Coronary artery bypass surgery conduits used for bypass: Difference between revisions
| Line 36: | Line 36: | ||
* [[Chronic pain]] at incision sites | * [[Chronic pain]] at incision sites | ||
== | ==Conduit nomenclature== | ||
The terms ''single bypass'', ''double bypass'', ''triple bypass'', ''quadruple bypass'' and ''quintuple bypass'' refer to the number of coronary arteries bypassed in the procedure. | The terms ''single bypass'', ''double bypass'', ''triple bypass'', ''quadruple bypass'' and ''quintuple bypass'' refer to the number of coronary arteries bypassed in the procedure. | ||
Revision as of 14:41, 12 September 2011
|
Coronary Artery Bypass Surgery Microchapters | |
|
Pathophysiology | |
|---|---|
|
Diagnosis | |
|
Treatment | |
|
Perioperative Monitoring | |
|
Surgical Procedure | |
|
Special Scenarios | |
|
Coronary artery bypass surgery conduits used for bypass On the Web | |
|
FDA on Coronary artery bypass surgery conduits used for bypass | |
|
CDC on Coronary artery bypass surgery conduits used for bypass | |
|
Coronary artery bypass surgery conduits used for bypass in the news | |
|
Blogs on Coronary artery bypass surgery conduits used for bypass|- |
|
|
Directions to Hospitals Performing Coronary artery bypass surgery conduits used for bypass | |
|
Risk calculators for Coronary artery bypass surgery conduits used for bypass | |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-in-Chief: Cafer Zorkun, M.D., Ph.D. [2], Mohammed A. Sbeih, M.D. [3]
Conduits used for bypass
The choice of conduits (arteries and/or veins from elsewhere in the body) to bypass the blockages is highly surgeon and institution dependent. Typically, the left internal thoracic artery (LITA) (also referred to as the left internal mammary artery or LIMA) is grafted to the Left Anterior Descending artery and a combination of other arteries and veins is used for other coronary arteries. The right internal thoracic artery (RITA), the great saphenous vein from the leg and the radial artery from the forearm are frequently used. The right gastroepiploic artery from the stomach is infrequently used given the difficult mobilization from the abdomen.
Saphenous vein
- Saphenous vein anatomy
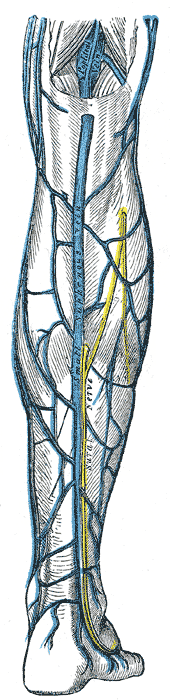
The great saphenous vein (GSV) is frequently used as a conduit for CABG. It originates from where the dorsal vein of the first digit (the large toe) merges with the dorsal venous arch of the foot.
After passing anterior to the medial malleolus (where it often can be visualized and palpated), it runs up the medial side of the leg. At the knee, it runs over the posterior border of the medial epicondyle of the femur bone.
The great saphenous vein then courses laterally to lie on the anterior surface of the thigh before entering an opening in the fascia lata called the saphenous opening. It joins with the femoral vein in the region of the femoral triangle at the saphenofemoral junction.
The small saphenous vein (also lesser saphenous vein) originates where the dorsal vein from the fifth digit (smallest toe) merges with the dorsal venous arch of the foot, which attaches to the great saphenous vein. It is considered a superficial vein and is subcutaneous (just under the skin). From its origin, it courses around the lateral aspect of the foot (inferior and posterior to the lateral malleolus) and runs along the posterior aspect of the leg (with the sural nerve), passes between the heads of the gastrocnemius muscle, and drains into the popliteal vein, approximately at or above the level of the knee joint.
-
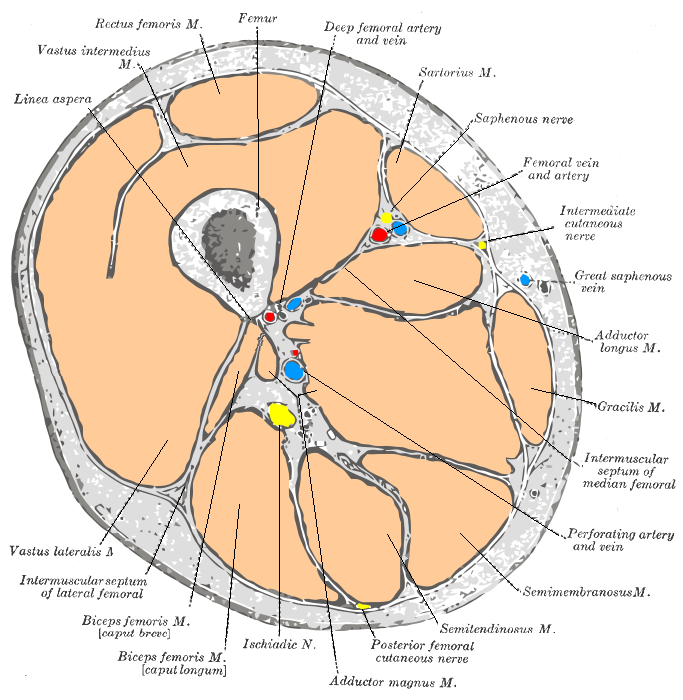
Cross-section through the middle of the thigh.
-
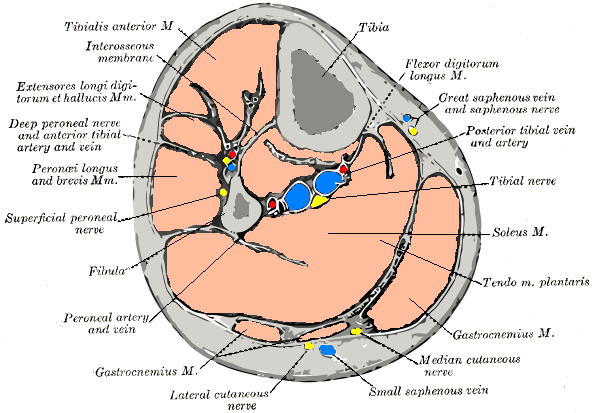
Cross-section through middle of leg.
-
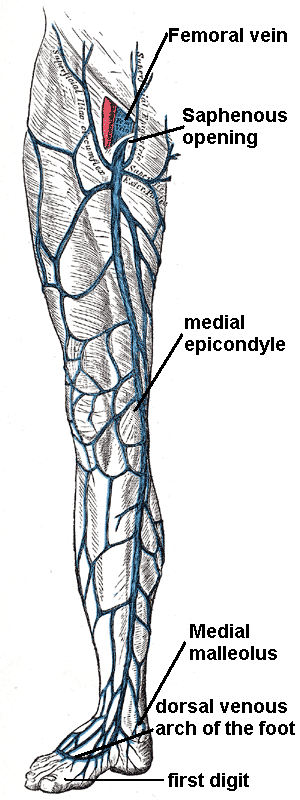
The great saphenous vein and landmarks along its course
-
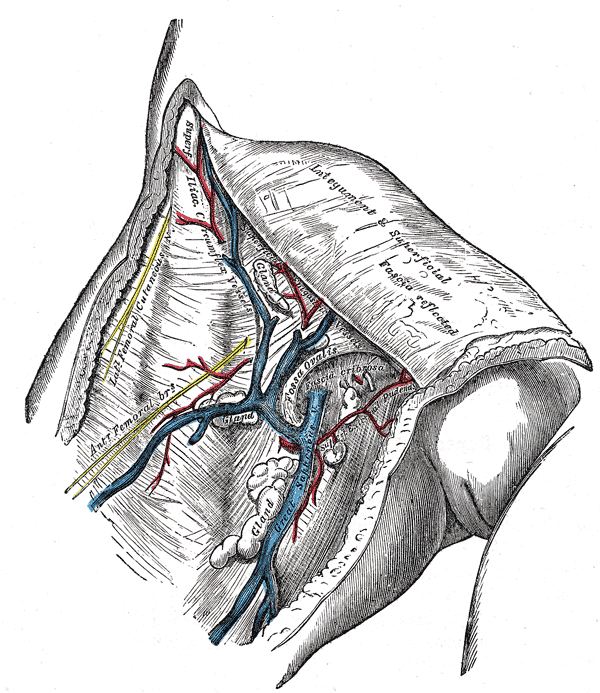
The great saphenous vein and its tributaries at the fossa ovalis in the groin.
-
Small saphenous vein and its tributaries.



- Saphenous vein harvesting
The saphenous vein can be harvested by either direct visualization or via an endoscopic approach. Veins that are used either have their valves removed or are turned around so that the valves in them do not occlude blood flow in the graft. The technique of saphenous vein harvesting may influence later SVG patency. The process of harvesting the vein and pressure testing the vein for a leak may damage the endothelium.[1][2]
The endoscopic approach has been associated with lower rates of wound infection, greater patient satisfaction, and earlier mobilization.[3][4][5][6] One small randomized study of 144 patients showed no difference in histologic findings between the traditional and endoscopic techniques.[3]In another small study of 40 patients randomized to the two techniques, no difference was seen in angiographic patency at 3 months.[6]Another small randomized study of 144 patients who returned for angiography demonstrated an occlusion rate of 21.7% for the endoscopic approach vs 17.6% for the open approach.[5] However, non- randomized data from a much larger multicenter study does suggest that endoscopic harvesting may be associated with higher rates of failure and adverse events such as death and MI.[4]
Complications associated with saphenous vein harvesting include the following:
- Saphenous nerve injury
- Infection at incision sites or sepsis.
- Deep vein thrombosis (DVT)
- Keloid scarring
- Chronic pain at incision sites
Conduit nomenclature
The terms single bypass, double bypass, triple bypass, quadruple bypass and quintuple bypass refer to the number of coronary arteries bypassed in the procedure.
In other words, a double bypass means two coronary arteries are bypassed (e.g. the left anterior descending (LAD) coronary artery and right coronary artery (RCA)); a triple bypass means three vessels are bypassed (e.g. LAD, RCA, left circumflex artery (LCX)); a quadruple bypass means four vessels are bypassed (e.g. LAD, RCA, LCX, first diagonal artery of the LAD) while quintuple means five. Less commonly more than four coronary arteries may be bypassed.
A greater number of bypasses does not imply a person is "sicker," nor does a lesser number imply a person is "healthier."[7] A person with a large amount of coronary artery disease (CAD) may receive fewer bypass grafts owing to the lack of suitable "target" vessels.
A patient with a single stenosis ("narrowing") of the left main coronary artery often requires only two bypasses (to the LAD and the LCX). However, depending upon the anatomy, grafts may also need to be placed to a large diagonal artery, or to additional large obtuse marginal branches.
Assessment of target vessels for bypass grafting
A coronary artery may be unsuitable for bypass grafting for the following reasons:
- Size: If the native target artery it is small (< 1 mm or < 1.5 mm depending on surgeon preference)
- Location: Some distal locations of the native target artery may not be accessible, or a conduit may not reach the far down the native artery.
- Native artery calcification: Heavily calcified native arteries are sometimes technically not amenable to anastamosis of a conduit.
- Diffuse disease: The native artery may not have a section of vessel that has minimal disease where a conduit can be grafted to.
- The native artery lies in the heart muscle or is intramyocardial: In this scenario the native coronary artery is located within the heart muscle rather than on the surface of the heart and a graft cannot be attached to it.
Although the cardiothoracic surgeon reviews the coronary angiogram prior to surgery and identifies the lesions (or "blockages") in the coronary arteries and will estimate the number of bypass grafts prior to surgery, the final decision is made in the operating room based upon the direct examination of the heart and the suitability of the native target vessel for bypassing.
References
- ↑ Lawrie GM, Weilbacher DE, Henry PD. Endothelium-dependent relaxation in human saphenous vein grafts. Effects of preparation and clinicopathologic correlations. J Thorac Cardiovasc Surg 1990;100:612—20.
- ↑ Souza DS, Johansson B, Bojo¨ L, Karlsson R, Geijer H, Filbey D, Bodin L, Arbeus M, Dashwood MR. Harvesting the saphenous vein with surrounding tissue for CABG provides long-term graft patency comparable to the left internal thoracic artery: results of a randomized longitudinal trial. J Thorac Cardiovasc Surg 2006;132:373—8.
- ↑ 3.0 3.1 Kiaii B, Moon BC, Massel D, Langlois Y, Austin TW, Willoughby A, Guiraudon C, Howard CR, Guo LR (2002). "A prospective randomized trial of endoscopic versus conventional harvesting of the saphenous vein in coronary artery bypass surgery". J. Thorac. Cardiovasc. Surg. 123 (2): 204–12. PMID 11828277. Retrieved 2010-07-23. Unknown parameter
|month=ignored (help) - ↑ 4.0 4.1 Lopes RD, Hafley GE, Allen KB, Ferguson TB, Peterson ED, Harrington RA, Mehta RH, Gibson CM, Mack MJ, Kouchoukos NT, Califf RM, Alexander JH (2009). "Endoscopic versus open vein-graft harvesting in coronary-artery bypass surgery". The New England Journal of Medicine. 361 (3): 235–44. doi:10.1056/NEJMoa0900708. PMID 19605828. Retrieved 2010-07-12. Unknown parameter
|month=ignored (help) - ↑ 5.0 5.1 Yun KL, Wu Y, Aharonian V, Mansukhani P, Pfeffer TA, Sintek CF, Kochamba GS, Grunkemeier G, Khonsari S (2005). "Randomized trial of endoscopic versus open vein harvest for coronary artery bypass grafting: six-month patency rates". J. Thorac. Cardiovasc. Surg. 129 (3): 496–503. doi:10.1016/j.jtcvs.2004.08.054. PMID 15746730. Retrieved 2010-07-23. Unknown parameter
|month=ignored (help) - ↑ 6.0 6.1 Perrault LP, Jeanmart H, Bilodeau L, Lespérance J, Tanguay JF, Bouchard D, Pagé P, Carrier M (2004). "Early quantitative coronary angiography of saphenous vein grafts for coronary artery bypass grafting harvested by means of open versus endoscopic saphenectomy: a prospective randomized trial". J. Thorac. Cardiovasc. Surg. 127 (5): 1402–7. doi:10.1016/j.jtcvs.2003.10.040. PMID 15115999. Retrieved 2010-07-23. Unknown parameter
|month=ignored (help) - ↑ Ohki S, Kaneko T, Satoh Y; et al. (2002). "[Coronary artery bypass grafting in octogenarian]". Kyobu geka. The Japanese journal of thoracic surgery (in Japanese). 55 (10): 829–33, discussion 833–6. PMID 12233100.