Bronchopleural fistula: Difference between revisions
Badria Munir (talk | contribs) No edit summary |
Badria Munir (talk | contribs) No edit summary |
||
| Line 2: | Line 2: | ||
{{SI}} | {{SI}} | ||
p{{CMG}} '''Associate Editor-In-Chief:''' | p{{CMG}} '''Associate Editor-In-Chief:''' {{CZ}} | ||
==Overview== | ==Overview== | ||
Revision as of 14:45, 11 August 2019
pEditor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
A bronchopleural fistula (BPF) is a fistula between the pleural space and the bronchial tree. It is a sinus tract between the bronchus and the pleural space that may result from many reasons but most commonly following pneumectomy, or sometimes due to tumors at bronchial margin. It can also occur in response to chemotherapy, radiotherapy COpD, lymph node dissection, long term mechanical ventilation and infections. On imaging, the diagnosis is suspected indirectly on radiograph. Increased gas in the pneumonectomy operative bed, or new gas within a loculated effusion are highly suggestive of the diagnosis. Although radiograph can help in diagnosing it but CT gives a better picture.
It can present with acute or subacute symptoms. It presents with symptoms such as sudden onset dyspnea, chest pain, hemodynamic instability in acute setting. The subacute presentation shows up with emphysema, fever, malaise. Depending on how the patient presents, general suppprtive care and surgical repair are the treatment options.
Pathophysiology
Bronchopleural fistula can occur due to necrotising pneumonia/empyema (anaerobic, pyogenic, tuberculous, and fungal), lung neoplasms, blunt and penetrating lung injuries. It can also occur as a complication of procedures, such as lung biopsy, chest tube drainage, thoracocentesis or may complicate radiation therapy. Most commonly it occurs as a complication of lung surgery. When the bronchial stump fails to heal, a sinus tract is formed between bronchus and pleura, which causes continuous air leak into the pleura. This failure to heal can be from improper initial closure, inadequate blood supply, infection or residual malignant tumour at the bronchial stump.
Epidemiology
The incidence of varies from 4.5% to 20% after pneumonectomy and 0.5% after lobectomy.
Risk
Certain patient characteristics increase this incidence. preoperative radiation to the chest, destroyed or infected lung from inflammatory disease, immunocompromised or immunesuppressed host, diabetes, hypoalbuminemia, cirrhosis, steroid administration, pneumonectomy, right-sided pneumonectomy, a long bronchial stump, residual cancer at the bronchial margin, devascularization of the bronchial stump, prolonged ventilation, or reintubation after resection and surgical inexperience are the factors which may make patient more vulnerable to having BPF. The increased risk of BPF associated with right pneumonectomy is due to the need of more extensive resection required in right pneumonectomy. [1]
Etiology
Bronchopleural fistula mostly develops after lung resection surgery. Some other causes of bronchopleural fistula are
- Right sided surgery[2]
- Chemotherapy and radiation
- Malignancies such as
- Lung cancer
- Thyroid cancer
- Esophageal cancer
- Lymphomas[3]
- Diabetes mellitus[4]
- Gastrointestinal causes such as
- Gastroesophageal reflux disease with Barrett esophagus
- Boerhaave syndrome
- Broncholithiasis
- Heavy smoking and COpD[5]
- Low nutritional status
- Residual tumor at bronchial margin
- Extensive lymph node dissection
- Traumatic and iatrogenic etiologies
- Thoracic trauma with tracheobronchial tree disruption
- Post-surgical (eg. lobectomy or lung biopsy) - by far the most common cause.
- Bougie intubation
- Necrotizing lung disease
- ARDS
- Ventilator-induced barotrauma
- Excessive manual ventilation
- Central line placement
- Complication of bronchoscopy
- Older age
- Long term postoperative mechanical ventilation specially following criteria predisposes patient to BPF
- High suction of the ICC
- High tidal volumes
- High inspiratory pressures
- Tuberculous[6] of fungal infection[7]. Other infections such as
- Haemophilus influenzae
- Streptococcus viridans
- Staphylococcus aureus
- Pseudomona aeruginosa
- Klebsiella pneumoniae
- Pneumococcus
- Nonhemolytic streptococcus
- Aspergillus
- Histoplasma capsulatum
Natural History, Classificatio And Prognosis
Patients with BPF can present with symptoms that range from acute symptoms to subacute symptoms. Most patients present in the first two weeks following lung resection. Bronchopleural fistula occurring postoperatively after lung resection almost always occur within three months of surgery while those developing as a complication of pleuropulmonary infections may develop at any point of time during the course of illness. BPF should be suspected in the postoperative lung resection patient who presents with sudden onset of dyspnea, chest pain, hemodynamic instability, and subcutaneous emphysema. Symptoms may be less abrupt in those who have chest tube placed. In such patients, a large persistent or new air leak through the chest tube drainage system may be the only sign.i
Patients who present in the late postoperative period (more than 14 days) usually present with symptom of empyema. These include fever, malaise, muscle wasting, cough with purulent sputum, reduced air entry and dullness to percussion on the affected side.
Changes in the air-fluid pattern on chest radiograph after surgery are critical as warning signs of BPF. ru Large fistula causing aspiration to the contralateral lung if a tension pneumothorax can develops acute respiratory distresrax. Varoli classified fistulas according to the time of onset after the operation:
- Early [1 to 7 days]
- Intermediate [8 to 30 days]
- Late fistulas [more than 30 days]
Mortality rates vary between 18% to 67%. In BPF the most common cause of death is aspiration pneumonia and subsequent acute respiratory distress syndrome or development of tension pneumothorax.[23] Later development of BPF and larger leaks are among bad prognostic factors. Uie ofsing omental and thoracic flduring surgical repair have shown decreased mortality.
Clinical features
Symptoms can vary from acute, with in first two weeks postoperative period, to subacute ie. >14 days.
Acute Symptoms
- Sudden onset dyspnea
- Chest pain
- Hemodynamic instability
- Subcutaneous emphysema
- Less severe symptoms in case of chest tube (large persistent or new air leak through chest tube drainage might be the only sign
Subacute Symptoms
- Empyema
- Fever
- Malaise
- Muscle wasting
- Cough with purulent sputum
Complication
Following complications can arise due to formation of Bronchopleural fistula.
- failure of lung re-expansion
- loss of a significant amount of each delivered TV
- loss of PEEP
- inappropriate cycling of ventilator
- inability to maintain alveolar ventilation
- Empyema necessitans
- death
Examination
Examination plays a vital role in diagnosing bronchopleural fistula. A careful early examination can lead to early diagnosis and hence good prognosis. Examination should involve the following steps
- Examine the patient (an ABC based primary survey, ensuring that the patient is not about to die of pneumothorax or mediastinal shift and is vitally stable)
- Exclude drain dislodgement (examine the drain)
- Quantify the leak by asking the patient to follow below given instructions.
- Ask the patient to cough
- Ask the patient to speak
- Observe the quantity of bubbles.
- If bubbling is constantly happening while the patient is speaking, the leak is significant.
- If the bubbling is only present with cough and diminishes with ssutained coughing, the leak is probably small.
On auscultation, percussion and checking position of trachea, following findings might be present
- Reduced air entry on affected side
- Dullness to percussion of affected side
- Tracheal deviation (if tension pneumothorax
Diagnosis
The diagnosis must be suspected in a postoperative lung resection patient when there is a
- persistent air-leak (immediate post-operative period)
- a new or increasing air-fluid level
- disappearance of pleural fluid on chest radiograph, if patient has no chest tube in place.
With a delayed BPF, a new air fluid level appears in a previously opacified haemithorax.
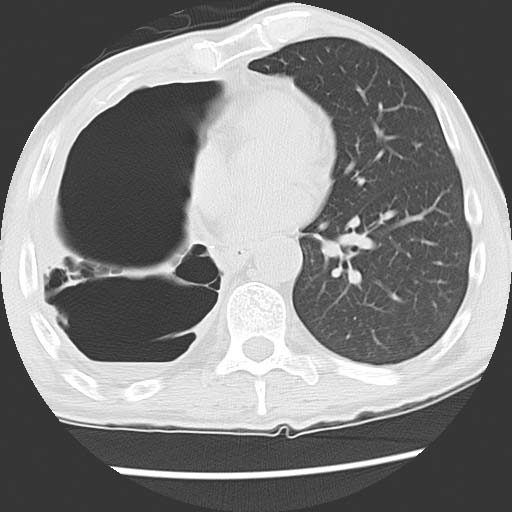
Imaging
Radiological features and CT scan that suggest the presence or the development of a BPF. Following features can be seen on a radiograph but are better appreciated on CT which hints towards formation of BPF
- Increase in intrapleural air space
- Appearance of a new air fluid level
- Changes in an already present air fluid level
- Drop in air fluid level exceeding 2 cm
- Cavity mass in case of malignancy
- pneumothorax
- pneumomediastinum
- Subcutaneous emphysema
- Failure of postpneumonectomy space to fill with fluid
- Air bubbles around surgical side
- Fistula
Bronchoscopy
The presence of BPF is suggested by the return of continuous bubbles during bronchial washing. A bronchoscope with inflation of a balloon-tipped catheter into selected airways can aid in localization, as balloon occlusion decreases or eliminates an air. Small metallic probes introduced through the working channel of the bronchoscope, and changes in gas concentration in the pneumonectomy cavity after inhaling different concentrations of oxygen and N2O are also useful. It can help in determining
- proper evaluation of stump
- Surgical site
- Fistula size and site
- Mucosal defect
- Localization of fistula by instilling dye
- Rule out other etiologies
While a large BPF is more likely to be seen on bronchoscopy, sequential balloon occlusion of the bronchi is sometimes used, particularly for the localization of a smaller or segmental BPF.
CT Bronchography
Computed tomography bronchography (CTB) has been used to diagnose difficult BPF. 20 to 30 mL of a water-based nonionic low osmolar iodinated contrast medium iois injected hexol at the suspected fistula site following bronchoscopy either through a catheter or directly through the working channel of the bronchoscope . The fistula was easily visualized using standard axial and sagittal se on CT.
Capnography
Capnography can be used to identify the bronchial segment related to BPF. End-tidal carbon dioxide is measured by connecting a capnograph to a polyethylene catheter and has a reported a sensitivity of 83% and a specificity of 100% in the diagnosis of BPF.[8]
Pulsography
Endoscopic monitoring of pulse blood flow in the bronchial stump after pneumonectomy is a reliable method of prediction of the BPF with the probability of 77.2% It is one of the latest modality in diagnosing BPF. [9]
Differential Diagnosis
Reasons for tension pneumothorax in postoperative period can be
- Blocked or displaced chest tube
- Tension Chylothorax
- Hemothorax
- Signs of empyema can be due to infection as well.
Management
General Supportive Care
These measures are usually practiced when bronchopleural fistula has subacute presentation. Drainage of air from pleural space by chest tube thoracostomy. If fluid is collected, it should be sent for following labs
- Cell count
- pH
- Total protein
- LDH
- Glucose
- Cytology
- Triglycerides
- Gram Stains
- Culture
Asses the patient for empyema[10] and treat him for it.
- Broad spectrum intravenous antibiotics until gram stains, culture and sensitivity is available
- Intrapleural fibrinolytic for patients with infected multi loculated effusions
- postural drainage
Maximize nutrition
Treat other co morbidities
- For mechanically ventilated patient, lower the level of positive pressure and selectively intubate healthy lung. Thihe advantages and disadvantages of some of the above mentioned measures are discussed bel.a.
| rategyt | vantagesd | Disadvantages | |
|---|---|---|---|
| h |
|
|
|
|
|
|
|
Independent Lung Ventilation
|
|
|
Surgical Repair
Surgical repair is usually done in patients if symptoms of bronchopleural effusion arise after lung resection.
| patient | procedure | Indication | Contraindication |
|---|---|---|---|
| Acute symptoms |
|
|
Wait until extubation in patients with
|
| Subacute symptoms | Time to bridge period before surgery by
|
|
Bronchoscopic therapies and general measures does not work for large fistulas |
Bronchoscopic therapies are performed depending on size of the fistula. Advantages and disadvantages of some of the invasive strategies have been given below.
| Strategy | Advantages | Disadvantage | |
|---|---|---|---|
| Surgical Repair |
|
|
|
| Bronchial Stenting |
|
|
|
| Bronchial Occlusion | Similarly to surgery, the affected bronchus is blocked with either a one-way valve or a plug. Other options includes blood clot, cyanoacrylate glue, fibrin, lead shot, gel foam, calf bone, and various others. |
|
|
| Application Of PEEP to ICC |
|
|
|
| OVF |
|
|
|
| ECMO |
|
|
Refractory Cases

For refractory patients, following interventions could be done.
- Repeat surgery
- Alternate bronchoscopic mathod
- Open window thoracostomy[15]
Follow Up
Monitor
- Clinical symptoms of recurrence
- Chest tube air output
- Radiograph and CT
Bronchoscopy is done if symptoms reappear.
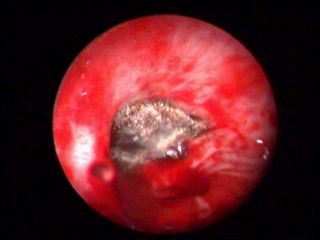
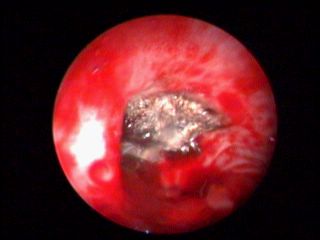
shown below are courtesy of Sedat Altin MD, Levent Dalar MD and Cafer Zorkun MD from Yedikule Education and Research Hospital, Istanbul - Turkey.
-

Bronchoscopy: Bronchopleural Fistula
-

Bronchoscopy: Bronchopleural Fistula
-
Bronchoscopy: Bronchopleural Fistula
-
Bronchoscopy: Bronchopleural Fistula




-

Pre fistula radiograph
-

-

-

-





References
- ↑ https://www.ncbi.nlm.nih.gov/pubmed/11309718. Missing or empty
|title=(help) - ↑ https://www.ncbi.nlm.nih.gov/pubmed/29516277. Missing or empty
|title=(help) - ↑ https://en.wikipedia.org/wiki/Bronchopleural_fistula. Missing or empty
|title=(help) - ↑ https://www.ncbi.nlm.nih.gov/pubmed/27063612. Missing or empty
|title=(help) - ↑ https://www.ncbi.nlm.nih.gov/pubmed/27499951. Missing or empty
|title=(help) - ↑ https://www.ncbi.nlm.nih.gov/pubmed/29516277. Missing or empty
|title=(help) - ↑ https://www.ncbi.nlm.nih.gov/pubmed/25019431. Missing or empty
|title=(help) - ↑ https://www.ncbi.nlm.nih.gov/books/NBK534765/. Missing or empty
|title=(help) - ↑ https://academic.oup.com/icvts/article/23/suppl_1/i18/2487499. Missing or empty
|title=(help) - ↑ https://www.ncbi.nlm.nih.gov/pubmed/30054070. Missing or empty
|title=(help) - ↑ https://www.ncbi.nlm.nih.gov/pubmed/29348280. Missing or empty
|title=(help) - ↑ https://www.ncbi.nlm.nih.gov/pubmed/29109057. Missing or empty
|title=(help) - ↑ https://www.ncbi.nlm.nih.gov/pubmed/29587951. Missing or empty
|title=(help) - ↑ https://www.ncbi.nlm.nih.gov/pubmed/29443771. Missing or empty
|title=(help) - ↑ [https://www.ncbi.nlm.nih.gov/pubmed/23525638
https://www.ncbi.nlm.nih.gov/pubmed/26743783
https://www.ncbi.nlm.nih.gov/pubmed/27220922
https://www.ncbi.nlm.nih.gov/pubmed/29109057 https://www.ncbi.nlm.nih.gov/pubmed/23525638 https://www.ncbi.nlm.nih.gov/pubmed/26743783 https://www.ncbi.nlm.nih.gov/pubmed/27220922 https://www.ncbi.nlm.nih.gov/pubmed/29109057] Check
|url=value (help). line feed character in|url=at position 45 (help); Missing or empty|title=(help)