Pancreatic cancer CT
|
Pancreatic cancer Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Pancreatic cancer CT On the Web |
|
American Roentgen Ray Society Images of Pancreatic cancer CT |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2];Parminder Dhingra, M.D. [3];Faizan Sheraz, M.D. [4]
Overview
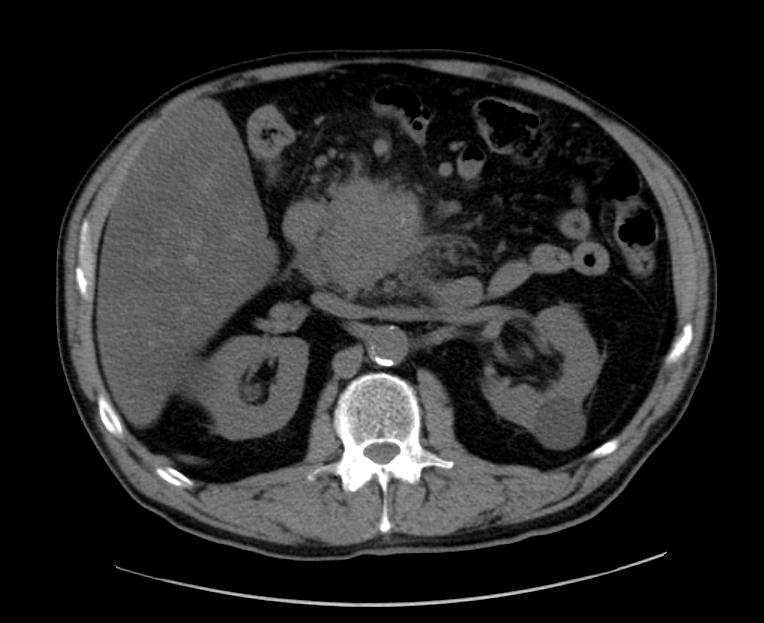
On abdominal CT scan, pancreatic cancer appears as a poorly defined mass with surrounding desmoplastic reaction.
CT
Pancreatic Adenocarcinoma
Typically ductal adenocarcinomas appear as poorly defined masses with extensive surrounding desmoplastic reaction. They enhance poorly compared to adjacent normal pancreatic tissue and thus appear hypodense on arterial phase scans in 75-90% of cases, but may become isodense on delayed scans (thus the need for multiple phase scanning when pancreatic cancer is the clinical question). Double duct sign may be seen. CT correlates well with surgical findings in predicting unresectablitly (positive predictive value of 89-100%). The most important feature to assess locally is the relationship of the tumour to surrounding vessels (SMA and coeliac axis). If the tumour surrounds a vessel by more than 180 degrees then it is deemed T4 disease and is unresectable.[1]
-
Pancreatic adenocarcinoma
-

Pancreatic adenocarcinoma
-

Pancreatic adenocarcinoma



References
- ↑ Pancreatic ductal carcinoma. Dr Ahmed Abd Rabou and Dr Frank Gaillard et al. Radiopedia.org 2015. http://radiopaedia.org/articles/pancreatic-ductal-carcinoma