Pulmonary embolism electrocardiogram: Difference between revisions
| Line 24: | Line 24: | ||
Image:V18.ht22.jpg|ECG of a patient with pulmonary embolism showing S1-Q3 and signs of right frontal axis deviation. <small>Image courtesy of Dr Jose Ganseman [http://www.ganseman.com/ecgbibnl.htm#_top000 Dr Ganseman's webpage: An ultimate source of EKG]</small> | Image:V18.ht22.jpg|ECG of a patient with pulmonary embolism showing S1-Q3 and signs of right frontal axis deviation. <small>Image courtesy of Dr Jose Ganseman [http://www.ganseman.com/ecgbibnl.htm#_top000 Dr Ganseman's webpage: An ultimate source of EKG]</small> | ||
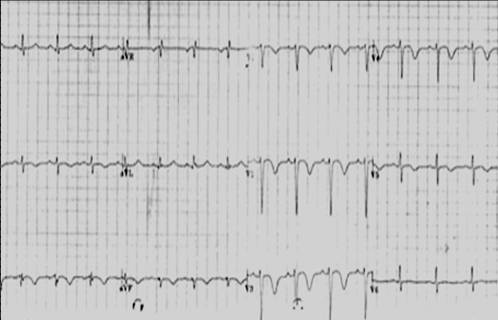
Image:picture1.jpg|ECG of patient with pulmonary embolism showing S1 Q3 T3, Right bundle branch block pattern and flipped anterior T waves.</small> | Image:picture1.jpg|ECG of patient with pulmonary embolism showing S1 Q3 T3, Right bundle branch block pattern and flipped anterior T waves.</small> | ||
Image:Pulmonary_embolism,_T_wave.jpg|Most common ECG finding in pulmonary embolism is anterior T wave inversion.</small> | |||
</gallery> | </gallery> | ||
</div> | </div> | ||
Revision as of 04:00, 23 September 2012
|
Pulmonary Embolism Microchapters |
|
Diagnosis |
|---|
|
Pulmonary Embolism Assessment of Probability of Subsequent VTE and Risk Scores |
|
Treatment |
|
Follow-Up |
|
Special Scenario |
|
Trials |
|
Case Studies |
|
Pulmonary embolism electrocardiogram On the Web |
|
Directions to Hospitals Treating Pulmonary embolism electrocardiogram |
|
Risk calculators and risk factors for Pulmonary embolism electrocardiogram |
Editor(s)-In-Chief: The APEX Trial Investigators, C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
ECG abnormalities occur in both PE and non-PE patients in the absence of preexisting cardiovascular disease, thus limiting the use of ECG in diagnosing a pulmonary embolism.[1][2] ECG findings may also be normal in the setting of a PE. A prospective study reported 70% of acute PE patients to have ECG abnormalities, which were most commonly nonspecific ST-segment and T-wave changes.[3]
Electrocardiogram
An electrocardiogram (ECG) is routinely done on all patients with chest pain to assess for a myocardial infarctions.
- The most common ECG abnormality seen in PE patients is an anterior T-wave inversion.[4] This likely represents reciprocal changes of infero-posterior ischemia due to compression of the right coronary artery (RCA), caused by pressure overload in the right ventricle (RV).
- Sinus tachycardia and right bundle branch block (RBBB) are also commonly seen, and are not sensitive or specific.
- Signs of right heart strain or acute cor pulmonale may be present in cases of large PEs. The classic sign of (S1Q3T3) will show a large S wave in lead I, a large Q wave in lead III and an inverted T wave in lead III .[5][6] This can be present in up to 20% of patients, but is also seen in other acute pulmonary conditions and is therefore of limited diagnostic value.
Sinus tachycardia is the most common ECG finding in the setting of a pulmonary embolism, but lacks specificity in the clinical setting.[7]
The presence of Q waves in anterior leads with ST-elevation following a PE has also been described in few case reports.[8]
-
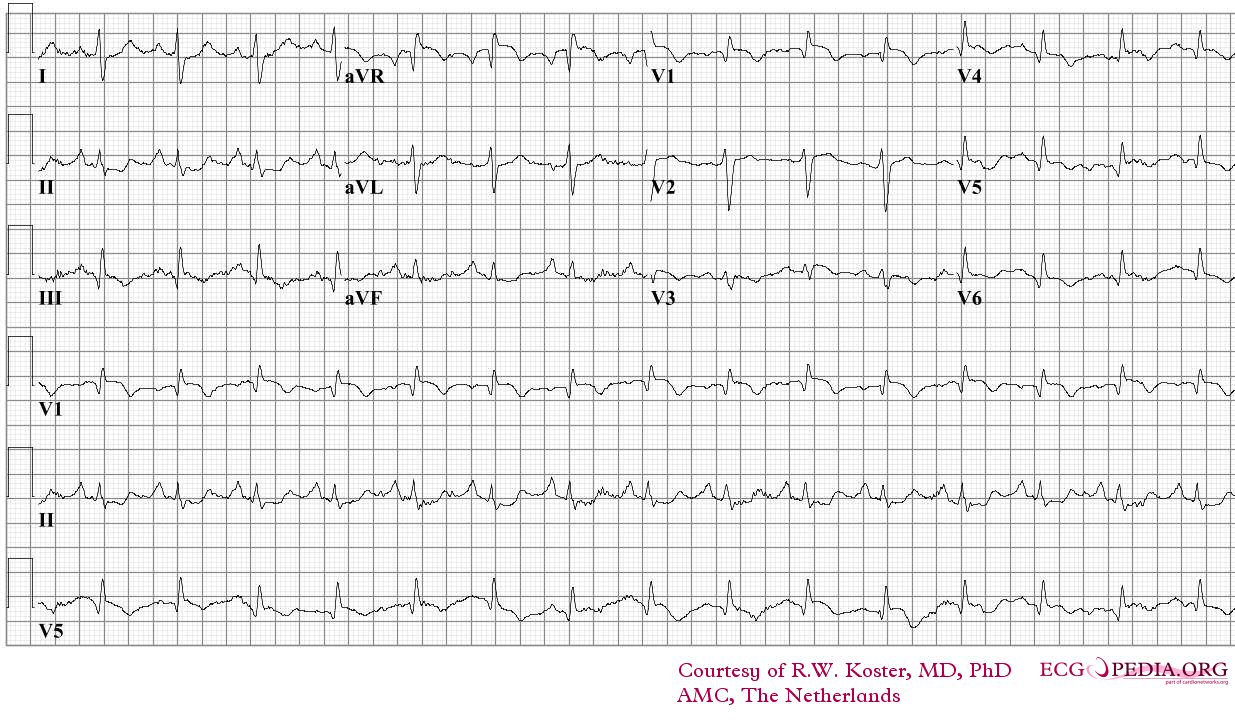
ECG of a patient with a pulmonary embolism. Image courtesy of ecgpedia
-
ECG of a patient with pulmonary embolism showing sinus tachycardia and right axis deviation.Image courtesy of ecgpedia
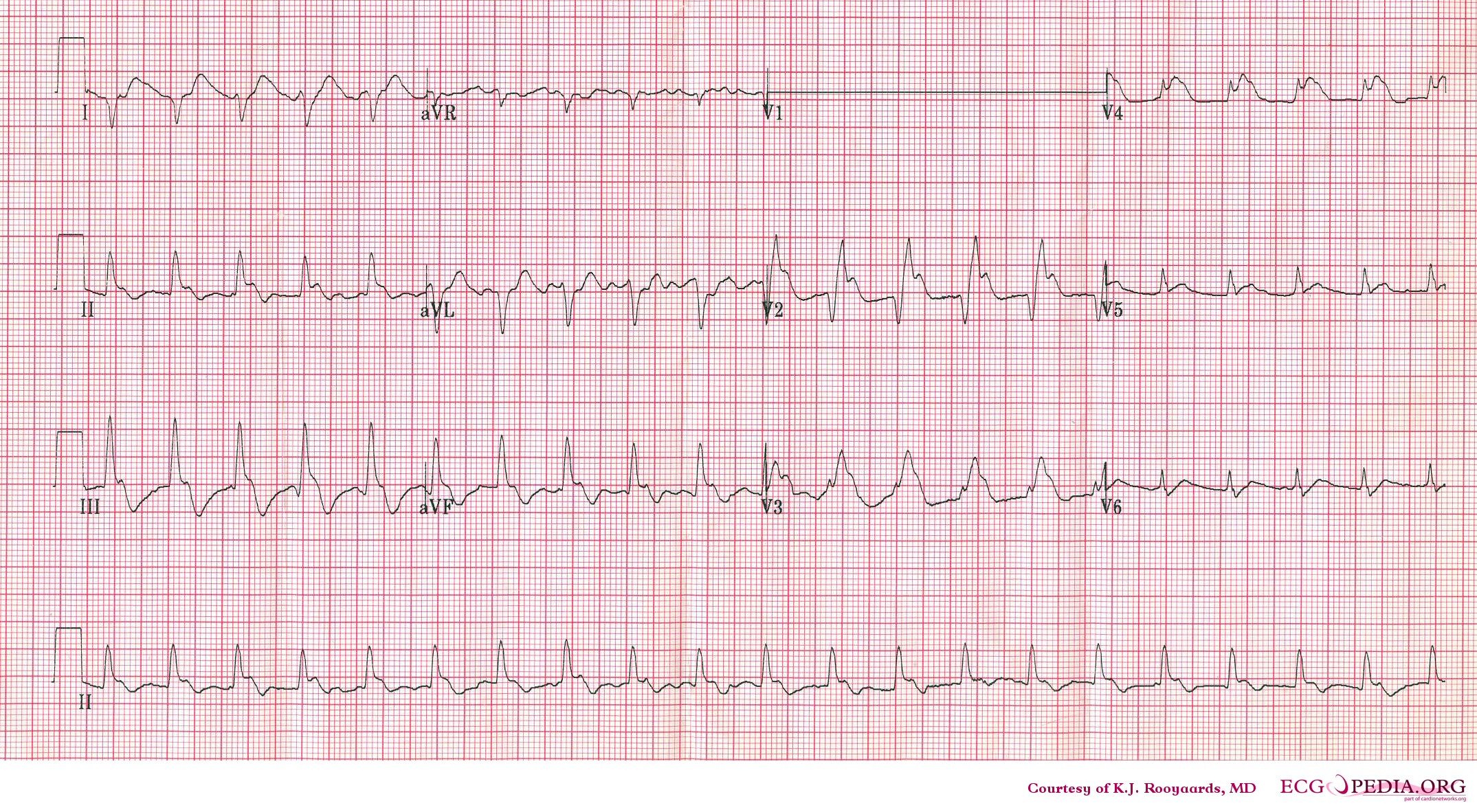
-
ECG of a patient with pulmonary embolism showing S1-Q3 and signs of right frontal axis deviation. Image courtesy of Dr Jose Ganseman Dr Ganseman's webpage: An ultimate source of EKG
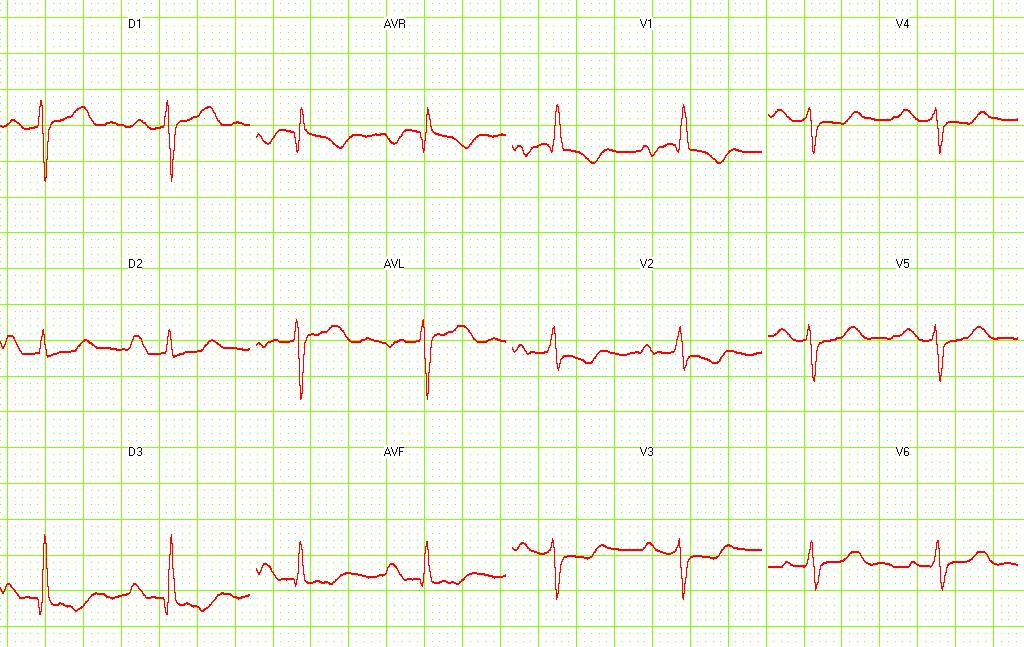
-
ECG of patient with pulmonary embolism showing S1 Q3 T3, Right bundle branch block pattern and flipped anterior T waves.
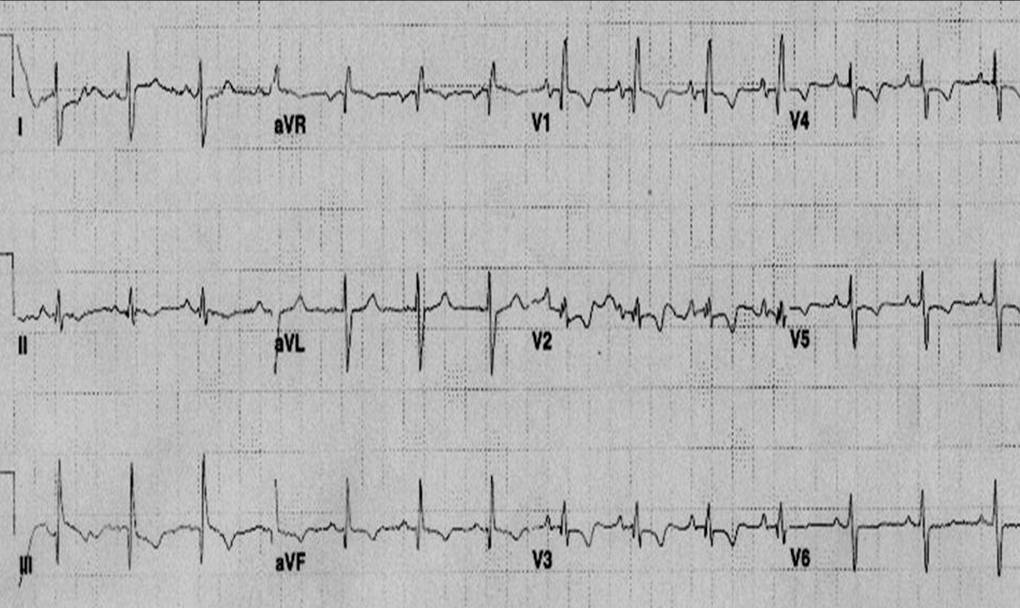
-
Most common ECG finding in pulmonary embolism is anterior T wave inversion.





Prognostic Assessment
ECG findings that are associated with a poor prognosis are:[4]
- Atrial arrhythmias
- Right bundle branch block
- Q-waves in the inferior leads
- Precordial T-wave inversion and ST-segment changes.
- Development of a QR wave in lead V1 is identified as an independent risk factor for an adverse prognosis.[9]
References
- ↑ Geibel A, Zehender M, Kasper W, Olschewski M, Klima C, Konstantinides SV (2005). "Prognostic value of the ECG on admission in patients with acute major pulmonary embolism". Eur Respir J. 25 (5): 843–8. doi:10.1183/09031936.05.00119704. PMID 15863641.
- ↑ Rodger M, Makropoulos D, Turek M, Quevillon J, Raymond F, Rasuli P; et al. (2000). "Diagnostic value of the electrocardiogram in suspected pulmonary embolism". Am J Cardiol. 86 (7): 807–9, A10. PMID 11018210.
- ↑ Stein PD, Saltzman HA, Weg JG (1991). "Clinical characteristics of patients with acute pulmonary embolism". Am J Cardiol. 68 (17): 1723–4. PMID 1746481.
- ↑ 4.0 4.1 Ferrari E, Imbert A, Chevalier T, Mihoubi A, Morand P, Baudouy M (1997). "The ECG in pulmonary embolism. Predictive value of negative T waves in precordial leads--80 case reports". Chest. 111 (3): 537–43. PMID 9118684. Retrieved 2011-12-05. Unknown parameter
|month=ignored (help) - ↑ McGinn S, White PD. Acute cor pulmonale resulting from pulmonary embolism. J Am Med Assoc 1935;104:1473–1480.
- ↑ Panos RJ, Barish RA, Whye DW, Groleau G (1988). "The electrocardiographic manifestations of pulmonary embolism". J Emerg Med. 6 (4): 301–7. PMID 3225435.
- ↑ Abecasis J, Monge J, Alberca D, Grenho MF, Arroja I, Aleixo AM (2008). "Electrocardiographic presentation of massive and submassive pulmonary embolism". Rev Port Cardiol. 27 (5): 591–610. PMID 18717213.
- ↑ Raghav KP, Makkuni P, Figueredo VM (2011). "A review of electrocardiography in pulmonary embolism: recognizing pulmonary embolus masquerading as ST-elevation myocardial infarction". Rev Cardiovasc Med. 12 (3): 157–63. PMID 22145193.
|access-date=requires|url=(help) - ↑ Kucher N, Walpoth N, Wustmann K, Noveanu M, Gertsch M (2003). "QR in V1--an ECG sign associated with right ventricular strain and adverse clinical outcome in pulmonary embolism". European Heart Journal. 24 (12): 1113–9. PMID 12804925. Retrieved 2011-12-05. Unknown parameter
|month=ignored (help)