*Adults and Adolescents (13 to 16 Years): The recommended oral dose is 1,500 mg (10 mL) once daily administered with a meal.
=====Treatment of Mild-to-Moderate PCP=====
*Adults and Adolescents (13 to 16 Years): The recommended oral dose is 750 mg (5 mL) administered with meals twice daily for 21 days (total daily dose 1,500 mg).
<!--Off-Label Use and Dosage (Adult)-->
<!--Guideline-Supported Use (Adult)-->
|offLabelAdultGuideSupport=There is limited information regarding <i>Off-Label Guideline-Supported Use</i> of {{PAGENAME}} in adult patients.
<!--Non–Guideline-Supported Use (Adult)-->
|offLabelAdultNoGuideSupport======Babesiosis=====
*Atovaquone 750 milligrams (mg) every 12 hours, with azithromycin 500 mg initially then 250 mg daily, each orally for 7 days. <ref name="pmid11078770">{{cite journal| author=Krause PJ, Lepore T, Sikand VK, Gadbaw J, Burke G, Telford SR et al.| title=Atovaquone and azithromycin for the treatment of babesiosis. | journal=N Engl J Med | year= 2000 | volume= 343 | issue= 20 | pages= 1454-8 | pmid=11078770 | doi=10.1056/NEJM200011163432004 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11078770 }} </ref>
<!--Pediatric Indications and Dosage-->
<!--FDA-Labeled Indications and Dosage (Pediatric)-->
|fdaLIADPed=There is limited information regarding <i>FDA-Labeled Use</i> of {{PAGENAME}} in pediatric patients.
<!--Off-Label Use and Dosage (Pediatric)-->
<!--Guideline-Supported Use (Pediatric)-->
|offLabelPedGuideSupport=There is limited information regarding <i>Off-Label Guideline-Supported Use</i> of {{PAGENAME}} in pediatric patients.
<!--Non–Guideline-Supported Use (Pediatric)-->
|offLabelPedNoGuideSupport=There is limited information regarding <i>Off-Label Non–Guideline-Supported Use</i> of {{PAGENAME}} in pediatric patients.
<!--Contraindications-->
|contraindications=*Atovaquone Suspension is contraindicated for patients who develop or have a history of potentially life-threatening allergic reactions to any of the components of the formulation.
<!--Warnings-->
|warnings=* Clinical experience with atovaquone for the treatment of PCP has been limited to patients with mild-to-moderate PCP ([(A-a)DO2]1≤45 mm Hg). Treatment of more severe episodes of PCP has not been systematically studied with this agent. Also, the efficacy of atovaquone in patients who are failing therapy with TMP-SMX has not been systematically studied.
====Precautions====
*Absorption of orally administered atovaquone is limited but can be significantly increased when the drug is taken with food. Plasma atovaquone concentrations have been shown to correlate with the likelihood of successful treatment and survival. Therefore, parenteral therapy with other agents should be considered for patients who have difficulty taking atovaquone with food. Gastrointestinal disorders may limit absorption of orally administered drugs. Patients with these disorders also may not achieve plasma concentrations of atovaquone associated with response to therapy in controlled trials.
*Based upon the spectrum of in vitro antimicrobial activity, atovaquone is not effective therapy for concurrent pulmonary conditions such as [[bacterial]], [[viral]], or other fungal [[pneumonia]] or mycobacterial diseases. Clinical deterioration in patients may be due to infections with other pathogens, as well as progressive PCP. All patients with acute PCP should be carefully evaluated for other possible causes of pulmonary disease and treated with additional agents as appropriate.
*Rare cases of hepatitis, elevated liver function tests and one case of fatal liver failure have been reported in patients treated with atovaquone. A causal relationship between atovaquone use and these events could not be established because of numerous confounding medical conditions and concomitant drug therapies.
*If it is necessary to treat patients with severe hepatic impairment, caution is advised and administration should be closely monitored.
<!--Adverse Reactions-->
<!--Clinical Trials Experience-->
|clinicalTrials=*Because many patients who participated in clinical trials with atovaquone had complications of advanced HIV disease, it was often difficult to distinguish adverse events caused by atovaquone from those caused by underlying medical conditions. There were no life-threatening or fatal adverse experiences caused by atovaquone.
*PCP Prevention Studies: In the dapsone comparative study of Atovaquone Suspension, adverse experience data were collected only for treatment-limiting events. Among the entire population (n = 1,057), treatment-limiting events occurred at similar frequencies in patients treated with Atovaquone Suspension or dapsone (Table 6). Among patients who were taking neither dapsone nor atovaquone at enrollment (n = 487), treatment-limiting events occurred in 43% of patients treated with dapsone and 20% of patients treated with Atovaquone Suspension (P <0.001). In both populations, the type of treatment-limiting events differed between the 2 treatment arms. [[Hypersensitivity]] reactions ([[rash]], [[fever]], allergic reaction) and [[anemia]] were more common in patients treated with dapsone, while gastrointestinal events ([[nausea]], [[diarrhea]] and [[vomiting]]) were more common in patients treated with Atovaquone Suspension.
: [[File:{{PAGENAME}}06.png|thumb|none|800px|This image is provided by the National Library of Medicine.]]
*Table 7 summarizes the clinical adverse experiences reported by ≥20% of patients in any group in the aerosolized pentamidine comparative study of Atovaquone Suspension (n = 549), regardless of attribution. The incidence of adverse experiences at the recommended dose was similar to that seen with aerosolized pentamidine. Rash was the only individual adverse experience that occurred significantly more commonly in patients treated with both dosages of Atovaquone Suspension (39% to 46%) than in patients treated with aerosolized pentamidine (28%). Among patients treated with Atovaquone Suspension, there was no evidence of a dose-related increase in the incidence of adverse experiences. Treatment-limiting adverse experiences occurred less often in patients treated with aerosolized pentamidine (7%) than in patients treated with 1,500 mg Atovaquone Suspension once daily (25%, P ≤0.001) or 750 mg Atovaquone Suspension once daily (16%, P = 0.004). The most common adverse experiences requiring discontinuation of dosing in the group receiving 1,500 mg Atovaquone Suspension once daily were rash (6%), [[diarrhea]] (4%) and [[nausea]] (3%). The most common adverse experience requiring discontinuation of dosing in the group receiving aerosolized pentamidine was [[bronchospasm]] (2%).
: [[File:{{PAGENAME}}07.png|thumb|none|800px|This image is provided by the National Library of Medicine.]]
*Other events occurring in ≥10% of the patients receiving the recommended dose of atovaquone included sweating, flu syndrome, pain, [[sinusitis]], [[pruritus]], [[insomnia]], depression and [[myalgia]]. [[Bronchospasm]] occurred more frequently in patients receiving aerosolized pentamidine (11%) than in patients receiving atovaquone 1,500 mg/day (4%) and atovaquone 750 mg/day (2%).
*Neither atovaquone nor aerosolized pentamidine was associated with a substantial change from baseline values in any measured laboratory parameter, nor were there any significant differences in any measured laboratory parameter between atovaquone and aerosolized pentamidine. Some patients had laboratory abnormalities considered serious by the investigator or that contributed to discontinuation of therapy.
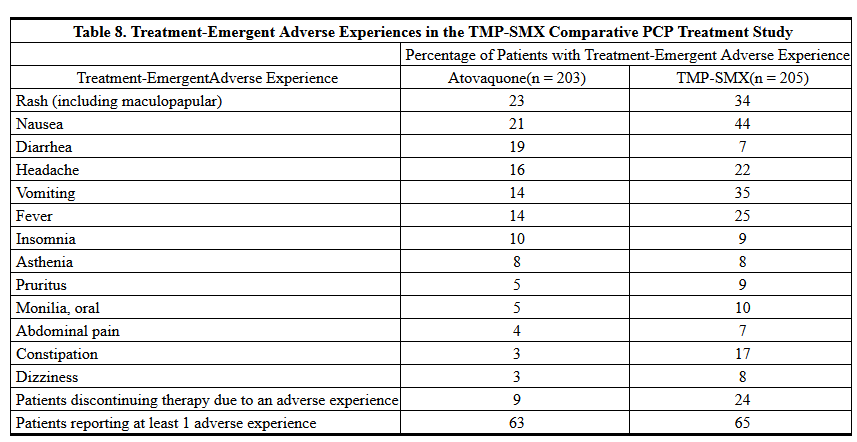
*PCP Treatment Studies: Table 8 summarizes all the clinical adverse experiences reported by ≥5% of the study population during the TMP-SMX comparative study of atovaquone (n = 408), regardless of attribution. The incidence of adverse experiences with Atovaquone Suspension at the recommended dose was similar to that seen with the tablet formulation of atovaquone.
: [[File:{{PAGENAME}}08.png|thumb|none|800px|This image is provided by the National Library of Medicine.]]
*Although an equal percentage of patients receiving atovaquone and TMP-SMX reported at least 1 adverse experience, more patients receiving TMP-SMX required discontinuation of therapy due to an adverse event. Twenty-four percent of patients receiving TMP-SMX were prematurely discontinued from therapy due to an adverse experience versus 9% of patients receiving atovaquone. Four percent of patients receiving atovaquone had therapy discontinued due to development of rash. The majority of cases of rash among patients receiving atovaquone were mild and did not require the discontinuation of dosing. The only other clinical adverse experience that led to premature discontinuation of dosing of atovaquone by more than 1 patient was [[vomiting]] (<1%). The most common adverse experience requiring discontinuation of dosing in the TMP-SMX group was [[rash]] (8%).
*Laboratory test abnormalities reported for ≥5% of the study population during the treatment period are summarized in Table 9. Two percent of patients treated with atovaquone and 7% of patients treated with TMP-SMX had therapy prematurely discontinued due to elevations in ALT/AST. In general, patients treated with atovaquone developed fewer abnormalities in measures of hepatocellular function (ALT, AST, alkaline phosphatase) or amylase values than patients treated with TMP-SMX.
: [[File:{{PAGENAME}}09.png|thumb|none|800px|This image is provided by the National Library of Medicine.]]
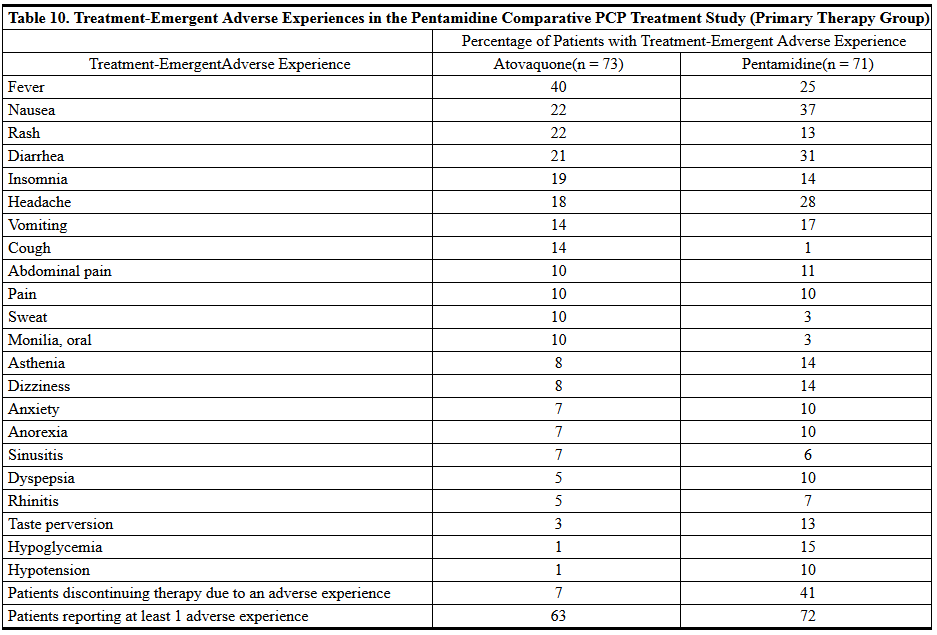
*Table 10 summarizes the clinical adverse experiences reported by ≥5% of the primary therapy study population (n = 144) during the comparative trial of atovaquone and intravenous pentamidine, regardless of attribution. A slightly lower percentage of patients who received atovaquone reported occurrence of adverse events than did those who received [[pentamidine]] (63% vs 72%). However, only 7% of patients discontinued treatment with atovaquone due to adverse events, while 41% of patients who received pentamidine discontinued treatment for this reason (P <;<0.001). Of the 5 patients who discontinued therapy with atovaquone, 3 reported [[rash]] (4%). Rash was not severe in any patient. No other reason for discontinuation of atovaquone was cited more than once. The most frequently cited reasons for discontinuation of pentamidine therapy were [[hypoglycemia]] (11%) and [[vomiting]] (9%).
: [[File:{{PAGENAME}}10.png|thumb|none|800px|This image is provided by the National Library of Medicine.]]
*Laboratory test abnormalities reported in ≥5% of patients in the pentamidine comparative study are presented in Table 11. Laboratory abnormality was reported as the reason for discontinuation of treatment in 2 of 73 patients who received atovaquone. One patient (1%) had elevated [[creatinine]] and BUN levels and 1 patient (1%) had elevated [[amylase]] levels. Laboratory abnormalities were the sole or contributing factor in 14 patients who prematurely discontinued pentamidine therapy. In the 71 patients who received pentamidine, laboratory parameters most frequently reported as reasons for discontinuation were [[hypoglycemia]] (11%), elevated creatinine levels (6%) and [[leukopenia]] (4%).
: [[File:{{PAGENAME}}11.png|thumb|none|800px|This image is provided by the National Library of Medicine.]]
<!--Postmarketing Experience-->
|postmarketing=*In addition to adverse events reported from clinical trials, the following events have been identified during post-approval use of atovaquone. Because they are reported voluntarily from a population of unknown size, estimates of frequency cannot be made. These events have been chosen for inclusion due to a combination of their seriousness, frequency of reporting, or potential causal connection to atovaquone.
=====Blood and Lymphatic System Disorders=====
[[Methemoglobinemia]], [[thrombocytopenia]].
=====Immune System Disorders=====
[[Hypersensitivity]] reactions including [[angioedema]], [[bronchospasm]], throat tightness and [[urticaria]].
=====Eye Disorders=====
Vortex [[keratopathy]].
=====Gastrointestinal Disorders=====
[[Pancreatitis]].
=====Hepatobiliary Disorders=====
Rare cases of [[hepatitis]], and one case of fatal [[liver failure]] have been reported with atovaquone usage.
=====Skin and Subcutaneous Tissue Disorders=====
[[Erythema multiforme]], [[Stevens-Johnson syndrome]] and skin desquamation have been reported in patients receiving multiple drug therapy including atovaquone.
=====Renal and Urinary Disorders=====
Acute [[renal impairment]].
<!--Drug Interactions-->
|drugInteractions=*Atovaquone is highly bound to plasma protein (>99.9%). Therefore, caution should be used when administering atovaquone concurrently with other highly plasma protein-bound drugs with narrow therapeutic indices, as competition for binding sites may occur. The extent of plasma protein binding of atovaquone in human plasma is not affected by the presence of therapeutic concentrations of phenytoin (15 mcg/mL), nor is the binding of phenytoin affected by the presence of atovaquone.
*Rifampin: Coadministration of [[rifampin]] and Atovaquone Suspension results in a significant decrease in average steady-state plasma atovaquone concentrations (see CLINICAL PHARMACOLOGY: Drug Interactions). Alternatives to rifampin should be considered during the course of PCP treatment with atovaquone.
*[[Rifabutin]], another rifamycin, is structurally similar to rifampin and may possibly have some of the same drug interactions as rifampin. No interaction trials have been conducted with atovaquone and rifabutin.
<!--Use in Specific Populations-->
|useInPregnancyFDA=* '''Pregnancy Category C'''
*Atovaquone was not teratogenic and did not cause reproductive toxicity in rats at plasma concentrations up to 2 to 3 times the estimated human exposure. Atovaquone caused maternal toxicity in rabbits at plasma concentrations that were approximately one half the estimated human exposure. Mean fetal body lengths and weights were decreased and there were higher numbers of early resorption and post-implantation loss per dam. It is not clear whether these effects were caused by atovaquone directly or were secondary to maternal toxicity. Concentrations of atovaquone in rabbit fetuses averaged 30% of the concurrent maternal plasma concentrations. In a separate study in rats given a single 14C-radiolabelled dose, concentrations of radiocarbon in rat fetuses were 18% (middle gestation) and 60% (late gestation) of concurrent maternal plasma concentrations. There are no adequate and well-controlled studies in pregnant women. Atovaquone should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
|useInPregnancyAUS=* '''Australian Drug Evaluation Committee (ADEC) Pregnancy Category'''
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of {{PAGENAME}} in women who are pregnant.
|useInLaborDelivery=There is no FDA guidance on use of {{PAGENAME}} during labor and delivery.
|useInNursing=*It is not known whether atovaquone is excreted into human milk. Because many drugs are excreted into human milk, caution should be exercised when atovaquone is administered to a nursing woman. In a rat study, atovaquone concentrations in the milk were 30% of the concurrent atovaquone concentrations in the maternal plasma.
|useInPed=*Evidence of safety and effectiveness in pediatric patients has not been established. A relationship between plasma atovaquone concentrations and successful treatment of PCP has been established in adults (see Table 2). In a study of Atovaquone Suspension in 27 HIV-infected, asymptomatic infants and children between 1 month and 13 years of age, the pharmacokinetics of atovaquone were age-dependent. No drug-related treatment-limiting adverse events were observed in the pharmacokinetic study.
|useInGeri=*Clinical studies of atovaquone did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, reflecting the greater frequency of decreased hepatic, renal, or cardiac function and of concomitant disease or other drug therapy.
|useInGender=There is no FDA guidance on the use of {{PAGENAME}} with respect to specific gender populations.
|useInRace=There is no FDA guidance on the use of {{PAGENAME}} with respect to specific racial populations.
|useInRenalImpair=There is no FDA guidance on the use of {{PAGENAME}} in patients with renal impairment.
|useInHepaticImpair=There is no FDA guidance on the use of {{PAGENAME}} in patients with hepatic impairment.
|useInReproPotential=There is no FDA guidance on the use of {{PAGENAME}} in women of reproductive potentials and males.
|useInImmunocomp=There is no FDA guidance one the use of {{PAGENAME}} in patients who are immunocompromised.
<!--Administration and Monitoring-->
|administration=* Oral
|monitoring=There is limited information regarding <i>Monitoring</i> of {{PAGENAME}} in the drug label.
<!--IV Compatibility-->
|IVCompat=There is limited information regarding <i>IV Compatibility</i> of {{PAGENAME}} in the drug label.
<!--Overdosage-->
|overdose====Chronic Overdose===
There is limited information regarding <i>Chronic Overdose</i> of {{PAGENAME}} in the drug label.
|mechAction=* Atovaquone is a hydroxy-1,4-naphthoquinone, an analog of ubiquinone, with antipneumocystis activity. The mechanism of action against Pneumocystis jiroveci has not been fully elucidated. In Plasmodium species, the site of action appears to be the cytochrome bc1 complex (Complex III). Several metabolic enzymes are linked to the mitochondrial electron transport chain via ubiquinone. Inhibition of electron transport by atovaquone will result in indirect inhibition of these enzymes. The ultimate metabolic effects of such blockade may include inhibition of nucleic acid and ATP synthesis.
{{Editor Help}}
<!--Structure-->
|structure=* Atovaquone is an antiprotozoal agent. The chemical name of atovaquone is trans-2-[4-(4-chlorophenyl)cyclohexyl]-3-hydroxy-1,4-naphthalenedione. Atovaquone is a yellow crystalline solid that is practically insoluble in water. It has a molecular weight of 366.84 and the molecular formula C22H19ClO3. The compound has the following structural formula:
: [[File:{{PAGENAME}}15.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
*Atovaquone Suspension is a formulation of micro-fine particles of atovaquone.
*The atovaquone particles, reduced in size to facilitate absorption, are significantly smaller than those in the previously marketed tablet formulation. Atovaquone Suspension is for oral administration and is bright yellow with a citrus flavor. Each teaspoonful (5 mL) contains 750 mg of atovaquone and the inactive ingredients benzyl alcohol, flavor (ethanol, propylene glycol, triacetin), poloxamer 188, purified water, saccharin sodium and xanthan gum.
<!--Pharmacodynamics-->
|PD=There is limited information regarding <i>Pharmacodynamics</i> of {{PAGENAME}} in the drug label.
<!--Pharmacokinetics-->
|PK=*Absorption
:*Atovaquone is a highly lipophilic compound with low aqueous solubility. The bioavailability of atovaquone is highly dependent on formulation and diet. The suspension formulation provides an approximately 2-fold increase in atovaquone bioavailability in the fasting or fed state compared to the previously marketed tablet formulation. The absolute bioavailability of a 750-mg dose of Atovaquone Suspension administered under fed conditions in 9 HIV-infected (CD4 >100 cells/mm3) volunteers was 47% ± 15%. In the same study, the bioavailability of a 750-mg dose of the previously marketed tablet formulation was 23% ± 11%.
:*Administering atovaquone with food enhances its absorption by approximately 2 fold. In one study, 16 healthy volunteers received a single dose of 750 mg Atovaquone Suspension after an overnight fast and following a standard breakfast (23 g fat: 610 kCal). The mean (±SD) area under the concentration-time curve (AUC) values were 324 ± 115 and 801 ± 320 hr●mcg/mL under fasting and fed conditions, respectively, representing a 2.6 ± 1-fold increase. The effect of food (23 g fat: 400 kCal) on plasma atovaquone concentrations was also evaluated in a multiple-dose, randomized, crossover study in 19 HIV-infected volunteers (CD4 <200 cells/mm3) receiving daily doses of 500 mg Atovaquone Suspension. AUC was 280 ± 114 hr●mcg/mL when atovaquone was administered with food as compared to 169 ± 77 hr●mcg/mL under fasting conditions. Maximum plasma atovaquone concentration (Cmax) was 15.1 ± 6.1 and 8.8 ± 3.7 mcg/mL when atovaquone was administered with food and under fasting conditions, respectively.
*Dose Proportionality
:*Plasma atovaquone concentrations do not increase proportionally with dose. When Atovaquone Suspension was administered with food at dosage regimens of 500 mg once daily, 750 mg once daily and 1,000 mg once daily, average steady-state plasma atovaquone concentrations were 11.7 ± 4.8, 12.5 ± 5.8 and 13.5 ± 5.1 mcg/mL, respectively. The corresponding Cmax concentrations were 15.1 ± 6.1, 15.3 ± 7.6 and 16.8 ± 6.4 mcg/mL. When Atovaquone Suspension was administered to 5 HIV-infected volunteers at a dose of 750 mg twice daily, the average steady-state plasma atovaquone concentration was 21 ± 4.9 mcg/mL and Cmax was 24 ± 5.7 mcg/mL. The minimum plasma atovaquone concentration (Cmin) associated with the 750-mg twice-daily regimen was 16.7 ± 4.6 mcg/mL.
*Distribution
:*Following the intravenous administration of atovaquone, the volume of distribution at steady-state (Vdss) was 0.60 ± 0.17 L/kg (n = 9). Atovaquone is extensively bound to plasma proteins (99.9%) over the concentration range of 1 to 90 mcg/mL. In 3 HIV-infected children who received 750 mg atovaquone as the tablet formulation 4 times daily for 2 weeks, the cerebrospinal fluid concentrations of atovaquone were 0.04, 0.14 and 0.26 mcg/mL, representing less than 1% of the plasma concentration.
*Elimination
:* The plasma clearance of atovaquone following intravenous (IV) administration in 9 HIV-infected volunteers was 10.4 ± 5.5 mL/min (0.15 ± 0.09 mL/min/kg). The half-life of atovaquone was 62.5 ± 35.3 hours after IV administration and ranged from 67 ± 33.4 to 77.6 ± 23.1 hours across studies following administration of Atovaquone Suspension. The half-life of atovaquone is long due to presumed enterohepatic cycling and eventual fecal elimination. In a study where 14C-labelled atovaquone was administered to healthy volunteers, greater than 94% of the dose was recovered as unchanged atovaquone in the feces over 21 days. There was little or no excretion of atovaquone in the urine (less than 0.6%). There is indirect evidence that atovaquone may undergo limited metabolism; however, a specific metabolite has not been identified.
*Special Populations
*Pediatrics
:*In a study of Atovaquone Suspension in 27 [[HIV]]-infected, asymptomatic infants and children between 1 month and 13 years of age, the pharmacokinetics of atovaquone were age dependent. These patients were dosed once daily with food for 12 days. The average steady-state plasma atovaquone concentrations in the 24 patients with available concentration data are shown in Table 1.
: [[File:{{PAGENAME}}01.png|thumb|none|800px|This image is provided by the National Library of Medicine.]]
*Hepatic/Renal Impairment
:* The pharmacokinetics of atovaquone have not been studied in patients with hepatic or renal impairment.
[[Image:270px-Malarone tablets.jpg|200px|thumb|left|Malarone anti-malaria tablets, as issued in the UK.]]
*Drug Interactions
'''Atovaquone''' (alternative spelling: '''atavaquone''') is a chemical compound that belongs to the class of [[naphthalene]]s. Atovaquone is a hydroxy-1,4-naphthoquinone, an analog of [[ubiquinone]], with antipneumocystic activity. Its average wholesale price is about $2.13 per standard 250 mg. tablet.<ref>[http://www.aegis.com/pubs/atn/1992/ATN16401.html (ATN) Atovaquone (Mepron; 566C80) Approved for Pneumocystis; Drug Development, Activism Success]</ref> It is also manufactured in the US in the liquid form, or oral suspension, under the brand name Mepron.<ref>[http://www.drugs.com/pro/mepron.html Mepron]</ref>
Atovaquone is a medication used to treat or prevent:
*Rifampin
# [[Pneumocystis pneumonia]] (PCP), although it is not approved for treatment of severe PCP.
:* In a study with 13 HIV-infected volunteers, the oral administration of rifampin 600 mg every 24 hours with Atovaquone Suspension 750 mg every 12 hours resulted in a 52% ± 13% decrease in the average steady-state plasma atovaquone concentration and a 37% ± 42% increase in the average steady-state plasma rifampin concentration. The half-life of atovaquone decreased from 82 ± 36 hours when administered without rifampin to 50 ± 16 hours with rifampin.
# [[Toxoplasmosis]]. The medication has antiparasitic and therapeutic effects.
:*Rifabutin, another rifamycin, is structurally similar to rifampin and may possibly have some of the same drug interactions as rifampin. No interaction trials have been conducted with atovaquone and rifabutin.
# [[Malaria]]. It is one of the two components (along with [[proguanil]]) in the drug Malarone. Malarone has fewer side effects than [[mefloquine]], but can be more expensive because it's taken daily.<ref>[http://healthlink.mcw.edu/article/979237802.html Malarone: New Malaria Medication With Fewer Side-effects]</ref>
[[Co-trimoxazole|Trimethoprim-sulfamethoxazole]] (TMP-SMX, Bactrim) is generally considered first line therapy for PCP or toxoplasmosis. However, atovaquone may be used in patients who cannot tolerate, or are allergic to, TMP-SMX. In addition, atovaquone has the advantage of not causing [[myelosuppression]], which is an important issue in patients who have undergone [[bone marrow transplantation]].
*Trimethoprim/Sulfamethoxazole (TMP-SMX)
:* The possible interaction between atovaquone and TMP-SMX was evaluated in 6 HIV-infected adult volunteers as part of a larger multiple-dose, dose-escalation and chronic dosing study of Atovaquone Suspension. In this crossover study, Atovaquone Suspension 500 mg once daily, or TMP-SMX tablets (160 mg trimethoprim and 800 mg sulfamethoxazole) twice daily, or the combination were administered with food to achieve steady-state. No difference was observed in the average steady-state plasma atovaquone concentration after coadministration with TMP-SMX. Coadministration of atovaquone with TMP-SMX resulted in a 17% and 8% decrease in average steady-state concentrations of trimethoprim and sulfamethoxazole in plasma, respectively. This effect is minor and would not be expected to produce clinically significant events.
==Malaria==
*Zidovudine
Atovaquone is only available as a fixed preparation with [[proguanil]] that has been commercially available from [[GlaxoSmithKline]] since 2000 as '''Malarone'''® (sometimes abbreviated '''A+P'''). It can be used both to treat and to prevent malaria.
:* Data from 14 HIV-infected volunteers who were given atovaquone tablets 750 mg every 12 hours with zidovudine 200 mg every 8 hours showed a 24% ± 12% decrease in zidovudine apparent oral clearance, leading to a 35% ± 23% increase in plasma zidovudine AUC. The glucuronide metabolite:parent ratio decreased from a mean of 4.5 when zidovudine was administered alone to 3.1 when zidovudine was administered with atovaquone tablets. This effect is minor and would not be expected to produce clinically significant events. Zidovudine had no effect on atovaquone pharmacokinetics.
A "standard" tablet of Malarone contains 100 mg of proguanil hydrochloride and 250 mg of atovaquone. A "pediatric" tablet of Malarone contains 25 mg of proguanil hydrochloride and 62.5 mg of atovaquone.
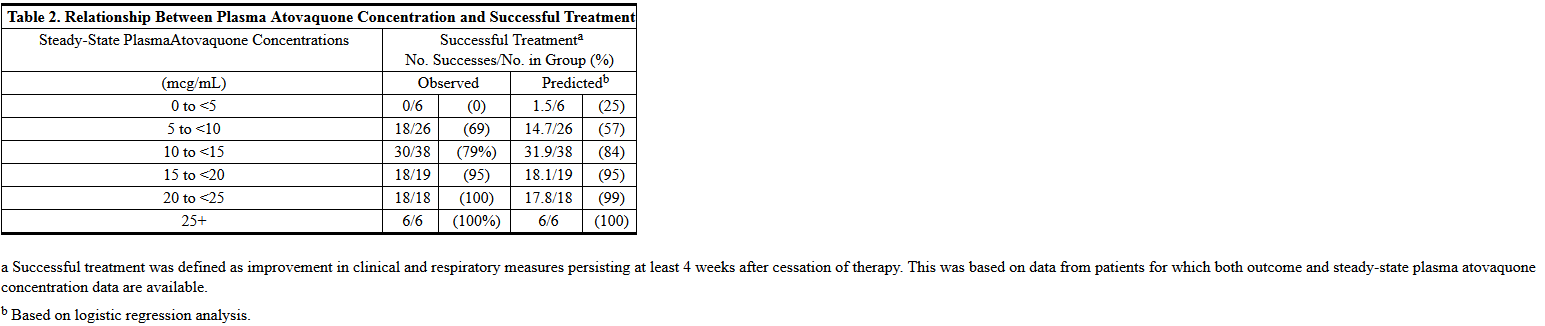
*Relationship Between Plasma Atovaquone Concentration and Clinical Outcome: In a comparative study of atovaquone tablets with TMP-SMX for oral treatment of mild-to-moderate PCP (see INDICATIONS AND USAGE), where AIDS patients received 750 mg atovaquone tablets 3 times daily for 21 days, the mean steady-state atovaquone concentration was 13.9 ± 6.9 mcg/mL (n = 133). Analysis of these data established a relationship between plasma atovaquone concentration and successful treatment. This is shown in Table 2.
===Treatment===
: [[File:{{PAGENAME}}02.png|thumb|none|800px|This image is provided by the National Library of Medicine.]]
The adult treatment dose is four "standard" tablets once a day for three days. In children, the drug is prescribed by body weight:
*11 to 20 kg: 1 "standard" tablet once daily for 3 days;
*21 to 30 kg: 2 "standard" tablets once daily for 3 days;
*31 to 40 kg: 3 "standard" tablets once daily for 3 days;
*41 kg and above: use adult dose.
Malarone is not licensed for use in children weighing 10 kg or less. The "pediatric" tablets are ''not'' used in malaria treatment.
The advice of a specialist should always be sought when starting malaria treatment. Malarone should not be used to treat severe malaria, when an injectable drug ([[quinine]] or [[artesunate]] in the UK; [[quinidine]] in the US) should be used instead.
*A dosing regimen of Atovaquone Suspension for the treatment of mild-to-moderate PCP has been selected to achieve average plasma atovaquone concentrations of approximately 20 mcg/mL, because this plasma concentration was previously shown to be well tolerated and associated with the highest treatment success rates (Table 2). In an open-label PCP treatment study with Atovaquone Suspension, dosing regimens of 1,000 mg once daily, 750 mg twice daily, 1,500 mg once daily and 1,000 mg twice daily were explored. The average steady-state plasma atovaquone concentration achieved at the 750-mg twice-daily dose given with meals was 22 ± 10.1 mcg/mL (n = 18).
===Prevention===
<!--Nonclinical Toxicology-->
Medical advice should always be taken before choosing a drug for malaria prevention. Because some strains of malaria are resistant, Malarone is not effective for malaria prevention in all parts of the world. It must be taken with a fatty meal or at least some milk to be absorbed adequately.
|nonClinToxic=*Carcinogenicity studies in rats were negative; 24-month studies in mice showed treatment-related increases in incidence of hepatocellular adenoma and hepatocellular carcinoma at all doses tested which ranged from 1.4 to 3.6 times the average steady-state plasma concentrations in humans during acute treatment of PCP. Atovaquone was negative with or without metabolic activation in the Ames Salmonella mutagenicity assay, the Mouse Lymphoma mutagenesis assay and the Cultured Human Lymphocyte cytogenetic assay. No evidence of genotoxicity was observed in the in vivo Mouse Micronucleus assay.
The adult dose is one "standard" tablet daily starting one or two days before traveling into a malaria-endemic area, and continuing throughout the stay and then for another 7 days after returning from the malarious area.
<!--Clinical Studies-->
|clinicalStudies======Prevention of PCP=====
The child dose is prescribed according to body weight:
*The indication for prevention of PCP is based on the results of 2 clinical trials comparing Atovaquone Suspension to dapsone or aerosolized pentamidine in HIV-infected adult and adolescent patients at risk of PCP (CD4 count <200 cells/mm3 or a prior episode of PCP) and intolerant to TMP-SMX.
*11–20 kg: 1 "pediatric" tablet once daily;
*21–30 kg: 2 "pediatric" tablets once daily;
*31–40 kg: 3 "pediatric" tablets once daily;
*41 kg and above use adult dose.
The duration of treatment is the same as for adults.
===Resistance===
*Dapsone Comparative Study: This randomized, open-label trial enrolled a total of 1,057 patients at 48 study centers. Patients were randomized to receive 1,500 mg Atovaquone Suspension once daily (n = 536) or 100 mg dapsone once daily (n = 521). Median follow-up was 24 months. Patients randomized to the dapsone arm who were seropositive for Toxoplasma gondii and had a CD4 count <100 cells/mm3 also received pyrimethamine and folinic acid. PCP event rates are shown in Table 3. There was no significant difference in mortality rates between the groups.
Proguanil acts as a [[mitochondrion|mitochondrial]] sensitiser and synergizes with atovaquone; also, there is a high natural frequency of [[Duodenal cytochrome B|cytochrome B]] mutants which leads to a high failure rate if atovaquone is used on its own to treat malaria. Specific mutations (Y268S, Y268C) have been shown to confer resistance ''in vivo,''<ref>{{cite journal | author=Färnet A, Lindberg J, Gil P, ''et al.'' | title=Evidence of ''Plasmodium falciparum'' malaria resistant to atovaquone and proguoanil hydrochloride: case reports | year=2003 | journal=Brit Med J | volume=326 | pages=628–29 }}</ref><ref>{{cite journal | author=Fivelman QL, Butcher GA, Adagu IS, ''et al.'' | title=Malarone treatment failure and in-vitro confirmation of resistance of ''Plasmodium falciparum'' isolate from Lagos, Nigeria | year=2002 | journal=Malaria J | volume=1 | pages=1 }}</ref><ref>{{cite journal | author=Schwartz E, Bujanover S, Kain KC | title=Genetic confirmation of atovaquone-proguanil-resistant ''Plasmodium falciparum'' malaria acquired by a nonimmune traveller to east Africa | year=2003 | journal=Clin Infect Dis | volume=37 | pages=450–51 }}</ref> but there are other mechanisms of resistance that remain unknown.<ref>{{cite journal | author=Wichmann O, Muehlen M, Gruss H, ''et al.'' | title=Malarone treatment failure not associated with previously described mutations in the cytochrome b gene | year=2004 | journal=Malaria J | volume=3 | pages=14 }}</ref>
==References==
*Aerosolized Pentamidine Comparative Study: This randomized, open-label trial enrolled a total of 549 patients at 35 study centers. Patients were randomized to receive 1,500 mg Atovaquone Suspension once daily (n = 175), 750 mg Atovaquone Suspension once daily (n = 188), or 300 mg aerosolized pentamidine once monthly (n = 186). Median follow-up was 11.3 months. The results of the PCP event rates appear in Table 3. There were no significant differences in mortality rates among the groups.
{{reflist|2}}
==External links==
: [[File:{{PAGENAME}}03.png|thumb|none|800px|This image is provided by the National Library of Medicine.]]
* [http://www.dartmouth.edu/~blt/Publications/JBC279,2817.pdf#search='Atovaquone' Molecular Basis for Atovaquone Resistance in Pneumocystis jirovecii]
{{Agents against amoebiasis and other protozoal diseases}}
{{SIB}}
*An analysis of all PCP events (intent-to-treat analysis) showed results similar to those above.
[[Category:Antimalarial agents]]
=====Treatment of PCP=====
[[Category:Naphthalenes]]
[[Category:Organochlorides]]
*The indication for treatment of mild-to-moderate PCP is based on the results of comparative pharmacokinetic studies of the suspension and tablet formulations (see CLINICAL PHARMACOLOGY) and clinical efficacy studies of the tablet formulation which established a relationship between plasma atovaquone concentration and successful treatment. The results of a randomized, double-blind trial comparing atovaquone to TMP-SMX in AIDS patients with mild-to-moderate PCP (defined in the study protocol as an alveolar-arterial oxygen diffusion gradient [(A-a)DO2]1≤45 mm Hg and PaO2≥60 mm Hg on room air) and a randomized trial comparing atovaquone to IV pentamidine isethionate in patients with mild-to-moderate PCP intolerant to trimethoprim or sulfa-antimicrobials are summarized below:
*TMP-SMX Comparative Study: This double-blind, randomized trial initiated in 1990 was designed to compare the safety and efficacy of atovaquone to that of TMP-SMX for the treatment of AIDS patients with histologically confirmed PCP. Only patients with mild-to-moderate PCP were eligible for enrollment.
*A total of 408 patients were enrolled into the trial at 37 study centers. Eighty-six patients without histologic confirmation of PCP were excluded from the efficacy analyses. Of the 322 patients with histologically confirmed PCP, 160 were randomized to receive atovaquone and 162 to TMP-SMX.
*Study participants randomized to treatment with atovaquone were to receive 750 mg atovaquone (three 250-mg tablets) 3 times daily for 21 days and those randomized to TMP-SMX were to receive 320 mg TMP plus 1,600 mg SMX 3 times daily for 21 days.
*Therapy success was defined as improvement in clinical and respiratory measures persisting at least 4 weeks after cessation of therapy. Therapy failures included lack of response, treatment discontinuation due to an adverse experience and unevaluable.
*There was a significant difference (P = 0.03) in mortality rates between the treatment groups. Among the 322 patients with confirmed PCP, 13 of 160 (8%) patients treated with atovaquone and 4 of 162 (2.5%) patients receiving TMP-SMX died during the 21-day treatment course or 8-week follow-up period. In the intent-to-treat analysis for all 408 randomized patients, there were 16 (8%) deaths in the arm treated with atovaquone and 7 (3.4%) deaths in the TMP-SMX arm (P = 0.051). Of the 13 patients treated with atovaquone who died, 4 died of PCP and 5 died with a combination of bacterial infections and PCP; bacterial infections did not appear to be a factor in any of the 4 deaths among TMP-SMX-treated patients.
*A correlation between plasma atovaquone concentrations and death was demonstrated; in general, patients with lower plasma concentrations were more likely to die. For those patients for whom day 4 plasma atovaquone concentration data are available, 5 (63%) of the 8 patients with concentrations <5 mcg/mL died during participation in the study. However, only 1 (2%) of the 49 patients with day 4 plasma atovaquone concentrations ≥5 mcg/mL died.
*Sixty-two percent of patients on atovaquone and 64% of patients on TMP-SMX were classified as protocol-defined therapy successes (Table 4).
: [[File:{{PAGENAME}}04.png|thumb|none|800px|This image is provided by the National Library of Medicine.]]
*The failure rate due to lack of response was significantly larger for patients receiving atovaquone while the failure rate due to adverse experiences was significantly larger for patients receiving TMP-SMX.
*There were no significant differences in the effect of either treatment on additional indicators of response (i.e., arterial blood gas measurements, vital signs, serum LDH levels, clinical symptoms and chest radiographs).
=====Pentamidine Comparative Study=====
*This unblinded, randomized trial initiated in 1991 was designed to compare the safety and efficacy of atovaquone to that of pentamidine for the treatment of histologically confirmed mild or moderate PCP in AIDS patients. Approximately 80% of the patients either had a history of intolerance to trimethoprim or sulfa-antimicrobials (the primary therapy group) or were experiencing intolerance to TMP-SMX with treatment of an episode of PCP at the time of enrollment in the study (the salvage treatment group).
*Patients randomized to atovaquone were to receive 750 mg atovaquone (three 250-mg tablets) 3 times daily for 21 days and those randomized to pentamidine isethionate were to receive a 3- to 4-mg/kg single IV infusion daily for 21 days.
*A total of 174 patients were enrolled into the trial at 22 study centers. Thirty-nine patients without histologic confirmation of PCP were excluded from the efficacy analyses. Of the 135 patients with histologically confirmed PCP, 70 were randomized to receive atovaquone and 65 to pentamidine. One hundred and ten (110) of these were in the primary therapy group and 25 were in the salvage therapy group. One patient in the primary therapy group randomized to receive pentamidine did not receive study medication.
*There was no difference in mortality rates between the treatment groups. Among the 135 patients with confirmed PCP, 10 of 70 (14%) patients randomized to atovaquone and 9 of 65 (14%) patients randomized to pentamidine died during the 21-day treatment course or 8-week follow-up period. In the intent-to-treat analysis for all randomized patients, there were 11 (12.5%) deaths in the arm treated with atovaquone and 12 (14%) deaths in the pentamidine arm. For those patients for whom day 4 plasma atovaquone concentrations are available, 3 of 5 (60%) patients with concentrations <5 mcg/mL died during participation in the study. However, only 2 of 21 (9%) patients with day 4 plasma concentrations ≥5 mcg/mL died.
*The therapeutic outcomes for the 134 patients who received study medication in this trial are presented in Table 5.
: [[File:{{PAGENAME}}05.png|thumb|none|800px|This image is provided by the National Library of Medicine.]]
<!--How Supplied-->
|howSupplied=* Atovaquone Suspension (bright yellow, citrus flavored) containing 750 mg atovaquone in each teaspoonful (5 mL).
*Bottle of 210 mL with child-resistant cap (NDC 65162-693-88).
*Store at 15° to 25°C (59° to 77°F). DO NOT FREEZE. Dispense in tight container as defined in USP.
<!--Patient Counseling Information-->
|fdaPatientInfo=There is limited information regarding <i>Patient Counseling Information</i> of {{PAGENAME}} in the drug label.
<!--Precautions with Alcohol-->
|alcohol=* Alcohol-{{PAGENAME}} interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
<!--Brand Names-->
|brandNames=* ATOVAQUONE®<ref>{{Cite web | title = ATOVAQUONE atovaquone suspension | url = http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=b7398fcf-522a-488a-8dd6-051561f62804 }}</ref>
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Adults and Adolescents (13 to 16 Years): The recommended oral dose is 1,500 mg (10 mL) once daily administered with a meal.
Treatment of Mild-to-Moderate PCP
Adults and Adolescents (13 to 16 Years): The recommended oral dose is 750 mg (5 mL) administered with meals twice daily for 21 days (total daily dose 1,500 mg).
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Atovaquone in adult patients.
Non–Guideline-Supported Use
Babesiosis
Atovaquone 750 milligrams (mg) every 12 hours, with azithromycin 500 mg initially then 250 mg daily, each orally for 7 days. [1]
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Atovaquone in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Atovaquone in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Atovaquone in pediatric patients.
Contraindications
Atovaquone Suspension is contraindicated for patients who develop or have a history of potentially life-threatening allergic reactions to any of the components of the formulation.
Warnings
Clinical experience with atovaquone for the treatment of PCP has been limited to patients with mild-to-moderate PCP ([(A-a)DO2]1≤45 mm Hg). Treatment of more severe episodes of PCP has not been systematically studied with this agent. Also, the efficacy of atovaquone in patients who are failing therapy with TMP-SMX has not been systematically studied.
Precautions
Absorption of orally administered atovaquone is limited but can be significantly increased when the drug is taken with food. Plasma atovaquone concentrations have been shown to correlate with the likelihood of successful treatment and survival. Therefore, parenteral therapy with other agents should be considered for patients who have difficulty taking atovaquone with food. Gastrointestinal disorders may limit absorption of orally administered drugs. Patients with these disorders also may not achieve plasma concentrations of atovaquone associated with response to therapy in controlled trials.
Based upon the spectrum of in vitro antimicrobial activity, atovaquone is not effective therapy for concurrent pulmonary conditions such as bacterial, viral, or other fungal pneumonia or mycobacterial diseases. Clinical deterioration in patients may be due to infections with other pathogens, as well as progressive PCP. All patients with acute PCP should be carefully evaluated for other possible causes of pulmonary disease and treated with additional agents as appropriate.
Rare cases of hepatitis, elevated liver function tests and one case of fatal liver failure have been reported in patients treated with atovaquone. A causal relationship between atovaquone use and these events could not be established because of numerous confounding medical conditions and concomitant drug therapies.
If it is necessary to treat patients with severe hepatic impairment, caution is advised and administration should be closely monitored.
Adverse Reactions
Clinical Trials Experience
Because many patients who participated in clinical trials with atovaquone had complications of advanced HIV disease, it was often difficult to distinguish adverse events caused by atovaquone from those caused by underlying medical conditions. There were no life-threatening or fatal adverse experiences caused by atovaquone.
PCP Prevention Studies: In the dapsone comparative study of Atovaquone Suspension, adverse experience data were collected only for treatment-limiting events. Among the entire population (n = 1,057), treatment-limiting events occurred at similar frequencies in patients treated with Atovaquone Suspension or dapsone (Table 6). Among patients who were taking neither dapsone nor atovaquone at enrollment (n = 487), treatment-limiting events occurred in 43% of patients treated with dapsone and 20% of patients treated with Atovaquone Suspension (P <0.001). In both populations, the type of treatment-limiting events differed between the 2 treatment arms. Hypersensitivity reactions (rash, fever, allergic reaction) and anemia were more common in patients treated with dapsone, while gastrointestinal events (nausea, diarrhea and vomiting) were more common in patients treated with Atovaquone Suspension.
This image is provided by the National Library of Medicine.
Table 7 summarizes the clinical adverse experiences reported by ≥20% of patients in any group in the aerosolized pentamidine comparative study of Atovaquone Suspension (n = 549), regardless of attribution. The incidence of adverse experiences at the recommended dose was similar to that seen with aerosolized pentamidine. Rash was the only individual adverse experience that occurred significantly more commonly in patients treated with both dosages of Atovaquone Suspension (39% to 46%) than in patients treated with aerosolized pentamidine (28%). Among patients treated with Atovaquone Suspension, there was no evidence of a dose-related increase in the incidence of adverse experiences. Treatment-limiting adverse experiences occurred less often in patients treated with aerosolized pentamidine (7%) than in patients treated with 1,500 mg Atovaquone Suspension once daily (25%, P ≤0.001) or 750 mg Atovaquone Suspension once daily (16%, P = 0.004). The most common adverse experiences requiring discontinuation of dosing in the group receiving 1,500 mg Atovaquone Suspension once daily were rash (6%), diarrhea (4%) and nausea (3%). The most common adverse experience requiring discontinuation of dosing in the group receiving aerosolized pentamidine was bronchospasm (2%).
This image is provided by the National Library of Medicine.
Other events occurring in ≥10% of the patients receiving the recommended dose of atovaquone included sweating, flu syndrome, pain, sinusitis, pruritus, insomnia, depression and myalgia. Bronchospasm occurred more frequently in patients receiving aerosolized pentamidine (11%) than in patients receiving atovaquone 1,500 mg/day (4%) and atovaquone 750 mg/day (2%).
Neither atovaquone nor aerosolized pentamidine was associated with a substantial change from baseline values in any measured laboratory parameter, nor were there any significant differences in any measured laboratory parameter between atovaquone and aerosolized pentamidine. Some patients had laboratory abnormalities considered serious by the investigator or that contributed to discontinuation of therapy.
PCP Treatment Studies: Table 8 summarizes all the clinical adverse experiences reported by ≥5% of the study population during the TMP-SMX comparative study of atovaquone (n = 408), regardless of attribution. The incidence of adverse experiences with Atovaquone Suspension at the recommended dose was similar to that seen with the tablet formulation of atovaquone.
This image is provided by the National Library of Medicine.
Although an equal percentage of patients receiving atovaquone and TMP-SMX reported at least 1 adverse experience, more patients receiving TMP-SMX required discontinuation of therapy due to an adverse event. Twenty-four percent of patients receiving TMP-SMX were prematurely discontinued from therapy due to an adverse experience versus 9% of patients receiving atovaquone. Four percent of patients receiving atovaquone had therapy discontinued due to development of rash. The majority of cases of rash among patients receiving atovaquone were mild and did not require the discontinuation of dosing. The only other clinical adverse experience that led to premature discontinuation of dosing of atovaquone by more than 1 patient was vomiting (<1%). The most common adverse experience requiring discontinuation of dosing in the TMP-SMX group was rash (8%).
Laboratory test abnormalities reported for ≥5% of the study population during the treatment period are summarized in Table 9. Two percent of patients treated with atovaquone and 7% of patients treated with TMP-SMX had therapy prematurely discontinued due to elevations in ALT/AST. In general, patients treated with atovaquone developed fewer abnormalities in measures of hepatocellular function (ALT, AST, alkaline phosphatase) or amylase values than patients treated with TMP-SMX.
Table 10 summarizes the clinical adverse experiences reported by ≥5% of the primary therapy study population (n = 144) during the comparative trial of atovaquone and intravenous pentamidine, regardless of attribution. A slightly lower percentage of patients who received atovaquone reported occurrence of adverse events than did those who received pentamidine (63% vs 72%). However, only 7% of patients discontinued treatment with atovaquone due to adverse events, while 41% of patients who received pentamidine discontinued treatment for this reason (P <;<0.001). Of the 5 patients who discontinued therapy with atovaquone, 3 reported rash (4%). Rash was not severe in any patient. No other reason for discontinuation of atovaquone was cited more than once. The most frequently cited reasons for discontinuation of pentamidine therapy were hypoglycemia (11%) and vomiting (9%).
This image is provided by the National Library of Medicine.
Laboratory test abnormalities reported in ≥5% of patients in the pentamidine comparative study are presented in Table 11. Laboratory abnormality was reported as the reason for discontinuation of treatment in 2 of 73 patients who received atovaquone. One patient (1%) had elevated creatinine and BUN levels and 1 patient (1%) had elevated amylase levels. Laboratory abnormalities were the sole or contributing factor in 14 patients who prematurely discontinued pentamidine therapy. In the 71 patients who received pentamidine, laboratory parameters most frequently reported as reasons for discontinuation were hypoglycemia (11%), elevated creatinine levels (6%) and leukopenia (4%).
This image is provided by the National Library of Medicine.
Postmarketing Experience
In addition to adverse events reported from clinical trials, the following events have been identified during post-approval use of atovaquone. Because they are reported voluntarily from a population of unknown size, estimates of frequency cannot be made. These events have been chosen for inclusion due to a combination of their seriousness, frequency of reporting, or potential causal connection to atovaquone.
Atovaquone is highly bound to plasma protein (>99.9%). Therefore, caution should be used when administering atovaquone concurrently with other highly plasma protein-bound drugs with narrow therapeutic indices, as competition for binding sites may occur. The extent of plasma protein binding of atovaquone in human plasma is not affected by the presence of therapeutic concentrations of phenytoin (15 mcg/mL), nor is the binding of phenytoin affected by the presence of atovaquone.
Rifampin: Coadministration of rifampin and Atovaquone Suspension results in a significant decrease in average steady-state plasma atovaquone concentrations (see CLINICAL PHARMACOLOGY: Drug Interactions). Alternatives to rifampin should be considered during the course of PCP treatment with atovaquone.
Rifabutin, another rifamycin, is structurally similar to rifampin and may possibly have some of the same drug interactions as rifampin. No interaction trials have been conducted with atovaquone and rifabutin.
Atovaquone was not teratogenic and did not cause reproductive toxicity in rats at plasma concentrations up to 2 to 3 times the estimated human exposure. Atovaquone caused maternal toxicity in rabbits at plasma concentrations that were approximately one half the estimated human exposure. Mean fetal body lengths and weights were decreased and there were higher numbers of early resorption and post-implantation loss per dam. It is not clear whether these effects were caused by atovaquone directly or were secondary to maternal toxicity. Concentrations of atovaquone in rabbit fetuses averaged 30% of the concurrent maternal plasma concentrations. In a separate study in rats given a single 14C-radiolabelled dose, concentrations of radiocarbon in rat fetuses were 18% (middle gestation) and 60% (late gestation) of concurrent maternal plasma concentrations. There are no adequate and well-controlled studies in pregnant women. Atovaquone should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Atovaquone in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Atovaquone during labor and delivery.
Nursing Mothers
It is not known whether atovaquone is excreted into human milk. Because many drugs are excreted into human milk, caution should be exercised when atovaquone is administered to a nursing woman. In a rat study, atovaquone concentrations in the milk were 30% of the concurrent atovaquone concentrations in the maternal plasma.
Pediatric Use
Evidence of safety and effectiveness in pediatric patients has not been established. A relationship between plasma atovaquone concentrations and successful treatment of PCP has been established in adults (see Table 2). In a study of Atovaquone Suspension in 27 HIV-infected, asymptomatic infants and children between 1 month and 13 years of age, the pharmacokinetics of atovaquone were age-dependent. No drug-related treatment-limiting adverse events were observed in the pharmacokinetic study.
Geriatic Use
Clinical studies of atovaquone did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, reflecting the greater frequency of decreased hepatic, renal, or cardiac function and of concomitant disease or other drug therapy.
Gender
There is no FDA guidance on the use of Atovaquone with respect to specific gender populations.
Race
There is no FDA guidance on the use of Atovaquone with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Atovaquone in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Atovaquone in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Atovaquone in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Atovaquone in patients who are immunocompromised.
Administration and Monitoring
Administration
Oral
Monitoring
There is limited information regarding Monitoring of Atovaquone in the drug label.
IV Compatibility
There is limited information regarding IV Compatibility of Atovaquone in the drug label.
Overdosage
Chronic Overdose
There is limited information regarding Chronic Overdose of Atovaquone in the drug label.
Atovaquone is a hydroxy-1,4-naphthoquinone, an analog of ubiquinone, with antipneumocystis activity. The mechanism of action against Pneumocystis jiroveci has not been fully elucidated. In Plasmodium species, the site of action appears to be the cytochrome bc1 complex (Complex III). Several metabolic enzymes are linked to the mitochondrial electron transport chain via ubiquinone. Inhibition of electron transport by atovaquone will result in indirect inhibition of these enzymes. The ultimate metabolic effects of such blockade may include inhibition of nucleic acid and ATP synthesis.
Structure
Atovaquone is an antiprotozoal agent. The chemical name of atovaquone is trans-2-[4-(4-chlorophenyl)cyclohexyl]-3-hydroxy-1,4-naphthalenedione. Atovaquone is a yellow crystalline solid that is practically insoluble in water. It has a molecular weight of 366.84 and the molecular formula C22H19ClO3. The compound has the following structural formula:
This image is provided by the National Library of Medicine.
Atovaquone Suspension is a formulation of micro-fine particles of atovaquone.
The atovaquone particles, reduced in size to facilitate absorption, are significantly smaller than those in the previously marketed tablet formulation. Atovaquone Suspension is for oral administration and is bright yellow with a citrus flavor. Each teaspoonful (5 mL) contains 750 mg of atovaquone and the inactive ingredients benzyl alcohol, flavor (ethanol, propylene glycol, triacetin), poloxamer 188, purified water, saccharin sodium and xanthan gum.
Pharmacodynamics
There is limited information regarding Pharmacodynamics of Atovaquone in the drug label.
Pharmacokinetics
Absorption
Atovaquone is a highly lipophilic compound with low aqueous solubility. The bioavailability of atovaquone is highly dependent on formulation and diet. The suspension formulation provides an approximately 2-fold increase in atovaquone bioavailability in the fasting or fed state compared to the previously marketed tablet formulation. The absolute bioavailability of a 750-mg dose of Atovaquone Suspension administered under fed conditions in 9 HIV-infected (CD4 >100 cells/mm3) volunteers was 47% ± 15%. In the same study, the bioavailability of a 750-mg dose of the previously marketed tablet formulation was 23% ± 11%.
Administering atovaquone with food enhances its absorption by approximately 2 fold. In one study, 16 healthy volunteers received a single dose of 750 mg Atovaquone Suspension after an overnight fast and following a standard breakfast (23 g fat: 610 kCal). The mean (±SD) area under the concentration-time curve (AUC) values were 324 ± 115 and 801 ± 320 hr●mcg/mL under fasting and fed conditions, respectively, representing a 2.6 ± 1-fold increase. The effect of food (23 g fat: 400 kCal) on plasma atovaquone concentrations was also evaluated in a multiple-dose, randomized, crossover study in 19 HIV-infected volunteers (CD4 <200 cells/mm3) receiving daily doses of 500 mg Atovaquone Suspension. AUC was 280 ± 114 hr●mcg/mL when atovaquone was administered with food as compared to 169 ± 77 hr●mcg/mL under fasting conditions. Maximum plasma atovaquone concentration (Cmax) was 15.1 ± 6.1 and 8.8 ± 3.7 mcg/mL when atovaquone was administered with food and under fasting conditions, respectively.
Dose Proportionality
Plasma atovaquone concentrations do not increase proportionally with dose. When Atovaquone Suspension was administered with food at dosage regimens of 500 mg once daily, 750 mg once daily and 1,000 mg once daily, average steady-state plasma atovaquone concentrations were 11.7 ± 4.8, 12.5 ± 5.8 and 13.5 ± 5.1 mcg/mL, respectively. The corresponding Cmax concentrations were 15.1 ± 6.1, 15.3 ± 7.6 and 16.8 ± 6.4 mcg/mL. When Atovaquone Suspension was administered to 5 HIV-infected volunteers at a dose of 750 mg twice daily, the average steady-state plasma atovaquone concentration was 21 ± 4.9 mcg/mL and Cmax was 24 ± 5.7 mcg/mL. The minimum plasma atovaquone concentration (Cmin) associated with the 750-mg twice-daily regimen was 16.7 ± 4.6 mcg/mL.
Distribution
Following the intravenous administration of atovaquone, the volume of distribution at steady-state (Vdss) was 0.60 ± 0.17 L/kg (n = 9). Atovaquone is extensively bound to plasma proteins (99.9%) over the concentration range of 1 to 90 mcg/mL. In 3 HIV-infected children who received 750 mg atovaquone as the tablet formulation 4 times daily for 2 weeks, the cerebrospinal fluid concentrations of atovaquone were 0.04, 0.14 and 0.26 mcg/mL, representing less than 1% of the plasma concentration.
Elimination
The plasma clearance of atovaquone following intravenous (IV) administration in 9 HIV-infected volunteers was 10.4 ± 5.5 mL/min (0.15 ± 0.09 mL/min/kg). The half-life of atovaquone was 62.5 ± 35.3 hours after IV administration and ranged from 67 ± 33.4 to 77.6 ± 23.1 hours across studies following administration of Atovaquone Suspension. The half-life of atovaquone is long due to presumed enterohepatic cycling and eventual fecal elimination. In a study where 14C-labelled atovaquone was administered to healthy volunteers, greater than 94% of the dose was recovered as unchanged atovaquone in the feces over 21 days. There was little or no excretion of atovaquone in the urine (less than 0.6%). There is indirect evidence that atovaquone may undergo limited metabolism; however, a specific metabolite has not been identified.
Special Populations
Pediatrics
In a study of Atovaquone Suspension in 27 HIV-infected, asymptomatic infants and children between 1 month and 13 years of age, the pharmacokinetics of atovaquone were age dependent. These patients were dosed once daily with food for 12 days. The average steady-state plasma atovaquone concentrations in the 24 patients with available concentration data are shown in Table 1.
This image is provided by the National Library of Medicine.
Hepatic/Renal Impairment
The pharmacokinetics of atovaquone have not been studied in patients with hepatic or renal impairment.
Drug Interactions
Rifampin
In a study with 13 HIV-infected volunteers, the oral administration of rifampin 600 mg every 24 hours with Atovaquone Suspension 750 mg every 12 hours resulted in a 52% ± 13% decrease in the average steady-state plasma atovaquone concentration and a 37% ± 42% increase in the average steady-state plasma rifampin concentration. The half-life of atovaquone decreased from 82 ± 36 hours when administered without rifampin to 50 ± 16 hours with rifampin.
Rifabutin, another rifamycin, is structurally similar to rifampin and may possibly have some of the same drug interactions as rifampin. No interaction trials have been conducted with atovaquone and rifabutin.
Trimethoprim/Sulfamethoxazole (TMP-SMX)
The possible interaction between atovaquone and TMP-SMX was evaluated in 6 HIV-infected adult volunteers as part of a larger multiple-dose, dose-escalation and chronic dosing study of Atovaquone Suspension. In this crossover study, Atovaquone Suspension 500 mg once daily, or TMP-SMX tablets (160 mg trimethoprim and 800 mg sulfamethoxazole) twice daily, or the combination were administered with food to achieve steady-state. No difference was observed in the average steady-state plasma atovaquone concentration after coadministration with TMP-SMX. Coadministration of atovaquone with TMP-SMX resulted in a 17% and 8% decrease in average steady-state concentrations of trimethoprim and sulfamethoxazole in plasma, respectively. This effect is minor and would not be expected to produce clinically significant events.
Zidovudine
Data from 14 HIV-infected volunteers who were given atovaquone tablets 750 mg every 12 hours with zidovudine 200 mg every 8 hours showed a 24% ± 12% decrease in zidovudine apparent oral clearance, leading to a 35% ± 23% increase in plasma zidovudine AUC. The glucuronide metabolite:parent ratio decreased from a mean of 4.5 when zidovudine was administered alone to 3.1 when zidovudine was administered with atovaquone tablets. This effect is minor and would not be expected to produce clinically significant events. Zidovudine had no effect on atovaquone pharmacokinetics.
Relationship Between Plasma Atovaquone Concentration and Clinical Outcome: In a comparative study of atovaquone tablets with TMP-SMX for oral treatment of mild-to-moderate PCP (see INDICATIONS AND USAGE), where AIDS patients received 750 mg atovaquone tablets 3 times daily for 21 days, the mean steady-state atovaquone concentration was 13.9 ± 6.9 mcg/mL (n = 133). Analysis of these data established a relationship between plasma atovaquone concentration and successful treatment. This is shown in Table 2.
This image is provided by the National Library of Medicine.
A dosing regimen of Atovaquone Suspension for the treatment of mild-to-moderate PCP has been selected to achieve average plasma atovaquone concentrations of approximately 20 mcg/mL, because this plasma concentration was previously shown to be well tolerated and associated with the highest treatment success rates (Table 2). In an open-label PCP treatment study with Atovaquone Suspension, dosing regimens of 1,000 mg once daily, 750 mg twice daily, 1,500 mg once daily and 1,000 mg twice daily were explored. The average steady-state plasma atovaquone concentration achieved at the 750-mg twice-daily dose given with meals was 22 ± 10.1 mcg/mL (n = 18).
Nonclinical Toxicology
Carcinogenicity studies in rats were negative; 24-month studies in mice showed treatment-related increases in incidence of hepatocellular adenoma and hepatocellular carcinoma at all doses tested which ranged from 1.4 to 3.6 times the average steady-state plasma concentrations in humans during acute treatment of PCP. Atovaquone was negative with or without metabolic activation in the Ames Salmonella mutagenicity assay, the Mouse Lymphoma mutagenesis assay and the Cultured Human Lymphocyte cytogenetic assay. No evidence of genotoxicity was observed in the in vivo Mouse Micronucleus assay.
Clinical Studies
Prevention of PCP
The indication for prevention of PCP is based on the results of 2 clinical trials comparing Atovaquone Suspension to dapsone or aerosolized pentamidine in HIV-infected adult and adolescent patients at risk of PCP (CD4 count <200 cells/mm3 or a prior episode of PCP) and intolerant to TMP-SMX.
Dapsone Comparative Study: This randomized, open-label trial enrolled a total of 1,057 patients at 48 study centers. Patients were randomized to receive 1,500 mg Atovaquone Suspension once daily (n = 536) or 100 mg dapsone once daily (n = 521). Median follow-up was 24 months. Patients randomized to the dapsone arm who were seropositive for Toxoplasma gondii and had a CD4 count <100 cells/mm3 also received pyrimethamine and folinic acid. PCP event rates are shown in Table 3. There was no significant difference in mortality rates between the groups.
Aerosolized Pentamidine Comparative Study: This randomized, open-label trial enrolled a total of 549 patients at 35 study centers. Patients were randomized to receive 1,500 mg Atovaquone Suspension once daily (n = 175), 750 mg Atovaquone Suspension once daily (n = 188), or 300 mg aerosolized pentamidine once monthly (n = 186). Median follow-up was 11.3 months. The results of the PCP event rates appear in Table 3. There were no significant differences in mortality rates among the groups.
This image is provided by the National Library of Medicine.
An analysis of all PCP events (intent-to-treat analysis) showed results similar to those above.
Treatment of PCP
The indication for treatment of mild-to-moderate PCP is based on the results of comparative pharmacokinetic studies of the suspension and tablet formulations (see CLINICAL PHARMACOLOGY) and clinical efficacy studies of the tablet formulation which established a relationship between plasma atovaquone concentration and successful treatment. The results of a randomized, double-blind trial comparing atovaquone to TMP-SMX in AIDS patients with mild-to-moderate PCP (defined in the study protocol as an alveolar-arterial oxygen diffusion gradient [(A-a)DO2]1≤45 mm Hg and PaO2≥60 mm Hg on room air) and a randomized trial comparing atovaquone to IV pentamidine isethionate in patients with mild-to-moderate PCP intolerant to trimethoprim or sulfa-antimicrobials are summarized below:
TMP-SMX Comparative Study: This double-blind, randomized trial initiated in 1990 was designed to compare the safety and efficacy of atovaquone to that of TMP-SMX for the treatment of AIDS patients with histologically confirmed PCP. Only patients with mild-to-moderate PCP were eligible for enrollment.
A total of 408 patients were enrolled into the trial at 37 study centers. Eighty-six patients without histologic confirmation of PCP were excluded from the efficacy analyses. Of the 322 patients with histologically confirmed PCP, 160 were randomized to receive atovaquone and 162 to TMP-SMX.
Study participants randomized to treatment with atovaquone were to receive 750 mg atovaquone (three 250-mg tablets) 3 times daily for 21 days and those randomized to TMP-SMX were to receive 320 mg TMP plus 1,600 mg SMX 3 times daily for 21 days.
Therapy success was defined as improvement in clinical and respiratory measures persisting at least 4 weeks after cessation of therapy. Therapy failures included lack of response, treatment discontinuation due to an adverse experience and unevaluable.
There was a significant difference (P = 0.03) in mortality rates between the treatment groups. Among the 322 patients with confirmed PCP, 13 of 160 (8%) patients treated with atovaquone and 4 of 162 (2.5%) patients receiving TMP-SMX died during the 21-day treatment course or 8-week follow-up period. In the intent-to-treat analysis for all 408 randomized patients, there were 16 (8%) deaths in the arm treated with atovaquone and 7 (3.4%) deaths in the TMP-SMX arm (P = 0.051). Of the 13 patients treated with atovaquone who died, 4 died of PCP and 5 died with a combination of bacterial infections and PCP; bacterial infections did not appear to be a factor in any of the 4 deaths among TMP-SMX-treated patients.
A correlation between plasma atovaquone concentrations and death was demonstrated; in general, patients with lower plasma concentrations were more likely to die. For those patients for whom day 4 plasma atovaquone concentration data are available, 5 (63%) of the 8 patients with concentrations <5 mcg/mL died during participation in the study. However, only 1 (2%) of the 49 patients with day 4 plasma atovaquone concentrations ≥5 mcg/mL died.
Sixty-two percent of patients on atovaquone and 64% of patients on TMP-SMX were classified as protocol-defined therapy successes (Table 4).
This image is provided by the National Library of Medicine.
The failure rate due to lack of response was significantly larger for patients receiving atovaquone while the failure rate due to adverse experiences was significantly larger for patients receiving TMP-SMX.
There were no significant differences in the effect of either treatment on additional indicators of response (i.e., arterial blood gas measurements, vital signs, serum LDH levels, clinical symptoms and chest radiographs).
Pentamidine Comparative Study
This unblinded, randomized trial initiated in 1991 was designed to compare the safety and efficacy of atovaquone to that of pentamidine for the treatment of histologically confirmed mild or moderate PCP in AIDS patients. Approximately 80% of the patients either had a history of intolerance to trimethoprim or sulfa-antimicrobials (the primary therapy group) or were experiencing intolerance to TMP-SMX with treatment of an episode of PCP at the time of enrollment in the study (the salvage treatment group).
Patients randomized to atovaquone were to receive 750 mg atovaquone (three 250-mg tablets) 3 times daily for 21 days and those randomized to pentamidine isethionate were to receive a 3- to 4-mg/kg single IV infusion daily for 21 days.
A total of 174 patients were enrolled into the trial at 22 study centers. Thirty-nine patients without histologic confirmation of PCP were excluded from the efficacy analyses. Of the 135 patients with histologically confirmed PCP, 70 were randomized to receive atovaquone and 65 to pentamidine. One hundred and ten (110) of these were in the primary therapy group and 25 were in the salvage therapy group. One patient in the primary therapy group randomized to receive pentamidine did not receive study medication.
There was no difference in mortality rates between the treatment groups. Among the 135 patients with confirmed PCP, 10 of 70 (14%) patients randomized to atovaquone and 9 of 65 (14%) patients randomized to pentamidine died during the 21-day treatment course or 8-week follow-up period. In the intent-to-treat analysis for all randomized patients, there were 11 (12.5%) deaths in the arm treated with atovaquone and 12 (14%) deaths in the pentamidine arm. For those patients for whom day 4 plasma atovaquone concentrations are available, 3 of 5 (60%) patients with concentrations <5 mcg/mL died during participation in the study. However, only 2 of 21 (9%) patients with day 4 plasma concentrations ≥5 mcg/mL died.
The therapeutic outcomes for the 134 patients who received study medication in this trial are presented in Table 5.
This image is provided by the National Library of Medicine.
How Supplied
Atovaquone Suspension (bright yellow, citrus flavored) containing 750 mg atovaquone in each teaspoonful (5 mL).
Bottle of 210 mL with child-resistant cap (NDC 65162-693-88).
Store at 15° to 25°C (59° to 77°F). DO NOT FREEZE. Dispense in tight container as defined in USP.
Storage
There is limited information regarding Atovaquone Storage in the drug label.
Images
Drug Images
{{#ask: Page Name::Atovaquone
|?Pill Name
|?Drug Name
|?Pill Ingred
|?Pill Imprint
|?Pill Dosage
|?Pill Color
|?Pill Shape
|?Pill Size (mm)
|?Pill Scoring
|?NDC
|?Drug Author
|format=template
|template=DrugPageImages
|mainlabel=-
|sort=Pill Name
}}





















{kind=link}