Clubbing
| Clubbing | |
 | |
|---|---|
| Clubbing in the fingers of a 33-year old female with pulmonary hypertension. | |
| ICD-10 | R68.3 |
| ICD-9 | 781.5 |
|
WikiDoc Resources for Clubbing |
|
Articles |
|---|
|
Most recent articles on Clubbing |
|
Media |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Clubbing at Clinical Trials.gov Clinical Trials on Clubbing at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Clubbing
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Directions to Hospitals Treating Clubbing Risk calculators and risk factors for Clubbing
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Clubbing |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [2] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Overview
In medicine, clubbing, finger clubbing, or digital clubbing is a deformity of the fingers and fingernails that is associated with a number of diseases, mostly of the heart and lungs. Idiopathic clubbing can also occur. Hippocrates was probably the first to document clubbing as a sign of disease, and the phenomenon is therefore occasionally called Hippocratic fingers.
Epidemiology
The exact frequency of clubbing in the population is not known. A 2008 study found clubbing in 1% of all patients admitted to a department of internal medicine. Of these, 40% turned out to have significant underlying disease of various causes, while 60% had no medical problems on further investigations and remained well over the subsequent year.[1]
Pathophysiology
The exact cause for sporadic clubbing is unknown, and there are numerous theories as to its cause. Vasodilation (distended blood vessels), secretion of growth factors (such as platelet-derived growth factor and hepatocyte growth factor) from the lungs, and other mechanisms have been proposed. The discovery of disorders in the prostaglandin metabolism in primary osteo-arthropathy has led to suggestions that overproduction of PGE2 by other tissues may be the causative factor for clubbing.[2]
Diagnosis
Signs and symptoms
Clubbing develops in five steps:[3]
- Fluctuation and softening of the nail bed (increased ballotability)
- Loss of the normal <165° angle ("Lovibond angle") between the nailbed and the fold (cuticula)
- Increased convexity of the nail fold
- Thickening of the whole distal (end part of the) finger (resembling a drumstick)
- Shiny aspect and striation of the nail and skin
Schamroth's test or Schamroth's window test (originally demonstrated by South African cardiologist Dr Leo Schamroth on himself[4]) is a popular test for clubbing. When the distal phalanges (bones nearest the fingertips) of corresponding fingers of opposite hands are directly apposed (placed against each other back to back), a small diamond-shaped "window" is normally apparent between the nailbeds. If this window is obliterated, the test is positive and clubbing is present.
When clubbing is encountered in patients, doctors will seek to identify its cause. They usually accomplish this by obtaining a medical history— particular attention is paid to lung, heart, and gastrointestinal conditions —and conducting a clinical examination, which may disclose associated features relevant to a diagnosis. Additional studies such as a chest x-ray may also be performed.
-
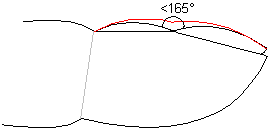
Clubbing of the fingernail. The red line shows the outline of a clubbed nail.

Physical Examination
Extremities

Disease associations
Although many diseases are associated with clubbing (particularly lung diseases), the reports are fairly anecdotal. Prospective studies of patients presenting with clubbing have not yet been performed, and hence there is no conclusive evidence of these associations.
Isolated clubbing
Clubbing is associated with:
- Lung disease:
- Lung cancer, mainly large-cell (35% of all cases), not seen frequently in small cell lung cancer[6]
- Interstitial lung disease
- Tuberculosis
- Bronchiectasis
- Suppurative lung disease: lung abscess, empyema
- Cystic fibrosis
- Pulmonary hypertension
- Mesothelioma
- It is worth noting that clubbing is not associated with chronic obstructive pulmonary disease (COPD). Indeed, the presence of clubbing in a patient with COPD should prompt a search for an underlying (lung) cancer.
- Heart disease:
- Any disease featuring chronic hypoxia
- Congenital cyanotic heart disease (most common cardiac cause)
- Subacute bacterial endocarditis
- Atrial myxoma (benign tumor)
- Gastrointestinal and hepatobiliary:
- Malabsorption
- Crohn's disease and ulcerative colitis
- Cirrhosis, especially in primary biliary cirrhosis[7]
- Other liver diseases (in the "hepatopulmonary syndrome", a complication of cirrhosis)[8]
- Others:
- Hyperthyroidism (thyroid acropachy)[9]
- Familial and racial clubbing and "pseudoclubbing" (people of African descent often have what appears to be clubbing)
- Vascular anomalies of the affected arm such as an axillary artery aneurysm (in unilateral clubbing)
Clubbing associated with other symptoms
HPOA

A special form of clubbing is hypertrophic pulmonary osteo-arthropathy, known in continental Europe as Pierre Marie-Bamberger syndrome. (In dogs the condition is known as hypertrophic osteopathy.) This is the combination of clubbing and thickening of periosteum (connective tissue lining of the bones) and synovium (lining of joints), and is often initially diagnosed as arthritis. It is commonly associated with lung cancer.
Primary HOA
Primary hypertrophic osteo-arthropathy is HPOA without signs of pulmonary disease. This form has a hereditary component, although subtle cardiac abnormalties can occasionally be found. It is known in continental Europe as the Touraine-Solente-Golé syndrome. This condition has been linked to mutations in the gene on the fourth chromosome (4q33-q34)coding for the enzyme 15-hydroxyprostaglandin dehydrogenase (HPGD); this leads to decreased breakdown of prostaglandin E2 and elevated levels of this substance.[10]
Secondary HOA
It is usually associated with lung cancer, pulmonary infections, cystic fibrosis, right-to-left cardiac shunts, and less often in Hodgkin lymphoma and cirrhosis.
Among patients with lung cancer, HOA is most frequently associated with adenocarcinoma and least frequently with small cell carcinoma. In one series of 111 consecutive patients with pathologically proven lung cancer, clubbing was present in 29 percent; clubbing was more common among women than men (40 versus 19 percent) and in non-small cell compared to small cell lung cancer (35 versus 4 percent) [12].
Clinical features of HOA include digital clubbing (show figure 1), periostosis of tubular bones (show radiograph 1A-1B), and synovial effusions, which are most prominent in the large joints. Periostosis is usually accompanied by pain on palpation of the involved area. Some patients present with a painful arthropathy in advance of clubbing, and may be thought to have an inflammatory arthritis [13].
Rarely, arterial vascular prosthesis infections may be associated with HOA [14]. Clinical features suggestive of vascular infection-related HOA include clubbing or periosteal new bone formation in a single limb (in the case of upper extremity arterial prostheses), or unilateral or bilateral lower extremity involvement in the case of arterial grafts to the legs or aortic prostheses.
When HOA is suspected, attention should be paid to the chest because the most frequent cause of acute onset of HOA is a lung neoplasm, either primary or secondary. A bone scan is a sensitive way to detect which bones are involved. Removal of lung cancer or treatment of the other causes of HOA results in regression in the clinical manifestations [13].
See also
- Periosteal reaction for more on HPOA and primary HOA
- clubbed thumb
Complete Differential Diagnosis of the Causes of Clubbing
(In alphabetical order)
- Arteriovenous malformations
- Bronchial carcinomas
- Bronchiectasis
- Celiac Sprue
- Cerebrovascular insult
- Chronic obstructive jaundice
- Cirrhosis
- Cyanotic congenital heart disease
- Cystic Fibrosis
- Emphysema
- Empyema
- Endocarditis
- Heart failure
- Hepatoma
- Hodgkin's lymphoma
- Liver tumors
- Lung abscess
- Mesothelioma
- Pachydermoperiostosis
- Pulmonic stenosis
- Pulmonary fibrosis
- Pulmonary metastases
- Right-to-left cardiac shunts
- Silicosis
- Thyrotoxicosis
- Tuberculosis
- Ulcerative colitis
Complete Differential Diagnosis of the Causes of Clubbing
(By organ system)
| Cardiovascular | No underlying causes |
| Chemical / poisoning | No underlying causes |
| Dermatologic | No underlying causes |
| Drug Side Effect | No underlying causes |
| Ear Nose Throat | No underlying causes |
| Endocrine | No underlying causes |
| Environmental | No underlying causes |
| Gastroenterologic | No underlying causes |
| Genetic | No underlying causes |
| Hematologic | No underlying causes |
| Iatrogenic | No underlying causes |
| Infectious Disease | No underlying causes |
| Musculoskeletal / Ortho | No underlying causes |
| Neurologic | No underlying causes |
| Nutritional / Metabolic | No underlying causes |
| Obstetric/Gynecologic | No underlying causes |
| Oncologic | No underlying causes |
| Opthalmologic | No underlying causes |
| Overdose / Toxicity | No underlying causes |
| Psychiatric | No underlying causes |
| Pulmonary | No underlying causes |
| Renal / Electrolyte | No underlying causes |
| Rheum / Immune / Allergy | No underlying causes |
| Sexual | No underlying causes |
| Trauma | No underlying causes |
| Urologic | No underlying causes |
| Miscellaneous | No underlying causes |
References
- ↑ Vandemergel X, Renneboog B (2008). "Prevalence, aetiologies and significance of clubbing in a department of general internal medicine". Eur. J. Intern. Med. 19 (5): 325–9. doi:10.1016/j.ejim.2007.05.015. PMID 18549933. Unknown parameter
|month=ignored (help) - ↑ Uppal S, Diggle CP, Carr IM, et al (June 2008). "Mutations in 15-hydroxyprostaglandin dehydrogenase cause primary hypertrophic osteoarthropathy". Nat. Genet. 40 (6): 789–93. doi:10.1038/ng.153. PMID 18500342
- ↑ Myers KA, Farquhar DR (2001). "The rational clinical examination: does this patient have clubbing?". JAMA. 286: 341–7. doi:10.1001/jama.286.3.341. PMID 11466101.
- ↑ Schamroth L (1976). "Personal experience". S. Afr. Med. J. 50 (9): 297–300. PMID 1265563. Unknown parameter
|month=ignored (help) - ↑ http://picasaweb.google.com/mcmumbi/USMLEIIImages
- ↑ Sridhar KS, Lobo CF, Altman RD. Digital clubbing and lung cancer. Chest 1998;114:1535-37. PMID 9872183
- ↑ Epstein O, Dick R, Sherlock S (1981). "Prospective study of periostitis and finger clubbing in primary biliary cirrhosis and other forms of chronic liver disease". Gut. 22 (3): 203–6. PMID 7227854.
- ↑ Naeije R. Hepatopulmonary syndrome and portopulmonary hypertension. Swiss Med Wkly. 2003;133:163-9. PMID 12715285.
- ↑ Template:GPnotebook
- ↑ Uppal S, Diggle CP, Carr IM; et al. (2008). "Mutations in 15-hydroxyprostaglandin dehydrogenase cause primary hypertrophic osteoarthropathy". Nat. Genet. 40 (6): 789–93. doi:10.1038/ng.153. PMID 18500342. Unknown parameter
|month=ignored (help)
Template:Skin and subcutaneous tissue symptoms and signs Template:Nervous and musculoskeletal system symptoms and signs Template:Urinary system symptoms and signs Template:Cognition, perception, emotional state and behaviour symptoms and signs Template:Speech and voice symptoms and signs Template:General symptoms and signs
de:Trommelschlägelfinger it:Dita_ippocratiche no:Trommestikkfingre