, in order to try to maintain coronary artery perfusion and systemic blood pressure (SVR) increases myocardial afterload, leading to an impairment in myocardial performance and an increase in its oxygen demand, worsening ischemia;
- The activation of the neurohormonal cascade will promote retention of water and sodium, in order to compensate for the hypotension and improve perfusion, yet this will also exacerbate pulmonary edema.
- The prolonged systemic hypoperfusion and hypoxia will cause a shift in cellular metabolism, prioritizing glycolysis, leading to a state of lactic acidosis, which jeopardizes contractility and systolic performance, thereby affecting the previously described system.
- All these factors affecting oxygen demand and cardiac performance create a vicious cycle that if not interrupted, may eventually lead to death.
- The therapeutic approach to cardiogenic shock focuses in disrupting this cycle.[6]
- The area of original infarct, remote territories may also exhibit some kind of myocardial damage, called myocardial stunning.
- Myocardial stunning is the name given the myocardium which remains dysfunctional even though the restoration to normal perfusion.
- The pathophysiology of myocardial stunning is multifactorial and involves calcium overload in the sarcolemma and diastolic dysfunction, as well as the release of myocardial depressant substances.
- This calcium overload is responsible for the activation of proteases called calpains. These and other proteases will be responsible for the degradation of myofilaments, which will decrease the response to calcium, thereby explaining the temporary myocardial dysfunction after reperfusion.
- Areas of stunned myocardium may remain stunned after revascularization due to the need to resynthetize new myofilaments.[7]
- These regions retain contractile reserve and usually respond to inotropic stimulation.
- Stunned myocardium, hibernating myocardium does respond earlier to revascularization since myocardial cells remain viable and when reperfused, calcium levels normalize.[8][9][10]
Right Ventricle Myocardial Infarction
- 5% of the cases but represents as high mortality rate as left ventricular shock.
- The right ventricular regions more commonly affected by infarction are the inferior and inferior-posterior walls.
- The coronary arteries frequently occluded in this setting are the right coronary artery, or the left circumflex coronary artery, in a left dominant system.[11][12] Patients with right coronary artery occlusion, in a right dominant system, are at higher risk of developing papillary muscle rupture and therefore undergoing valvular heart disease, such as mitral regurgitation.[12][13][14]
- Right ventricle failure may affect left ventricular performance by several means:[15][16]
- Decrease in right ventricular output leading to a decrease in left ventricular filling thereby affecting overall cardiac output;
- Increased right ventricular telediastolic pressure, leading to a shifting of the interventricular septum into the left ventricle, therefore jeopardizing left ventricular filling and systolic function.
Ventricular Septal and Free Wall Rupture
- Ventricular septal rupture and free wall rupture, which constitute two entities of cardiac rupture, represent the second most common cause of death in patients with acute myocardial infarction, during hospital stay.[17][18][19]
- Ventricular septal rupture in the SHOCK registry, it accounted for 4.6% of the cases of cardiogenic shock.[20]
- The most recent registries show that ventricular septal rupture generally develops within the first 16 to 24 hours post-MI and has the following characteristics:[21][22][23][24][25][12][26][12][27][28]
- According to the SHOCK trial data, this type of rupture had 55% of mortality rate within the first 30 days.[28] Free wall rupture may also be classified as simple or complex. It may occur either on the anterior or the lateral and posterior left ventricular walls.[28][17] These last two are thought to rupture easier, however, because of the higher proportion of anterior MIs, they are seen less frequently.[12]
- The rupture may present with different types of courses:
- Acute - the patient generally feels acute onset of chest pain, developing cardiac tamponade, hemodynamical collapse and sudden death. Because of the rapid course of this type, it is usually not controlled with current therapies.[29][30]
- Subacute - this type generally results in smaller and contained ruptures. These may be stabilized by the formation of a clot or fibrinous pericardial adhesions for a short period of time. Therapeutical measures must be applied urgently.[31][24]
- Chronic - less frequently associated with cardiogenic shock.
Inflammation and Hemodynamics
- Studies like the SHOCK trial show that not all patients follow this classic paradigm, since:[32][33][34]
- The range of elevation of systemic vascular resistance in this trial was wide, suggesting that the compensatory vasoconstriction wasn't a rule in every patient;
- The mean ejection fraction was also moderately decreased in this trial, showing that other mechanisms besides cardiac failure were present;
- Some of the patients had leukocytosis and fever, which along with the decreased systemic vascular resistance suggested SIRS.
- These facts have introduced the concept that myocardial infarction may cause SIRS and that inflammation plays an important part in the development and persistence of cardiogenic shock, contributing to myocardial dysfunction and vasodilation.
- The possibility of developing SIRS raises with the increasing permanence in cardiogenic shock.[1][35][36]
- At the time of the cardiac injury, the myocardium releases into circulation cytokines, particularly during the first 24 to 72 hours after the MI. *These will induce the enzyme nitric oxide synthase, thereby increasing the level of nitric oxide, which will be responsible for vasodilation and worsening of hypotension, further jeopardizing left ventricle performance.[37][38][39][40][41][42] NO may also form a toxic radical, called peroxynitrite, when combined with superoxide, affecting myocardial contractility.[43]
- Among these released cytokines during cardiogenic shock, are interleukin-6 and tumor necrosis factor.
- IL-6,is specific cytokine is correlated with the degree of organ failure and therefore mortality.[44]
- These inflammatory mediators, among other actions, are responsible for the release of BNP, which makes the levels of BNP good markers, not only for the level of inflammation, but also to evaluate hemodynamic decompensation.[45]
- Other circulatory factors, such as procalcitonin, complement and CRP, have been reported in some studies to contribute to the development of SIRS in cardiogenic shock.[46][47]
- Besides the aforementioned macrocirculatory changes in cardiogenic shock, which may also be seen in septic shock, it is important to mention that microcirculatory abnormalities, caused in part by the inflammatory cascades, play an important part in the pathogenesis of organ failure as well.[48][49][50]
Iatrogenic Cardiogenic Shock
- An important number of patients in cardiogenic shock complicating myocardial infarction (around 3/4), develop it after hospital admission.[51][52]
- In some of these patients, it is reported that the development of shock, particularly in high risk patients, is related to the use of certain classes of medications, used to treat the MI. These include:[53][54][55][56]
- Beta-blockers
- ACE inhibitors
- Morphine
- Diuretics (As a cause or aggravating factor. This is due to the fact that pulmonary edema is a common complication of cardiogenic shock, leading to a decrease of circulating plasma volume, particularly in patients with prior heart failure.
- After the administration of high-dose diuretics, the plasma volume will further decline)
- Excess fluid administration (In the case of right ventricular myocardial infarction, the excess volume loading in these patients may also contribute to the development of shock)
Histopathological Findings Of myocardial infarction and plaque rupture
http://www.peir.net Images courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology]
-
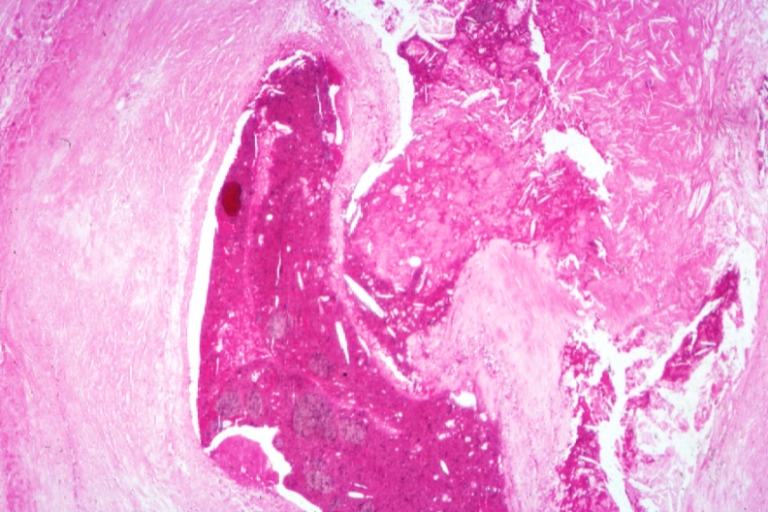
Coronary artery: Atherosclerosis: Micro H&E med mag; A good example of plaque rupture with thrombosis.
-
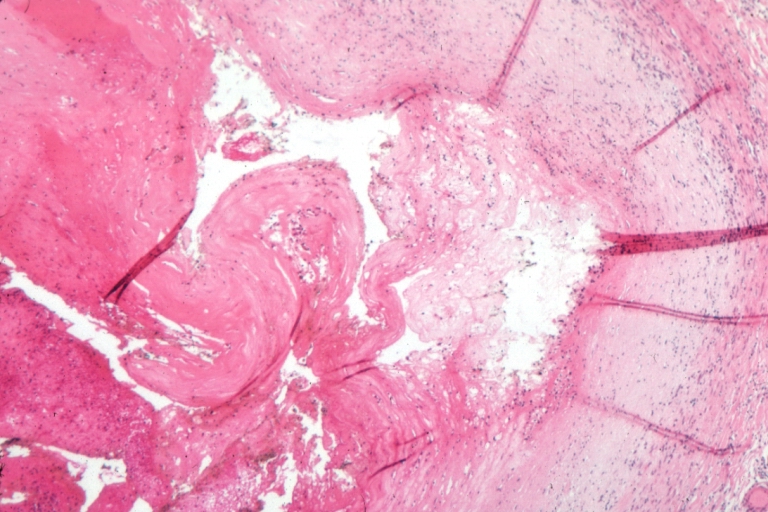
Right coronary artery: Ruptured Plaque: Micro low mag H&E; Ruptured plaque with foam cell lesion (near rupture site).


-
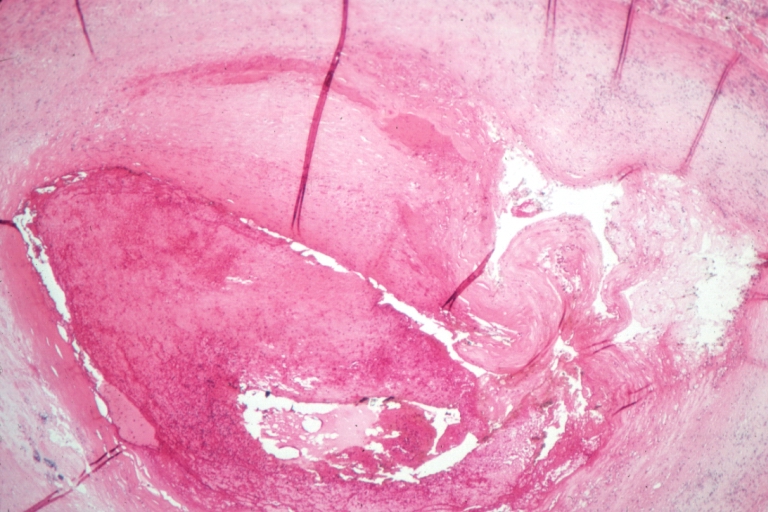
Right coronary artery: Atherosclerosis Plaque Ruptured with Thrombus: Micro low mag H&E; an excellent view of ruptured plaque with thrombus and some old fibrin in it.
-
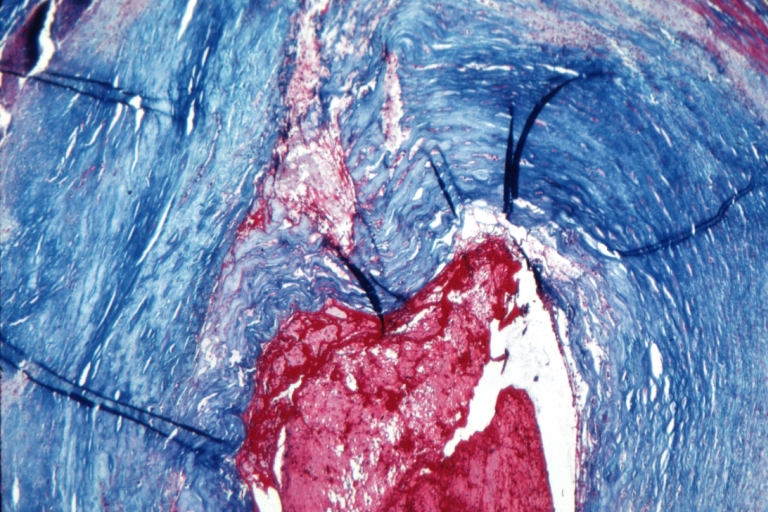
Right coronary artery: Atherosclerosis Plaque Ruptured with Thrombus: Micro low mag trichrome.


-
Right coronary artery: Atherosclerosis Plaque Ruptured: Micro low mag H&E; large plaque with hemorrhage; (an excellent example of hemorrhage).
-
Coronary artery: Atherosclerosis: Micro H&E low mag injected artery fairly typical uncomplicated atheromatous plaque


-
Coronary artery: Atherosclerosis: Micro H&E low mag, injected artery has typical fibrous plaque with small hemorrhage in atheroma.
-
Coronary artery: Atherosclerosis: Micro H&E low mag, injected artery is a very good example of marked lumen stenosis due to typical fibrous plaque with calcification


References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 Reynolds, H. R.; Hochman, J. S. (2008). "Cardiogenic Shock: Current Concepts and Improving Outcomes". Circulation. 117 (5): 686–697. doi:10.1161/CIRCULATIONAHA.106.613596. ISSN 0009-7322.
- ↑ 2.0 2.1 Hollenberg SM, Kavinsky CJ, Parrillo JE (1999). "Cardiogenic shock". Ann Intern Med. 131 (1): 47–59. PMID 10391815.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Bolli R, Marbán E (1999). "Molecular and cellular mechanisms of myocardial stunning". Physiol Rev. 79 (2): 609–34. PMID 10221990.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Bolli R (1998). "Basic and clinical aspects of myocardial stunning". Prog Cardiovasc Dis. 40 (6): 477–516. PMID 9647607.
- ↑ Marban E (1991). "Myocardial stunning and hibernation. The physiology behind the colloquialisms". Circulation. 83 (2): 681–8. PMID 1991384.
- ↑ Isner JM, Roberts WC (1978). "Right ventricular infarction complicating left ventricular infarction secondary to coronary heart disease. Frequency, location, associated findings and significance from analysis of 236 necropsy patients with acute or healed myocardial infarction". Am J Cardiol. 42 (6): 885–94. PMID 153103.
- ↑ 12.0 12.1 12.2 12.3 12.4 Ng, R.; Yeghiazarians, Y. (2011). "Post Myocardial Infarction Cardiogenic Shock: A Review of Current Therapies". Journal of Intensive Care Medicine. 28 (3): 151–165. doi:10.1177/0885066611411407. ISSN 0885-0666.
- ↑ Reeder GS (1995). "Identification and treatment of complications of myocardial infarction". Mayo Clin Proc. 70 (9): 880–4. doi:10.1016/S0025-6196(11)63946-3. PMID 7643642.
- ↑ Lavie CJ, Gersh BJ (1990). "Mechanical and electrical complications of acute myocardial infarction". Mayo Clin Proc. 65 (5): 709–30. PMID 2190052.
- ↑ Jacobs AK, Leopold JA, Bates E, Mendes LA, Sleeper LA, White H; et al. (2003). "Cardiogenic shock caused by right ventricular infarction: a report from the SHOCK registry". J Am Coll Cardiol. 41 (8): 1273–9. PMID 12706920.
- ↑ Brookes, C.; Ravn, H.; White, P.; Moeldrup, U.; Oldershaw, P.; Redington, A. (1999). "Acute Right Ventricular Dilatation in Response to Ischemia Significantly Impairs Left Ventricular Systolic Performance". Circulation. 100 (7): 761–767. doi:10.1161/01.CIR.100.7.761. ISSN 0009-7322.
- ↑ 17.0 17.1 Figueras J, Alcalde O, Barrabés JA, Serra V, Alguersuari J, Cortadellas J; et al. (2008). "Changes in hospital mortality rates in 425 patients with acute ST-elevation myocardial infarction and cardiac rupture over a 30-year period". Circulation. 118 (25): 2783–9. doi:10.1161/CIRCULATIONAHA.108.776690. PMID 19064683.
- ↑ Becker RC, Gore JM, Lambrew C, Weaver WD, Rubison RM, French WJ; et al. (1996). "A composite view of cardiac rupture in the United States National Registry of Myocardial Infarction". J Am Coll Cardiol. 27 (6): 1321–6. PMID 8626938.
- ↑ Becker RC, Hochman JS, Cannon CP, Spencer FA, Ball SP, Rizzo MJ; et al. (1999). "Fatal cardiac rupture among patients treated with thrombolytic agents and adjunctive thrombin antagonists: observations from the Thrombolysis and Thrombin Inhibition in Myocardial Infarction 9 Study". J Am Coll Cardiol. 33 (2): 479–87. PMID 9973029.
- ↑ Hochman JS, Buller CE, Sleeper LA, Boland J, Dzavik V, Sanborn TA; et al. (2000). "Cardiogenic shock complicating acute myocardial infarction--etiologies, management and outcome: a report from the SHOCK Trial Registry. SHould we emergently revascularize Occluded Coronaries for cardiogenic shocK?". J Am Coll Cardiol. 36 (3 Suppl A): 1063–70. PMID 10985706.
- ↑ Thompson CR, Buller CE, Sleeper LA, Antonelli TA, Webb JG, Jaber WA; et al. (2000). "Cardiogenic shock due to acute severe mitral regurgitation complicating acute myocardial infarction: a report from the SHOCK Trial Registry. SHould we use emergently revascularize Occluded Coronaries in cardiogenic shocK?". J Am Coll Cardiol. 36 (3 Suppl A): 1104–9. PMID 10985712.
- ↑ Crenshaw BS, Granger CB, Birnbaum Y, Pieper KS, Morris DC, Kleiman NS; et al. (2000). "Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial infarction. GUSTO-I (Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries) Trial Investigators". Circulation. 101 (1): 27–32. PMID 10618300.
- ↑ Radford MJ, Johnson RA, Daggett WM, Fallon JT, Buckley MJ, Gold HK; et al. (1981). "Ventricular septal rupture: a review of clinical and physiologic features and an analysis of survival". Circulation. 64 (3): 545–53. PMID 7020978.
- ↑ 24.0 24.1 Skehan JD, Carey C, Norrell MS, de Belder M, Balcon R, Mills PG (1989). "Patterns of coronary artery disease in post-infarction ventricular septal rupture". Br Heart J. 62 (4): 268–72. PMC 1277362. PMID 2803872.
- ↑ SWITHINBANK JM (1959). "Perforation of the interventricular septum in myocardial infarction". Br Heart J. 21: 562–6. PMC 1017615. PMID 13836145.
- ↑ Cohn, Lawrence (2012). Cardiac surgery in the adult. New York: McGraw-Hill Medical. ISBN 978-0-07-163310-9.
- ↑ Oliva PB, Hammill SC, Edwards WD (1993). "Cardiac rupture, a clinically predictable complication of acute myocardial infarction: report of 70 cases with clinicopathologic correlations". J Am Coll Cardiol. 22 (3): 720–6. PMID 8354804.
- ↑ 28.0 28.1 28.2 Slater J, Brown RJ, Antonelli TA, Menon V, Boland J, Col J; et al. (2000). "Cardiogenic shock due to cardiac free-wall rupture or tamponade after acute myocardial infarction: a report from the SHOCK Trial Registry. Should we emergently revascularize occluded coronaries for cardiogenic shock?". J Am Coll Cardiol. 36 (3 Suppl A): 1117–22. PMID 10985714.
- ↑ Figueras J, Cortadellas J, Soler-Soler J (2000). "Left ventricular free wall rupture: clinical presentation and management". Heart. 83 (5): 499–504. PMC 1760810. PMID 10768896.
- ↑ Cohn, Lawrence (2012). Cardiac surgery in the adult. New York: McGraw-Hill Medical. ISBN 007163312X.
- ↑ Cohn, Lawrence (2012). Cardiac surgery in the adult. New York: McGraw-Hill Medical. ISBN 007163312X.
- ↑ Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD; et al. (1999). "Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock". N Engl J Med. 341 (9): 625–34. doi:10.1056/NEJM199908263410901. PMID 10460813.
- ↑ Picard MH, Davidoff R, Sleeper LA, Mendes LA, Thompson CR, Dzavik V; et al. (2003). "Echocardiographic predictors of survival and response to early revascularization in cardiogenic shock". Circulation. 107 (2): 279–84. PMID 12538428.
- ↑ Kohsaka S, Menon V, Lowe AM, Lange M, Dzavik V, Sleeper LA; et al. (2005). "Systemic inflammatory response syndrome after acute myocardial infarction complicated by cardiogenic shock". Arch Intern Med. 165 (14): 1643–50. doi:10.1001/archinte.165.14.1643. PMID 16043684.
- ↑ Hochman, J. S. (2003). "Cardiogenic Shock Complicating Acute Myocardial Infarction: Expanding the Paradigm". Circulation. 107 (24): 2998–3002. doi:10.1161/01.CIR.0000075927.67673.F2. ISSN 0009-7322.
- ↑ Brunkhorst FM, Clark AL, Forycki ZF, Anker SD (1999). "Pyrexia, procalcitonin, immune activation and survival in cardiogenic shock: the potential importance of bacterial translocation". Int J Cardiol. 72 (1): 3–10. PMID 10636626.
- ↑ Hasdai, David. (2002). Cardiogenic shock : diagnosis and treatmen. Totowa, N.J.: Humana Press. ISBN 1-58829-025-5.
- ↑ Neumann, F.-J.; Ott, I.; Gawaz, M.; Richardt, G.; Holzapfel, H.; Jochum, M.; Schomig, A. (1995). "Cardiac Release of Cytokines and Inflammatory Responses in Acute Myocardial Infarction". Circulation. 92 (4): 748–755. doi:10.1161/01.CIR.92.4.748. ISSN 0009-7322.
- ↑ Shah, A (2000). "Inducible nitric oxide synthase and cardiovascular disease". Cardiovascular Research. 45 (1): 148–155. doi:10.1016/S0008-6363(99)00316-8. ISSN 0008-6363.
- ↑ Feng Q, Lu X, Jones DL, Shen J, Arnold JM (2001). "Increased inducible nitric oxide synthase expression contributes to myocardial dysfunction and higher mortality after myocardial infarction in mice". Circulation. 104 (6): 700–4. PMID 11489778.
- ↑ Cotter G, Kaluski E, Blatt A, Milovanov O, Moshkovitz Y, Zaidenstein R; et al. (2000). "L-NMMA (a nitric oxide synthase inhibitor) is effective in the treatment of cardiogenic shock". Circulation. 101 (12): 1358–61. PMID 10736276.
- ↑ Kaluski E, Hendler A, Blatt A, Uriel N (2006). "Nitric oxide synthase inhibitors in post-myocardial infarction cardiogenic shock--an update". Clin Cardiol. 29 (11): 482–8. PMID 17133844.
- ↑ Ferdinandy P, Danial H, Ambrus I, Rothery RA, Schulz R (2000). "Peroxynitrite is a major contributor to cytokine-induced myocardial contractile failure". Circ Res. 87 (3): 241–7. PMID 10926876.
- ↑ Geppert A, Dorninger A, Delle-Karth G, Zorn G, Heinz G, Huber K (2006). "Plasma concentrations of interleukin-6, organ failure, vasopressor support, and successful coronary revascularization in predicting 30-day mortality of patients with cardiogenic shock complicating acute myocardial infarction". Crit Care Med. 34 (8): 2035–42. doi:10.1097/01.CCM.0000228919.33620.D9. PMID 16775569.
- ↑ Rudiger A, Gasser S, Fischler M, Hornemann T, von Eckardstein A, Maggiorini M (2006). "Comparable increase of B-type natriuretic peptide and amino-terminal pro-B-type natriuretic peptide levels in patients with severe sepsis, septic shock, and acute heart failure". Crit Care Med. 34 (8): 2140–4. doi:10.1097/01.CCM.0000229144.97624.90. PMID 16763507.
- ↑ Granger CB, Mahaffey KW, Weaver WD, Theroux P, Hochman JS, Filloon TG; et al. (2003). "Pexelizumab, an anti-C5 complement antibody, as adjunctive therapy to primary percutaneous coronary intervention in acute myocardial infarction: the COMplement inhibition in Myocardial infarction treated with Angioplasty (COMMA) trial". Circulation. 108 (10): 1184–90. doi:10.1161/01.CIR.0000087447.12918.85. PMID 12925454.
- ↑ APEX AMI Investigators. Armstrong PW, Granger CB, Adams PX, Hamm C, Holmes D; et al. (2007). "Pexelizumab for acute ST-elevation myocardial infarction in patients undergoing primary percutaneous coronary intervention: a randomized controlled trial". JAMA. 297 (1): 43–51. doi:10.1001/jama.297.1.43. PMID 17200474.
- ↑ De Backer D, Creteur J, Dubois MJ, Sakr Y, Vincent JL (2004). "Microvascular alterations in patients with acute severe heart failure and cardiogenic shock". Am Heart J. 147 (1): 91–9. PMID 14691425.
- ↑ De Backer D, Creteur J, Preiser JC, Dubois MJ, Vincent JL (2002). "Microvascular blood flow is altered in patients with sepsis". Am J Respir Crit Care Med. 166 (1): 98–104. PMID 12091178.
- ↑ Trzeciak S, Dellinger RP, Parrillo JE, Guglielmi M, Bajaj J, Abate NL; et al. (2007). "Early microcirculatory perfusion derangements in patients with severe sepsis and septic shock: relationship to hemodynamics, oxygen transport, and survival". Ann Emerg Med. 49 (1): 88–98, 98.e1–2. doi:10.1016/j.annemergmed.2006.08.021. PMID 17095120.
- ↑ Babaev A, Frederick PD, Pasta DJ, Every N, Sichrovsky T, Hochman JS; et al. (2005). "Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock". JAMA. 294 (4): 448–54. doi:10.1001/jama.294.4.448. PMID 16046651.
- ↑ Jeger, R. V. (2006). "Emergency revascularization in patients with cardiogenic shock on admission: a report from the SHOCK trial and registry". European Heart Journal. 27 (6): 664–670. doi:10.1093/eurheartj/ehi729. ISSN 0195-668X.
- ↑ Meine TJ, Roe MT, Chen AY, Patel MR, Washam JB, Ohman EM; et al. (2005). "Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative". Am Heart J. 149 (6): 1043–9. doi:10.1016/j.ahj.2005.02.010. PMID 15976786.
- ↑ "ISIS-4: a randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58,050 patients with suspected acute myocardial infarction. ISIS-4 (Fourth International Study of Infarct Survival) Collaborative Group". Lancet. 345 (8951): 669–85. 1995. PMID 7661937.
- ↑ "Indications for ACE inhibitors in the early treatment of acute myocardial infarction: systematic overview of individual data from 100,000 patients in randomized trials. ACE Inhibitor Myocardial Infarction Collaborative Group". Circulation. 97 (22): 2202–12. 1998. PMID 9631869.
- ↑ Chen ZM, Pan HC, Chen YP, Peto R, Collins R, Jiang LX; et al. (2005). "Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial". Lancet. 366 (9497): 1622–32. doi:10.1016/S0140-6736(05)67661-1. PMID 16271643. Review in: ACP J Club. 2006 May-Jun;144(3):58-9 Review in: Evid Based Med. 2006 Jun;11(3):82-3