In 1970, Aarskog-Scott syndrome (AAS) was first described by Aarskog, a Norwegian pediatrician and human geneticist.
In 1971, Scott described the association between ligamentous laxity which results in hyperextensibility of the fingers, genu recurvatum, flat feet and Aarskog-Scott syndrome (AAS).[1]
In 1973, Sugarman et al described an Mexican-American family in which 2 half brothers and their 2 maternal uncles had Aarskog syndrome.
In 1984, Van den Bergh et al. mentioned a patient with Aarskog-Scott syndrome (AAS) development of syndrome of benign intracranial hypertension after minor headtrauma.[5]
In 1994, Fernandez et al. mentioned 10 Japanese patients who are positive with Aarskog syndrome.[6]
In 1998, Logie and Porteous concluded that in patients with Aarskog-Scott syndrome (AAS) have normal intelligence.[7]
In 2002, Lebel et al. is the one who found a missense mutation in the FGD1 gene.[8]
In 2005, Orrico et al. described attention deficit-hyperactivity disorder (ADHD) in patient with Aarskog-Scott syndrome (AAS).[9]
In 2010, Orrico et al. genetically confirmed 11 patients for Aarskog-Scott syndrome.[10]
Detection of FGD1 mutations. (A) Schematic representation of the domains of the FGD1 protein showing mutations (p.Glu380* and p.Gln664*) identified in patients with AAS. Arrows indicate the positions of the mutated nucleotides in FGD1. (B) sequencing results (p.Glu380* and p.Gln664*) detected in exon 5 and 12, respectively. The altered amino acids are shown in red. Case courtesy by Mariana Pérez-Coria et al[11]
Classification
There is no established system for the classification of Aarskog-Scott syndrome (AAS).[12]
These abnormalities of FGD1/Cdc42 signaling pathway may produce an defective embryonic development and abnormal endochondral and intramembranous bone formation and leads to Aarskog-Scott syndrome (AAS).
Causes
Genetic Cause
Aarskog-Scott syndrome (AAS) is caused by a mutation in the FGD1 gene.
Differentiating Aarskog-Scott syndrome from other Diseases
Patients with clinical features of Aarskog syndrome-(A) Patient 1; note distinctive facial characteristics and interdigital tracts in both hands. (B) Patient 2; discrete facial features and the shawl scrotum can be appreciated. (C) Patient 3 and his mother (patient 8); note prominent forehead, widow's peak, hypertelorism, and fold under the lower lip. (D) Patient 4 with widow's peak, midface hypoplasia, ptosis, clinodactyly, and brachydactyly. (E) Patient 5, brother of patient 4, with distinctive facial features, clinodactyly, and brachydactyly. Case courtesy by Mariana Pérez-Coria et al[44]
History and Symptoms
Common Symptoms
Common symptoms of Aarskog-Scott syndrome (AAS) include:[25][45]
There are no diagnostic laboratory findings associated with Aarskog-Scott syndrome (AAS).
Electrocardiogram
There are no ECG findings associated with Aarskog-Scott syndrome (AAS).
X-Ray Findings
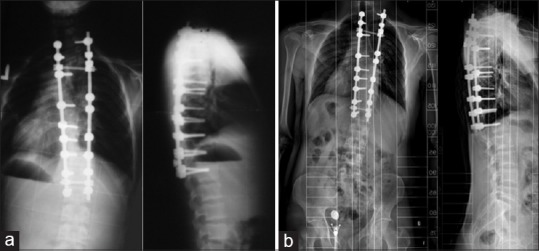
Scoliosis- a) Early postoperative X-ray (b) 10 years follow-up X-ray.Case courtesy Kerim Sariyilmaz[50]There are no x-ray findings associated with Aarskog-Scott syndrome (AAS). However, an x-ray may be helpful in the diagnosis of complications of Aarskog-Scott syndrome (AAS), which include:[51][52]
There are no MRI findings associated with Aarskog-Scott syndrome (AAS).
Medical Therapy
There is no treatment for Aarskog-Scott syndrome (AAS); the mainstay of therapy is symptomatic care.
Patients with short stature are treated with growth hormone, which shows promising results in increasing the height of the patients.[54][55]
Interventions
There are some recommended therapeutic interventions for the management of Aarskog-Scott syndrome (AAS), which includes speech pathologists, audiologists and eye specialists who can improve the quality of the patient's life.
↑Grier, Robert E.; Farrington, Frank H.; Kendig, Robert; Mamunes, Peter; Opitz, John M. (1983). "Autosomal dominant inheritance of the Aarskog syndrome". American Journal of Medical Genetics. 15 (1): 39–46. doi:10.1002/ajmg.1320150105. ISSN0148-7299.
↑Bawle, E.; Tyrkus, M.; Lipman, S.; Bozimowski, D.; Opitz, John M. (1984). "Aarskog syndrome: Full male and female expression associated with an X-autosome translocation". American Journal of Medical Genetics. 17 (3): 595–602. doi:10.1002/ajmg.1320170307. ISSN0148-7299.
↑Zou, Weiguo; Greenblatt, Matthew B.; Shim, Jae-Hyuck; Kant, Shashi; Zhai, Bo; Lotinun, Sutada; Brady, Nicholas; Hu, Dorothy Zhang; Gygi, Steven P.; Baron, Roland; Davis, Roger J.; Jones, Dallas; Glimcher, Laurie H. (2011). "MLK3 regulates bone development downstream of the faciogenital dysplasia protein FGD1 in mice". Journal of Clinical Investigation. 121 (11): 4383–4392. doi:10.1172/JCI59041. ISSN0021-9738.
↑Weinstein, Lee S. (2016). "GNAS and McCune-Albright/Fibrous Dysplasia, Albright Hereditary Osteodystrophy, and Pseudohypoparathyroidism": 1178–1181. doi:10.1093/med/9780199934522.003.0179.
↑Reza Jabalameli, M.; Briceno, Ignacio; Martinez, Julio; Briceno, Ignacio; J. Pengelly, Reuben; Ennis, Sarah; Collins, Andrew (2016). "Aarskog-Scott syndrome: phenotypic and genetic heterogeneity". AIMS Genetics. 3 (1): 49–59. doi:10.3934/genet.2016.1.49. ISSN2377-1143.
↑Reza Jabalameli, M.; Briceno, Ignacio; Martinez, Julio; Briceno, Ignacio; J. Pengelly, Reuben; Ennis, Sarah; Collins, Andrew (2016). "Aarskog-Scott syndrome: phenotypic and genetic heterogeneity". AIMS Genetics. 3 (1): 49–59. doi:10.3934/genet.2016.1.49. ISSN2377-1143.