Endoscopic foreign body retrieval
Template:DiseaseDisorder infobox
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Endoscopic foreign body retrieval refers to the removal of ingested objects from the esophagus, stomach and duodenum by endoscopic techniques. It does not involve surgery, but rather encompasses a variety of techniques employed through the gastroscope for grasping foreign bodies, manipulating them, and removing them while protecting the esophagus and trachea.[1] It is of particular importance with children,[2] people with mental illness,[3] and prison inmates[4] as these groups have a high rate of foreign body ingestion.
Differential diagnosis of common foreign bodies
Commonly swallowed objects include coins, buttons, batteries, and small bones (such as fish bones),[1] but can include more complex objects, such as eyeglasses,[5] spoons,[6] and toothbrushes[5] (see image).
Indications and contraindications
Some patients at risk for foreign body ingestion may not be able to give an accurate medical history of ingestion, either due to age or mental illness. It is important that physicians treating these patients recognize the symptoms of esophageal foreign body impaction requiring urgent intervention. Most frequently, these include drooling and the inability to swallow saliva, neck tenderness, regurgitation of food, stridor and shortness of breath if there is compression of the trachea.[1][7]
There are several situations in which endoscopic techniques are not indicated, such as for small blunt objects less than 2.5 cm which have already passed into the stomach (as these usually do not obstruct anywhere else), when there is perforation of the esophagus or mediastinitis (inflammation of structures around the esophagus), and for narcotic-containing bags or condoms that have been ingested, because of the risk of overdose if they are ruptured.[1]
Foreign bodies should be removed from the esophagus within 24 hours of ingestion because of a high risk of complication.[8]
Non-invasive testing
Prior to undertaking endoscopy, attempts should be made to locate the foreign body with x-rays or other non-invasive techniques.[1] For radio-opaque objects, x-rays of the neck, chest and abdomen can be used to locate the foreign body and assist endoscopy.[9] Alternative approaches, including the use of metal detectors, have also been described. [10]
X-rays are also useful for identifying the type of foreign body ingested and complications of foreign body ingestion, including mediastinitis and perforation of the esophagus.[1]
Endoscopy
Endoscopic retrieval involves the use of a gastroscope or an optic fiber charge-coupled device camera. This instrument is shaped as a long tube, which is inserted through the mouth into the esophagus and stomach to identify the foreign body or bodies. This procedure is typically performed under conscious sedation. Many techniques have been described to remove foreign bodies from the stomach and esophagus. Usually the esophagus is protected with an overtube (a plastic tube of varying length), through which the gastroscope and retrieved objects are passed.[11]
Once the foreign body has been identified with the gastroscope, various devices can be passed through the gastroscope to grasp or manipulate the foreign body. Devices used include forceps, which come in varying shapes, sizes and grips,[12] snares, and oval loops that can be retracted from outside the gastroscope to lasso objects,[13] as well as Roth baskets (mesh nets that can be closed to trap small objects), [14] and magnets placed at the end of the scope or at the end of orogastric tubes.[12][15] Some techniques have been described that use foley catheters to trap objects, or use two snares to orient foreign bodies.[6]
Examples
<
-
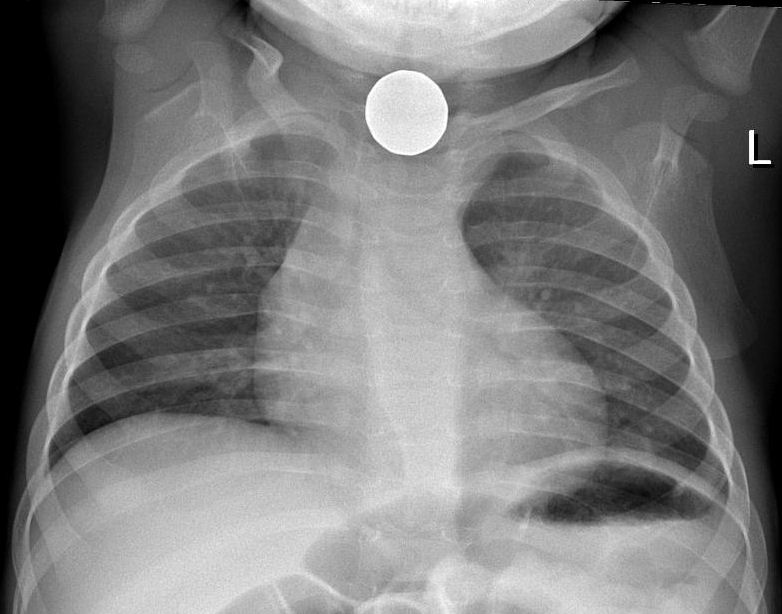 Chest X-ray showing a coin in the esophagus of a young child
Chest X-ray showing a coin in the esophagus of a young child -

-

-

-
 A screwdriver with a plastic handle. (Dr. A.K. Sharma, Agra, India
A screwdriver with a plastic handle. (Dr. A.K. Sharma, Agra, India -

-
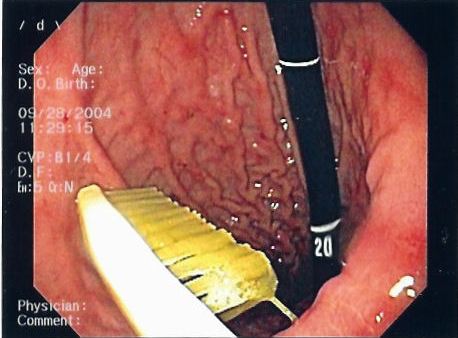 Gastric foreign body (toothbrush)
Gastric foreign body (toothbrush) -

-

-

-
 Gastric foreign body (toothbrush)
Gastric foreign body (toothbrush) -
 Rectal foreign body (Image courtesy of Dr Frank Gaillard)
Rectal foreign body (Image courtesy of Dr Frank Gaillard) -
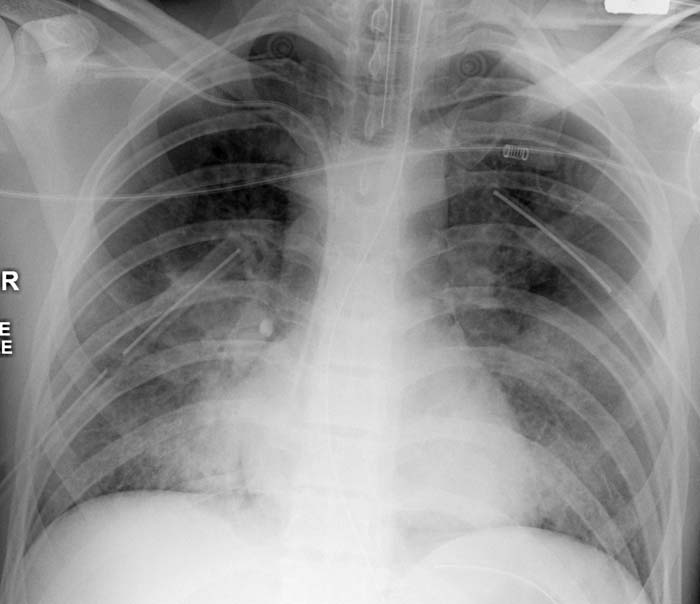
 This patient collapsed on the ward and was thought to have had a pulmonary embolus. A CTPA revealed a tablet lying dependently in the patient's trachea, with changes of aspiration in both lower lobes (not shown). A second tablet was visible in the stomach... the tablet was removed via a bronchoscope and confirmed to be a Slow K (potassium). (Image courtesy of Dr Frank Gaillard)
This patient collapsed on the ward and was thought to have had a pulmonary embolus. A CTPA revealed a tablet lying dependently in the patient's trachea, with changes of aspiration in both lower lobes (not shown). A second tablet was visible in the stomach... the tablet was removed via a bronchoscope and confirmed to be a Slow K (potassium). (Image courtesy of Dr Frank Gaillard) -
 This patient collapsed on the ward and was thought to have had a pulmonary embolus. A CTPA revealed a tablet lying dependently in the patient's trachea, with changes of aspiration in both lower lobes (not shown). A second tablet was visible in the stomach... the tablet was removed via a bronchoscope and confirmed to be a Slow K (potassium). (Image courtesy of Dr Frank Gaillard)
This patient collapsed on the ward and was thought to have had a pulmonary embolus. A CTPA revealed a tablet lying dependently in the patient's trachea, with changes of aspiration in both lower lobes (not shown). A second tablet was visible in the stomach... the tablet was removed via a bronchoscope and confirmed to be a Slow K (potassium). (Image courtesy of Dr Frank Gaillard) -
 This patient collapsed on the ward and was thought to have had a pulmonary embolus. A CTPA revealed a tablet lying dependently in the patient's trachea, with changes of aspiration in both lower lobes (not shown). A second tablet was visible in the stomach... the tablet was removed via a bronchoscope and confirmed to be a Slow K (potassium). (Image courtesy of Dr Frank Gaillard)
This patient collapsed on the ward and was thought to have had a pulmonary embolus. A CTPA revealed a tablet lying dependently in the patient's trachea, with changes of aspiration in both lower lobes (not shown). A second tablet was visible in the stomach... the tablet was removed via a bronchoscope and confirmed to be a Slow K (potassium). (Image courtesy of Dr Frank Gaillard) -
 Rectal foreign body (Image courtesy of Dr Frank Gaillard)
Rectal foreign body (Image courtesy of Dr Frank Gaillard) -
 Vaginal foreign body (Image courtesy of Dr Donna D'Souza)
Vaginal foreign body (Image courtesy of Dr Donna D'Souza) -
 This patient presented with a self-harm injury. The axial CT scan shows a ball-point pen in-situ. The pen missed optic nerve, middle cerebral artery and any eloquent brain. A cerebral angiogram was performed which was normal except for truncation of the ophthalmic artery. The pen was removed under flouroscopic guidance. Upon removal, there was brisk bleeding from the ophthalmic artery. Endovascular embolisation of the bleeding vessel was performed with coils, with good result. The patient’s pupil remains reactive, suggesting a good prognosis for the optic nerve and the patient’s vision. (Image courtesy of Dr Laughlin Dawes)
This patient presented with a self-harm injury. The axial CT scan shows a ball-point pen in-situ. The pen missed optic nerve, middle cerebral artery and any eloquent brain. A cerebral angiogram was performed which was normal except for truncation of the ophthalmic artery. The pen was removed under flouroscopic guidance. Upon removal, there was brisk bleeding from the ophthalmic artery. Endovascular embolisation of the bleeding vessel was performed with coils, with good result. The patient’s pupil remains reactive, suggesting a good prognosis for the optic nerve and the patient’s vision. (Image courtesy of Dr Laughlin Dawes) -
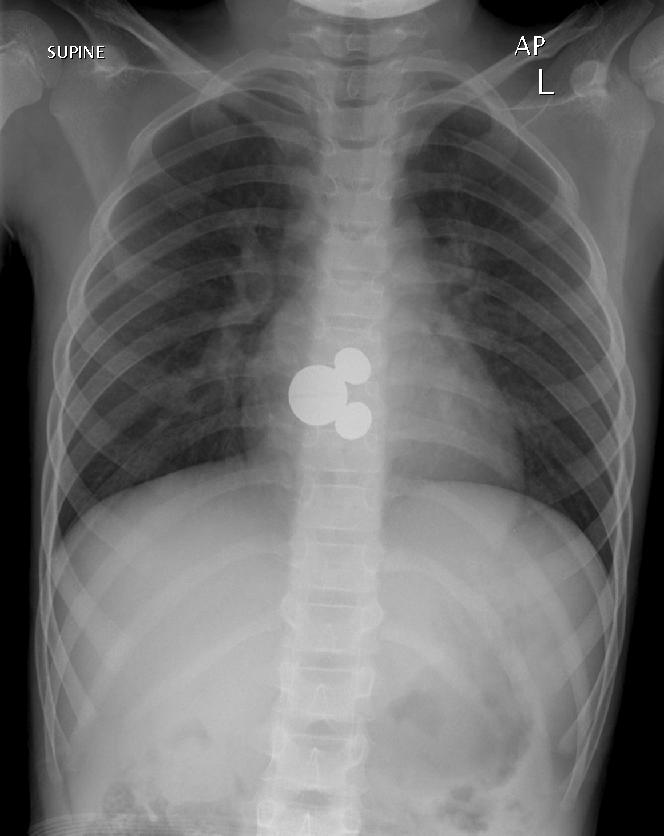 A 7 year old girl presented to ED after swallowing a foreign body. Initial CXR shows a foreign body at the level of T8. There was no change in the position of the Mickey Mouse key ring after 8 hours. No pneumomediastinum or pneumothorax. The airway is patent. It was finally retrieved with oesophagoscopy. (Image courtesy of Dr Lily Wang)
A 7 year old girl presented to ED after swallowing a foreign body. Initial CXR shows a foreign body at the level of T8. There was no change in the position of the Mickey Mouse key ring after 8 hours. No pneumomediastinum or pneumothorax. The airway is patent. It was finally retrieved with oesophagoscopy. (Image courtesy of Dr Lily Wang) -
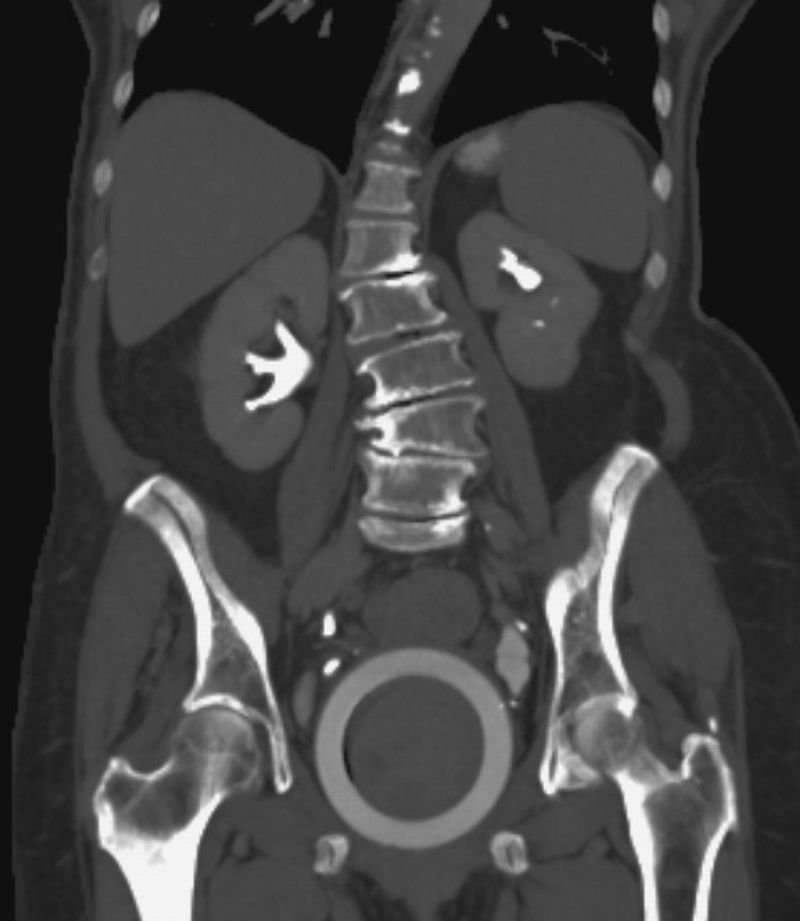
 A middle-aged male presented to the emergency department with abdominal discomfort. An abdominal radiograph was performed as shown. There is no evidence of perforation or obstruction. The patient was taken to operating room within 12 hours of presentation, with consent for colostomy. Under general anaesthesia in the lithotomy position, dilatation of anal sphincter was performed and per rectum retrieval successful. These patients typically have a delayed presentation to the emergency department because of embarrassment and after multiple attempts at self removal. Respect for their privacy is a key factor in the patient’s care plan. ED physicians need to decide if removal of foreign body can be performed in the emergency department or surgical team to be notified. Operating room procedures include anal dilatation under GA, transrectal manipulation, bimanual palpation if necessary and withdrawal of foreign body. Laparotomy or laparoscopy are occasionally necessary. (Image courtesy of Andrew Roshan)
A middle-aged male presented to the emergency department with abdominal discomfort. An abdominal radiograph was performed as shown. There is no evidence of perforation or obstruction. The patient was taken to operating room within 12 hours of presentation, with consent for colostomy. Under general anaesthesia in the lithotomy position, dilatation of anal sphincter was performed and per rectum retrieval successful. These patients typically have a delayed presentation to the emergency department because of embarrassment and after multiple attempts at self removal. Respect for their privacy is a key factor in the patient’s care plan. ED physicians need to decide if removal of foreign body can be performed in the emergency department or surgical team to be notified. Operating room procedures include anal dilatation under GA, transrectal manipulation, bimanual palpation if necessary and withdrawal of foreign body. Laparotomy or laparoscopy are occasionally necessary. (Image courtesy of Andrew Roshan) -
 Rectal foreign body. Body packer. (Image courtesy of Dr Frank Gaillard)
Rectal foreign body. Body packer. (Image courtesy of Dr Frank Gaillard) -
 Rectal foreign body (Image courtesy of Dr Frank Gaillard)
Rectal foreign body (Image courtesy of Dr Frank Gaillard) -
 Rectal foreign body (Image courtesy of Dr Frank Gaillard)
Rectal foreign body (Image courtesy of Dr Frank Gaillard) -
 Rectal foreign body (Image courtesy of Dr Frank Gaillard)
Rectal foreign body (Image courtesy of Dr Frank Gaillard) -
 (Image courtesy of Simon Pilgrim and Laughlin Dawes)
(Image courtesy of Simon Pilgrim and Laughlin Dawes) -
 Vaginal pessary for treatment of uterine prolapse (Image courtesy of Dr Frank Gaillard)
Vaginal pessary for treatment of uterine prolapse (Image courtesy of Dr Frank Gaillard) -
 This building-site worker inadvertently stapled-gunned his hand, neatly sitting in his interosseous space. (Image courtesy of Dr Frank Gaillard)
This building-site worker inadvertently stapled-gunned his hand, neatly sitting in his interosseous space. (Image courtesy of Dr Frank Gaillard) -
 This trauma patient had significant craniofacial injuries and aspirated a tooth. It lodged in the right lower lobe bronchus, causing post-obstructive consolidation. Inhaled foreign bodies may be complicated by haemoptysis, air trapping, post-obstructive collapse, pneumonia or bronchiectasis. Removal of the foreign body is usually performed via bronchoscopy. (Image courtesy of Dr Donna D'Souza)
This trauma patient had significant craniofacial injuries and aspirated a tooth. It lodged in the right lower lobe bronchus, causing post-obstructive consolidation. Inhaled foreign bodies may be complicated by haemoptysis, air trapping, post-obstructive collapse, pneumonia or bronchiectasis. Removal of the foreign body is usually performed via bronchoscopy. (Image courtesy of Dr Donna D'Souza) -
 This patient was transfered to ICU from another hospital. On examination of their abdomen a wire was noted to project through the right atrium, down the IVC to end in the right iliac vein. The J-shaped tip gave the game away... a right jugular CVC had been placed, and the wire used for the insertion pushed in with the catheter. This guide wire was successfully retrieved from the groin, without complication. (Image courtesy of Dr Frank Gaillard)
This patient was transfered to ICU from another hospital. On examination of their abdomen a wire was noted to project through the right atrium, down the IVC to end in the right iliac vein. The J-shaped tip gave the game away... a right jugular CVC had been placed, and the wire used for the insertion pushed in with the catheter. This guide wire was successfully retrieved from the groin, without complication. (Image courtesy of Dr Frank Gaillard) -
 This patient was transfered to ICU from another hospital. On examination of their abdomen a wire was noted to project through the right atrium, down the IVC to end in the right iliac vein. The J-shaped tip gave the game away... a right jugular CVC had been placed, and the wire used for the insertion pushed in with the catheter. This guide wire was successfully retrieved from the groin, without complication. (Image courtesy of Dr Frank Gaillard)
This patient was transfered to ICU from another hospital. On examination of their abdomen a wire was noted to project through the right atrium, down the IVC to end in the right iliac vein. The J-shaped tip gave the game away... a right jugular CVC had been placed, and the wire used for the insertion pushed in with the catheter. This guide wire was successfully retrieved from the groin, without complication. (Image courtesy of Dr Frank Gaillard)






























See also
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 Eisen GM, Baron TH, Dominitz JA, Faigel DO, Goldstein JL, Johanson JF, Mallery JS, Raddawi HM, Vargo JJ 2nd, Waring JP, Fanelli RD, Wheeler-Harbough J; American Society for Gastrointestinal Endoscopy. Guideline for the management of ingested foreign bodies. Gastrointest Endosc. 2002 Jun;55(7):802-6. PMID 12024131
- ↑ Kay M, Wyllie R. Pediatric foreign bodies and their management. Curr Gastroenterol Rep. 2005 Jun;7(3):212-8. PMID 15913481.
- ↑ Webb WA. Management of foreign bodies of the upper gastrointestinal tract: update. Gastrointest Endosc. 1995 Jan;41(1):39-51. PMID 7698623
- ↑ O'Sullivan ST, Reardon CM, McGreal GT, Hehir DJ, Kirwan WO, Brady MP. Deliberate ingestion of foreign bodies by institutionalised psychiatric hospital patients and prison inmates. Ir J Med Sci. 1996 Oct-Dec;165(4):294-6.
- ↑ 5.0 5.1 Grover SC, Kim YI, Kortan PP, Marcon NE. Endoscopic removal of eight gastric foreign bodies ingested sequentially in twelve days: a case of creative endoscopy. Abstract presented at World Congress of Gastroenterology, Montreal, Canada, September 2005.
- ↑ 6.0 6.1 Aoyagi K, Maeda K, Morita I, Eguchi K, Nishimura H, Sakisaka S. Endoscopic removal of a spoon from the stomach with a double-snare and balloon. Gastrointest Endosc. 2003 Jun;57(7):990-1. PMID 12776067
- ↑ Nandi P, Ong GB. Foreign body in the oesophagus: review of 2394 cases. Br J Surg. 1978 Jan;65(1):5-9. PMID 623968
- ↑ Chaikhouni A, Kratz JM, Crawford FA. Foreign bodies of the esophagus. Am Surg. 1985 Apr;51(4):173-9. PMID 3985482
- ↑ Lane JE, Boltri JM. Imaging gastric pennies in children. Emerg Radiol. 2005 Apr;11(3):180-2. PMID 16028326
- ↑ Ramlakhan SL, Burke DP, Gilchrist J. Things that go beep: experience with an ED guideline for use of a handheld metal detector in the management of ingested non-hazardous metallic foreign bodies. Emerg Med J. 2006 Jun;23(6):456-60. PMID 16714508
- ↑ Smith MT, Wong RK. Esophageal foreign bodies: types and techniques for removal. Curr Treat Options Gastroenterol. 2006 Feb;9(1):75-84.
- ↑ 12.0 12.1 Seo JK. Endoscopic management of gastrointestinal foreign bodies in children. Indian J Pediatr. 1999;66(1 Suppl):S75-80. PMID 11132474
- ↑ Chen SC, Yu SC, Yuan RH, Chang KJ. Endoscopic removal of a large gastric metallic watch with a polypectomy snare loop. Endoscopy. 1997 Nov; 29(9):S55-6. PMID 9476781
- ↑ Neustater B, Barkin JS. Extraction of an esophageal food impaction with a Roth retrieval net. Gastrointest Endosc. 1996 Jan;43(1):66-7. PMID 8903823.
- ↑ Yamauchi K, Kobayashi T, Shinomiya T, Fujiwara D, Ito W, Onoda T, Yozai K, Ishii T, Nanamiya W, Sumiyoshi R, Ono T, Tamai M, Yamane Y, Suzaki N. Device for the removal of button batteries. Intern Med. 2001 Jan;40(1):9-13. PMID 11201377
External links
- Esophageal Coin MedPix Topic
- Cynsa's Rectal Foreign Bodies page
- eMedicine gastrointestinal emergency medicine
- Medical Journal of Australia
- Royal College of Surgeons of Edinburgh
- British Dental Journal case report: Don't forget your toothbrush! (subscribers only - with useful bibliography)