Pamidronic acid: Difference between revisions
Brian Blank (talk | contribs) No edit summary |
No edit summary |
||
| (9 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
{{ | {{DrugProjectFormSinglePage | ||
| | |authorTag={{VP}}<!--Overview--> | ||
| | |aOrAn=a | ||
| | |drugClass=[[bisphosphonate]] | ||
| | |indicationType=treatment | ||
| | |indication=[[hypercalcemia]] of [[malignancy]], [[Paget's disease]], osteolytic [[bone metastases]] of [[breast cancer]] and osteolytic lesions of [[multiple myeloma]] | ||
| | |adverseReactions=[[hypertension]], injection site reactiion, [[hypocalcemia]], [[hypokalemia]], [[hypomagnesemia]], [[hypophosphatemia]], [[loss of appetite]], [[nausea]], [[vomiting]], [[anemia]], urinary tract infectious disease, [[cough]], [[dyspnea]], [[fatigue]], and [[malaise]] | ||
| | |||
| | <!--Black Box Warning--> | ||
| | |blackBoxWarningTitle=Title | ||
| | |blackBoxWarningBody=<i><span style="color:#FF0000;">ConditionName: </span></i> | ||
| | |||
| | * Content | ||
| | |||
<!--Adult Indications and Dosage--> | |||
<!--FDA-Labeled Indications and Dosage (Adult)--> | |||
|fdaLIADAdult======Hypercalcemia of Malignancy===== | |||
*Pamidronate disodium, in conjunction with adequate hydration, is indicated for the treatment of moderate or severe [[hypercalcemia]] associated with malignancy, with or without bone [[metastases]]. Patients who have either epidermoid or non-epidermoid tumors respond to treatment with pamidronate disodium. Vigorous saline hydration, an integral part of hypercalcemia therapy, should be initiated promptly and an attempt should be made to restore the urine output to about 2 L/day throughout treatment. Mild or asymptomatic [[hypercalcemia]] may be treated with conservative measures (i.e., saline hydration, with or without [[loop diuretics]]). Patients should be hydrated adequately throughout the treatment, but overhydration, especially in those patients who have cardiac failure, must be avoided. Diuretic therapy should not be employed prior to correction of [[hypovolemia]]. The safety and efficacy of pamidronate disodium in the treatment of [[hypercalcemia]] associated with [[hyperparathyroidism]] or with other non-tumor-related conditions has not been established. | |||
*Moderate Hypercalcemia | |||
:*The recommended dose of pamidronate disodium in moderate [[hypercalcemia]] (corrected serum calcium* of approximately 12 to 13.5 mg/dL) is 60 to 90 mg given as a SINGLE-DOSE, intravenous infusion over 2 to 24 hours. Longer infusions (i.e., >2 hours) may reduce the risk of renal toxicity, particularly in patients with preexisting [[renal insufficiency]]. | |||
*Severe Hypercalcemia | |||
:*The recommended dose of pamidronate disodium in severe [[hypercalcemia]] (corrected serum calcium* >13.5 mg/dL) is 90 mg given as a SINGLE-DOSE, intravenous infusion over 2 to 24 hours. Longer infusions (i.e., >2 hours) may reduce the risk of renal toxicity, particularly in patients with preexisting [[renal insufficiency]]. | |||
:*Albumin-corrected serum calcium (CCa, mg/dL) = serum calcium, mg/dL + 0.8 (4.0-serum albumin, g/dL). | |||
*Retreatment | |||
:*A limited number of patients have received more than one treatment with pamidronate disodium for [[hypercalcemia]]. Retreatment with pamidronate disodium, in patients who show complete or partial response initially, may be carried out if serum calcium does not return to normal or remain normal after initial treatment. It is recommended that a minimum of 7 days elapse before retreatment, to allow for full response to the initial dose. The dose and manner of retreatment is identical to that of the initial therapy. | |||
=====Paget’s Disease===== | |||
*Pamidronate disodium is indicated for the treatment of patients with moderate to severe Paget’s disease of bone. The effectiveness of pamidronate disodium was demonstrated primarily in patients with serum [[alkaline phosphatase]] ≥3 times the upper limit of normal. Pamidronate disodium therapy in patients with Paget’s disease has been effective in reducing serum alkaline phosphatase and urinary hydroxyproline levels by ≥50% in at least 50% of patients, and by ≥30% in at least 80% of patients. Pamidronate disodium therapy has also been effective in reducing these biochemical markers in patients with [[Paget’s disease]] who failed to respond, or no longer responded to other treatments. | |||
*The recommended dose of pamidronate disodium in patients with moderate to severe [[Paget’s disease of bone]] is 30 mg daily, administered as a 4 hour infusion on 3 consecutive days for a total dose of 90 mg. | |||
*Retreatment | |||
:*A limited number of patients with Paget’s disease have received more than one treatment of pamidronate disodium in clinical trials. When clinically indicated, patients should be retreated at the dose of initial therapy. | |||
=====Osteolytic Bone Metastases of Breast Cancer and Osteolytic Lesions of Multiple Myeloma===== | |||
*Pamidronate disodium is indicated, in conjunction with standard antineoplastic therapy, for the treatment of osteolytic bone metastases of [[breast cancer]] and osteolytic lesions of [[multiple myeloma]]. The pamidronate disodium treatment effect appeared to be smaller in the study of breast cancer patients receiving hormonal therapy than in the study of those receiving chemotherapy, however, overall evidence of clinical benefit has been demonstrated. | |||
*Osteolytic Bone Lesions of Multiple Myeloma | |||
:*The recommended dose of pamidronate disodium in patients with osteolytic bone lesions of multiple myeloma is 90 mg administered as a 4 hour infusion given on a monthly basis. | |||
:*Patients with marked Bence-Jones proteinuria and dehydration should receive adequate hydration prior to pamidronate disodium infusion. | |||
:*Limited information is available on the use of pamidronate disodium in multiple myeloma patients with a serum creatinine ≥3.0 mg/dL. | |||
:*Patients who receive pamidronate disodium should have serum [[creatinine]] assessed prior to each treatment. Treatment should be withheld for renal deterioration. In a clinical study, renal deterioration was defined as follows: | |||
:**For patients with normal baseline creatinine, increase of 0.5 mg/dL. | |||
:**For patients with abnormal baseline creatinine, increase of 1.0 mg/dL. | |||
:*In this clinical study, pamidronate disodium treatment was resumed only when the creatinine returned to within 10% of the baseline value. | |||
:*The optimal duration of therapy is not yet known, however, in a study of patients with myeloma, final analysis after 21 months demonstrated overall benefits (see Clinical Trials section). | |||
*Osteolytic Bone Metastases of Breast Cancer | |||
:*The recommended dose of pamidronate disodium in patients with osteolytic bone metastases is 90 mg administered over a 2 hour infusion given every 3 to 4 weeks. | |||
:*Pamidronate disodium has been frequently used with [[doxorubicin]], [[fluorouracil]], [[cyclophosphamide]], [[methotrexate]], [[mitoxantrone]], [[vinblastine]], [[dexamethasone]], [[prednisone]], [[melphalan]], [[vincristine]], [[megesterol]], and [[tamoxifen]]. It has been given less frequently with [[etoposide]], [[cisplatin]], [[cytarabine]], [[paclitaxel]], and aminoglutethimide. | |||
:*Patients who receive pamidronate disodium should have serum creatinine assessed prior to each treatment. Treatment should be withheld for renal deterioration. In a clinical study, renal deterioration was defined as follows: | |||
:**For patients with normal baseline creatinine, increase of 0.5 mg/dL. | |||
:**For patients with abnormal baseline creatinine, increase of 1.0 mg/dL. | |||
:*In this clinical study, pamidronate disodium treatment was resumed only when the creatinine returned to within 10% of the baseline value. | |||
:*The optimal duration of therapy is not known, however, in two breast cancer studies, final analyses performed after 24 months of therapy demonstrated overall benefit. | |||
<!--Off-Label Use and Dosage (Adult)--> | |||
<!--Guideline-Supported Use (Adult)--> | |||
|offLabelAdultGuideSupport=There is limited information regarding <i>Off-Label Guideline-Supported Use</i> of {{PAGENAME}} in adult patients. | |||
<!--Non–Guideline-Supported Use (Adult)--> | |||
|offLabelAdultNoGuideSupport======Complex regional pain syndrome, type I===== | |||
*IV pamidronate 60 mg administered once daily over an interval of 3 consecutive days.<ref name="pmid11752511">{{cite journal| author=Kubalek I, Fain O, Paries J, Kettaneh A, Thomas M| title=Treatment of reflex sympathetic dystrophy with pamidronate: 29 cases. | journal=Rheumatology (Oxford) | year= 2001 | volume= 40 | issue= 12 | pages= 1394-7 | pmid=11752511 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11752511 }} </ref> | |||
=====Disorder of joint of spine===== | |||
*6 months a monthly IV infusion of pamidronate 60 mg.<ref name="pmid11920413">{{cite journal| author=Maksymowych WP, Jhangri GS, Fitzgerald AA, LeClercq S, Chiu P, Yan A et al.| title=A six-month randomized, controlled, double-blind, dose-response comparison of intravenous pamidronate (60 mg versus 10 mg) in the treatment of nonsteroidal antiinflammatory drug-refractory ankylosing spondylitis. | journal=Arthritis Rheum | year= 2002 | volume= 46 | issue= 3 | pages= 766-73 | pmid=11920413 | doi=10.1002/art.10139 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11920413 }} </ref> | |||
=====Drug-induced osteoporosis; Prophylaxis - Gonad regulating hormone adverse reaction===== | |||
*IV pamidronate 60 mg.<ref name="pmid11575286">{{cite journal| author=Smith MR, McGovern FJ, Zietman AL, Fallon MA, Hayden DL, Schoenfeld DA et al.| title=Pamidronate to prevent bone loss during androgen-deprivation therapy for prostate cancer. | journal=N Engl J Med | year= 2001 | volume= 345 | issue= 13 | pages= 948-55 | pmid=11575286 | doi=10.1056/NEJMoa010845 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11575286 }} </ref> | |||
=====Hypercalcemia, Associated with tamoxifen-induced tumor flare===== | |||
*Single IV infusion of pamidronate, at doses ranging from 30 to 90 mg. (determined by severity of hypercalcemia).<ref name="pmid11244326">{{cite journal| author=Nikolic-Tomasević Z, Jelic S, Popov I, Radosavljević D, Mitrović L| title=Tumor 'flare' hypercalcemia--an additional indication for bisphosphonates? | journal=Oncology | year= 2001 | volume= 60 | issue= 2 | pages= 123-6 | pmid=11244326 | doi=55308 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11244326 }} </ref> | |||
=====Osteopenia (Acute); Prophylaxis - Total replacement of hip===== | |||
*Single postoperative IV infusion of pamidronate 90 mg.<ref name="pmid11277274">{{cite journal| author=Wilkinson JM, Stockley I, Peel NF, Hamer AJ, Elson RA, Barrington NA et al.| title=Effect of pamidronate in preventing local bone loss after total hip arthroplasty: a randomized, double-blind, controlled trial. | journal=J Bone Miner Res | year= 2001 | volume= 16 | issue= 3 | pages= 556-64 | pmid=11277274 | doi=10.1359/jbmr.2001.16.3.556 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11277274 }} </ref> | |||
=====Osteoporosis due to corticosteroids===== | |||
*Oral pamidronate for 12 months.<ref name="pmid2892989">{{cite journal| author=Reid IR, King AR, Alexander CJ, Ibbertson HK| title=Prevention of steroid-induced osteoporosis with (3-amino-1-hydroxypropylidene)-1,1-bisphosphonate (APD). | journal=Lancet | year= 1988 | volume= 1 | issue= 8578 | pages= 143-6 | pmid=2892989 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=2892989 }} </ref> | |||
=====Postmenopausal osteoporosis===== | |||
*300 mg pamidronate orally once daily for 4 weeks every 16 weeks.<ref name="pmid10793877">{{cite journal| author=Ryan PJ, Blake GM, Davie M, Haddaway M, Gibson T, Fogelman I| title=Intermittent oral disodium pamidronate in established osteoporosis: a 2 year double-masked placebo-controlled study of efficacy and safety. | journal=Osteoporos Int | year= 2000 | volume= 11 | issue= 2 | pages= 171-6 | pmid=10793877 | doi=10.1007/PL00004179 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=10793877 }} </ref> | |||
<!--Pediatric Indications and Dosage--> | |||
<!--FDA-Labeled Indications and Dosage (Pediatric)--> | |||
|fdaLIADPed=There is limited information regarding <i>FDA-Labeled Use</i> of {{PAGENAME}} in pediatric patients. | |||
<!--Off-Label Use and Dosage (Pediatric)--> | |||
<!--Guideline-Supported Use (Pediatric)--> | |||
|offLabelPedGuideSupport=There is limited information regarding <i>Off-Label Guideline-Supported Use</i> of {{PAGENAME}} in pediatric patients. | |||
<!--Non–Guideline-Supported Use (Pediatric)--> | |||
|offLabelPedNoGuideSupport======Osteogenesis imperfecta===== | |||
*Pamidronate by slow IV infusion over 3 hours for 3 consecutive days.<ref name="pmid19039235">{{cite journal| author=Alharbi M, Pinto G, Finidori G, Souberbielle JC, Guillou F, Gaubicher S et al.| title=Pamidronate treatment of children with moderate-to-severe osteogenesis imperfecta: a note of caution. | journal=Horm Res | year= 2009 | volume= 71 | issue= 1 | pages= 38-44 | pmid=19039235 | doi=10.1159/000173740 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=19039235 }} </ref> | |||
=====Osteopenia - Tetraplegic cerebral palsy===== | |||
*IV pamidronate dosed at 1 mg/kg (total daily dose not less than 15 mg or greater than 30 mg) and given daily for 3 consecutive days every 3 months for 1 year.<ref name="pmid12410192">{{cite journal| author=Henderson RC, Lark RK, Kecskemethy HH, Miller F, Harcke HT, Bachrach SJ| title=Bisphosphonates to treat osteopenia in children with quadriplegic cerebral palsy: a randomized, placebo-controlled clinical trial. | journal=J Pediatr | year= 2002 | volume= 141 | issue= 5 | pages= 644-51 | pmid=12410192 | doi=10.1067/mpd.2002.128207 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=12410192 }} </ref> | |||
<!--Contraindications--> | |||
|contraindications=* Pamidronate disodium is contraindicated in patients with clinically significant [[hypersensitivity]] to pamidronate disodium or other bisphosphonates. | |||
<!--Warnings--> | |||
|warnings=* Deterioration in Renal Function | |||
:*Bisphosphonates, including pamidronate disodium, have been associated with renal toxicity manifested as deterioration of renal function and potential renal failure. | |||
:*Due to the risk of clinically significant deterioration in renal function, which may progress to renal failure, single doses of pamidronate disodium should not exceed 90 mg. Renal deterioration, progression to [[renal failure]], and [[dialysis]] have been reported in patients after the initial or a single dose of pamidronate disodium. | |||
:*[[Focal segmental glomerulosclerosis]] (including the collapsing variant) with or without nephrotic syndrome, which may lead to renal failure, has been reported in pamidronate disodium–treated patients, particularly in the setting of [[multiple myeloma]] and [[breast cancer]]. Some of these patients had gradual improvement in renal status after pamidronate disodium was discontinued. | |||
:*Patients who receive pamidronate disodium should have serum [[creatinine]] assessed prior to each treatment. Patients treated with pamidronate disodium for bone metastases should have the dose withheld if renal function has deteriorated. | |||
*PREGNANCY: pamidronate disodium should not be used during pregnancy | |||
:*Pamidronate disodium may cause fetal harm when administered to a pregnant woman. | |||
:*There are no studies in pregnant women using pamidronate disodium. If the patient becomes pregnant while taking this drug, the patient should be apprised of the potential harm to the fetus. Women of childbearing potential should be advised to avoid becoming pregnant. | |||
:*Studies conducted in young rats have reported the disruption of dental dentine formation following single- and multi-dose administration of [[bisphosphonates]]. The clinical significance of these findings is unknown. | |||
====Precautions==== | |||
* General | |||
:*Standard [[hypercalcemia]]-related metabolic parameters, such as serum levels of calcium, phosphate, magnesium, and potassium, should be carefully monitored following initiation of therapy with pamidronate disodium. Cases of asymptomatic [[hypophosphatemia]] (12%), [[hypokalemia]] (7%), [[hypomagnesemia]] (11%), and [[hypocalcemia]] (5% to 12%), were reported in pamidronate disodium-treated patients. Rare cases of symptomatic hypocalcemia (including tetany) have been reported in association with pamidronate therapy. If [[hypocalcemia]] occurs, short-term calcium therapy may be necessary. In [[Paget’s disease of bone]], 17% of patients treated with 90 mg of pamidronate disodium showed serum calcium levels below 8 mg/dL. | |||
:*Patients with a history of thyroid surgery may have relative [[hypoparathyroidism]] that may predispose to [[hypocalcemia]] with pamidronate disodium. | |||
*Renal Insufficiency | |||
:*Pamidronate disodium is excreted intact primarily via the kidney, and the risk of renal adverse reactions may be greater in patients with impaired renal function. Patients who receive pamidronate disodium should have serum creatinine assessed prior to each treatment. In patients receiving pamidronate disodium for bone metastases, who show evidence of deterioration in renal function, pamidronate disodium treatment should be withheld until renal function returns to baseline. | |||
:*In clinical trials, patients with renal impairment (serum creatinine >3.0 mg/dL) have not been studied. Limited pharmacokinetic data exist in patients with creatinine clearance <;<30 mL/min. For the treatment of bone metastases, the use of pamidronate disodium in patients with severe [[renal impairment]] is not recommended. In other indications, clinical judgement should determine whether the potential benefit outweighs the potential risk in such patients. | |||
*Osteonecrosis of the Jaw | |||
:*[[Osteonecrosis of the jaw]] (ONJ) has been reported predominantly in cancer patients treated with intravenous [[biphosphonates]], including pamidronate disodium. Many of these patients were also receiving [[chemotherapy]] and [[corticosteroids]] which may be risk factors for ONJ. Postmarketing experience and the literature suggest a greater frequency of reports of ONJ based on tumor type (advanced [[breast cancer]], [[multiple myeloma]]), and dental status (dental extraction, periodontal disease, local trauma including poorly fitting dentures). Many reports of ONJ involved patients with signs of local infection including [[osteomyelitis]]. | |||
:*Cancer patients should maintain good oral hygiene and should have a dental examination with preventive dentistry prior to treatment with bisphophonates. | |||
:*While on treatment, these patients should avoid invasive dental procedures if possible. For patients who develop ONJ while on bisphosphonate therapy, dental surgey may exacerbate the condition. For patients requiring dental procedures, there are no data available to suggest whether discontinuation of bisphosphonate treatment reduces the risk of ONJ. Clinical judgement of the treating physician should guide the management plan of each patient based on individual benefit/risk assessment. | |||
*Musculoskeletal Pain | |||
:*In post-marketing experience, severe and occasionally incapacitating bone, joint, and/or muscle pain has been reported in patients taking biphosphonates. However, such reports have been infrequent. This category of drugs includes pamidronate disodium injection. The time to onset of symptoms varied from one day to several months after starting the drug. Most patients had relief of symptoms after stopping. A subset had recurrence of symptoms when rechallanged with the same drug or another biphosphonate. | |||
*Laboratory Tests | |||
:*Patients who receive pamidronate disodium should have serum [[creatinine]] assessed prior to each treatment. Serum calcium, electrolytes, phosphate, magnesium, and CBC, differential, and [[hematocrit]]/[[hemoglobin]] must be closely monitored in patients treated with pamidronate disodium. Patients who have preexisting [[anemia]], [[leukopenia]], or [[thrombocytopenia]] should be monitored carefully in the first 2 weeks following treatment. | |||
<!--Adverse Reactions--> | |||
<!--Clinical Trials Experience--> | |||
|clinicalTrials======Hypercalcemia of Malignancy===== | |||
*Transient mild elevation of temperature by at least 1°C was noted 24 to 48 hours after administration of pamidronate disodium in 34% of patients in clinical trials. In the saline trial, 18% of patients had a temperature elevation of at least 1°C 24 to 48 hours after treatment. | |||
*Drug-related local soft-tissue symptoms (redness, swelling or induration and pain on palpation) at the site of catheter insertion were most common in patients treated with 90 mg of pamidronate disodium. Symptomatic treatment resulted in rapid resolution in all patients. | |||
*Rare cases of [[uveitis]], [[iritis]], [[scleritis]], and [[episcleritis]] have been reported, including one case of [[scleritis]], and one case of uveitis upon separate rechallenges. | |||
*Five of 231 patients (2%) who received pamidronate disodium during the four U.S. controlled hypercalcemia clinical studies were reported to have had seizures, 2 of whom had preexisting seizure disorders. None of the [[seizures]] were considered to be drug-related by the investigators. However, a possible relationship between the drug and the occurrence of seizures cannot be ruled out. It should be noted that in the saline arm 1 patient (4%) had a [[seizure]]. | |||
*There are no controlled clinical trials comparing the efficacy and safety of 90 mg pamidronate disodium over 24 hours to 2 hours in patients with [[hypercalcemia]] of [[malignancy]]. However, a comparison of data from separate clinical trials suggests that the overall safety profile in patients who received 90 mg pamidronate disodium over 24 hours is similar to those who received 90 mg pamidronate disodium over 2 hours. The only notable differences observed were an increase in the proportion of patients in the pamidronate 24 hour group who experienced fluid overload and electrolyte/mineral abnormalities. | |||
*At least 15% of patients treated with pamidronate disodium for hypercalcemia of malignancy also experienced the following adverse events during a clinical trial: | |||
=====General===== | |||
Fluid overload, generalized pain | |||
=====Cardiovascular===== | |||
[[Hypertension]] | |||
=====Gastrointestinal===== | |||
[[Abdominal pain]], [[anorexia]], [[constipation]], [[nausea]], [[vomiting]] | |||
=====Genitourinary===== | |||
[[Urinary tract infection]] | |||
=====Musculoskeletal===== | |||
[[Bone pain]] | |||
=====Laboratory abnormality===== | |||
[[Anemia]], [[hypokalemia]], [[hypomagnesemia]], [[hypophosphatemia]] | |||
*Many of these adverse experiences may have been related to the underlying disease state. The following table lists the adverse experiences considered to be treatment-related during comparative, controlled U.S. trials. | |||
: [[File:{{PAGENAME}}06.png|thumb|none|600px|This image is provided by the National Library of Medicine.]] | |||
=====Paget’s Disease===== | |||
*Transient mild elevation of temperature >1°C above pretreatment baseline was noted within 48 hours after completion of treatment in 21% of the patients treated with 90 mg of pamidronate disodium in clinical trials. | |||
*Drug-related musculoskeletal pain and nervous system symptoms ([[dizziness]], [[headache]], [[paresthesia]], increased sweating) were more common in patients with Paget’s disease treated with 90 mg of pamidronate disodium than in patients with hypercalcemia of malignancy treated with the same dose. | |||
*Adverse experiences considered to be related to trial drug, which occurred in at least 5% of patients with Paget’s disease treated with 90 mg of pamidronate disodium in two U.S. clinical trials, were [[fever]], [[nausea]], [[back pain]], and [[bone pain]]. | |||
*At least 10% of all pamidronate disodium-treated patients with Paget’s disease also experienced the following adverse experiences during clinical trials: | |||
=====Cardiovascular===== | |||
[[Hypertension]] | |||
=====Musculoskeletal===== | |||
[[Arthrosis]], [[bone pain]] | |||
=====Nervous system===== | |||
[[Headache]] | |||
*Most of these adverse experiences may have been related to the underlying disease state. | |||
=====Osteolytic Bone Metastases of Breaset Cancer and Osteolytic Lesions of Multiple Myeloma===== | |||
*The most commonly reported (>15%) adverse experiences occurred with similar frequencies in the pamidronate disodium and placebo treatment groups, and most of these adverse experiences may have been related to the underlying disease state or cancer therapy. | |||
: [[File:{{PAGENAME}}07.png|thumb|none|600px|This image is provided by the National Library of Medicine.]] | |||
*Of the toxicities commonly associated with chemotherapy, the frequency of vomiting, anorexia, and anemia were slightly more common in the pamidronate disodium patients whereas stomatitis and alopecia occurred at a frequency similar to that in placebo patients. In the breast cancer trials, mild elevations of serum creatinine occurred in 18.5% of pamidronate disodium patients and 12.3% of placebo patients. Mineral and electrolyte disturbances, including hypocalcemia, were reported rarely and in similar percentages of pamidronate disodium-treated patients compared with those in the placebo group. The reported frequencies of [[hypocalcemia]], [[hypokalemia]], [[hypophophatemia]], and [[hypomagnesemia]] for pamidronate disodium-treated patients were 3.3%, 10.5%, 1.7%, and 4.4%, respectively, and for placebo-treated patients were 1.2%, 12%, 1.7%, and 4.5%, respectively. In previous hypercalcemia of malignancy trials, patients treated with pamidronate disodium (60 or 90 mg over 24 hours) developed electrolyte abnormalities more frequently. | |||
*Arthralgias and myalgias were reported slightly more frequently in the pamidronate disodium group than in the placebo group (13.6% and 26% vs 10.8% and 20.1%, respectively). | |||
*In multiple myeloma patients, there were five pamidronate disodium-related serious and unexpected adverse experiences. Four of these were reported during the 12 month extension of the [[multiple myeloma]] trial. Three of the reports were of worsening renal function developing in patients with progressive multiple myeloma or multiple myeloma-associated amyloidosis. The fourth report was the adult [[respiratory distress syndrome]] developing in a patient recovering from [[pneumonia]] and acute gangrenous cholecystitis. One pamidronate disodium-treated patient experienced an allergic reaction characterized by swollen and itchy eyes, runny nose, and scratchy throat within 24 hours after the sixth infusion. | |||
*In the [[breast cancer]] trials, there were four pamidronate disodium-related adverse experiences, all moderate in severity, that caused a patient to discontinue participation in the trial. One was due to [[interstitial pneumonitis]], another to malaise and dyspnea. One pamidronate disodium patient discontinued the trial due to a symptomatic hypocalcemia. Another pamidronate disodium patient discontinued therapy due to severe bone pain after each infusion, which the investigator felt was trial-drug-related. | |||
=====Renal Toxicity===== | |||
*In a study of the safety and efficacy of pamidronate disodium 90 mg (2 hour infusion) versus Zometa® 4 mg (15 minute infusion) in bone metastases patients with multiple myeloma or breast cancer, renal deterioration was defined as an increase in serum creatinine of 0.5 mg/dL for patients with normal baseline creatinine (<1.4 mg/dL) or an increase of 1.0 mg/dL for patients with an abnormal baseline creatinine (≥1.4 mg/dL). The following are data on the incidence of renal deterioration in patients in this trial. See table below. | |||
: [[File:{{PAGENAME}}08.png|thumb|none|600px|This image is provided by the National Library of Medicine.]] | |||
<!--Postmarketing Experience--> | |||
|postmarketing=*The following adverse reactions have been reported in post-marketing use: General : reactivation of [[Herpes simplex]] and [[Herpes zoster]], [[influenza]]-like symptoms; CNS : confusion and visual hallucinations, sometimes in the presence of electrolyte imbalance; Skin : [[rash]], [[pruritus]]; Special senses : [[conjunctivitis]]; Renal : [[focal segmental glomerulosclerosis]] including the collapsing variant, [[nephrotic syndrome]]; Laboratory abnormalities : [[hyperkalemia]], [[hypernatremia]], [[hematuria]]. Rare instances of allergic manifestations have been reported, including [[hypotension]], [[dyspnea]], or [[angioedema]], and very rarely, anaphylactic shock. Pamidronate disodium is contraindicated in patients with clinically significant [[hypersensitivity]] to pamidronate disodium or other bisphosphonates. | |||
*Cases of [[osteonecrosis]] (primarily involving the jaw) have been reported predominantly in cancer patients treated with intravenous [[bisphosphonates]], including pamidronate disodium. Many of these patients were also receiving chemotherapy and [[corticosteroids]] which may be risk factors for ONJ. Data suggest a greater frequency of reports of ONJ in certain cancers, such as advanced [[breast cancer]] and [[multiple myeloma]]. The majority of the reported cases are in cancer patients following invasive dental procedures, such as tooth extraction. It is therefore prudent to avoid invasive dental procrdures as recovery may be prolonged. | |||
<!--Drug Interactions--> | |||
|drugInteractions=*Concomitant administration of a [[loop diuretic]] had no effect on the calcium-lowering action of pamidronate disodium. | |||
*Caution is indicated when pamidronate disodium is used with other potentially nephrotoxic drugs. | |||
*In [[multiple myeloma]] patients, the risk of renal dysfunction may be increased when pamidronate disodium is used in combination with thalidomide. | |||
<!--Use in Specific Populations--> | |||
|useInPregnancyFDA=* '''Pregnancy Category D''' | |||
*There are no adequate and well-controlled studies in pregnant women. | |||
*Bolus intravenous studies conducted in rats and rabbits determined that pamidronate disodium produces maternal toxicity and embryo/fetal effects when given during organogenesis at doses of 0.6 to 8.3 times the highest recommended human dose for a single intravenous infusion. As it has been shown that pamidronate disodium can cross the placenta in rats and has produced marked maternal and nonteratogenic embryo/fetal effects in rats and rabbits, it should not be given to women during pregnancy. | |||
*Bisphosphonates are incorporated into the bone matrix, from where they are gradually released over periods of weeks to years. The extent of bisphosphonate incorporation into adult bone, and hence, the amount available for release back into the systematic circulation, is directly related to the total dose and duration of bisphosphonate use. Although there are no data on fetal risk in humans, bisphosphonates do cause fetal harm in animals, and animal data suggest that uptake of bisphosphonates into fetal bone is greater than into maternal bone. Therefore, there is a theoretical risk of fetal harm (e.g., skeletal and other abnormalities) if a woman becomes pregnant after completing a course of bisphosphonate therapy. The impact of variables such as time between cessation of bisphosphonate therapy to conception, the particular bisphosphonate used, and the route of administration (intravenous versus oral) on this risk has not been established. | |||
|useInPregnancyAUS=* '''Australian Drug Evaluation Committee (ADEC) Pregnancy Category''' | |||
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of {{PAGENAME}} in women who are pregnant. | |||
|useInLaborDelivery=There is no FDA guidance on use of {{PAGENAME}} during labor and delivery. | |||
|useInNursing=*It is not known whether pamidronate disodium is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when pamidronate disodium is administered to a nursing woman. | |||
|useInPed=*Safety and effectiveness of pamidronate disodium in pediatric patients have not been established. | |||
|useInGeri=*Of the total number of subjects in clinical studies of pamidronate disodium, approximately 20% were 65 and over, while approximately 15% were 75 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy. | |||
|useInGender=There is no FDA guidance on the use of {{PAGENAME}} with respect to specific gender populations. | |||
|useInRace=There is no FDA guidance on the use of {{PAGENAME}} with respect to specific racial populations. | |||
|useInRenalImpair=There is no FDA guidance on the use of {{PAGENAME}} in patients with renal impairment. | |||
|useInHepaticImpair=There is no FDA guidance on the use of {{PAGENAME}} in patients with hepatic impairment. | |||
|useInReproPotential=There is no FDA guidance on the use of {{PAGENAME}} in women of reproductive potentials and males. | |||
|useInImmunocomp=There is no FDA guidance one the use of {{PAGENAME}} in patients who are immunocompromised. | |||
<!--Administration and Monitoring--> | |||
|administration=* Intravenous | |||
|monitoring=There is limited information regarding <i>Monitoring</i> of {{PAGENAME}} in the drug label. | |||
<!--IV Compatibility--> | |||
|IVCompat=There is limited information regarding <i>IV Compatibility</i> of {{PAGENAME}} in the drug label. | |||
<!--Overdosage--> | |||
|overdose====Acute Overdose=== | |||
*There have been several cases of drug maladministration of intravenous pamidronate disodium in [[hypercalcemia]] patients with total doses of 225 mg to 300 mg given over 21/2 to 4 days. All of these patients survived, but they experienced [[hypocalcemia]] that required intravenous and/or oral administration of calcium. Single doses of pamidronate disodium should not exceed 90 mg and the duration of the intravenous infusion should be no less than 2 hours. | |||
*In addition, one obese woman (95 kg) who was treated with 285 mg of pamidronate disodium/day for 3 days experienced high [[fever]] (39.5°C), [[hypotension]] (from 170/90 mmHg to 90/60 mmHg), and transient taste perversion, noted about 6 hours after the first infusion. The [[fever]] and [[hypotension]] were rapidly corrected with [[steroids]]. | |||
*If overdosage occurs, symptomatic [[hypocalcemia]] could also result; such patients should be treated with short-term intravenous calcium. | |||
===Chronic Overdose=== | |||
There is limited information regarding <i>Chronic Overdose</i> of {{PAGENAME}} in the drug label. | |||
<!--Pharmacology--> | |||
<!--Drug box 2--> | |||
|drugBox={{Drugbox2 | |||
| verifiedrevid = 476996826 | |||
| IUPAC_name = (3-amino-1-hydroxypropane-1,1-diyl)bis(phosphonic acid) | |||
| image = Pamidronic acid00.png | |||
<!--Clinical data--> | |||
| tradename = | |||
| Drugs.com = {{drugs.com|international|pamidronic-acid}} | |||
| MedlinePlus = a601163 | |||
| pregnancy_AU = B3 | | pregnancy_AU = B3 | ||
| pregnancy_US = D | | pregnancy_US = D | ||
| Line 19: | Line 313: | ||
| legal_US = Rx-only | | legal_US = Rx-only | ||
| routes_of_administration = [[Intravenous therapy|Intravenous]] | | routes_of_administration = [[Intravenous therapy|Intravenous]] | ||
<!--Pharmacokinetic data--> | |||
| bioavailability = n/a | |||
| protein_bound = 54% | |||
| metabolism = Nil | |||
| elimination_half-life = 28 ± 7 hours | |||
| excretion = [[Kidney|Renal]] | |||
<!--Identifiers--> | |||
| CASNo_Ref = {{cascite|correct|CAS}} | |||
| CAS_number_Ref = {{cascite|correct|??}} | |||
| CAS_number = 40391-99-9 | |||
| ATC_prefix = M05 | |||
| ATC_suffix = BA03 | |||
| PubChem = 4674 | |||
| DrugBank_Ref = {{drugbankcite|correct|drugbank}} | |||
| DrugBank = DB00282 | |||
| ChemSpiderID_Ref = {{chemspidercite|correct|chemspider}} | |||
| ChemSpiderID = 4512 | |||
| UNII_Ref = {{fdacite|correct|FDA}} | |||
| UNII = OYY3447OMC | |||
| KEGG_Ref = {{keggcite|correct|kegg}} | |||
| KEGG = D07281 | |||
| ChEMBL_Ref = {{ebicite|correct|EBI}} | |||
| ChEMBL = 834 | |||
<!--Chemical data--> | |||
| C=3 | H=11 | N=1 | O=7 | P=2 | |||
| molecular_weight = 235.07 g/mol | |||
| smiles = O=P(O)(O)C(O)(CCN)P(=O)(O)O | |||
| InChI = 1/C3H11NO7P2/c4-2-1-3(5,12(6,7)8)13(9,10)11/h5H,1-2,4H2,(H2,6,7,8)(H2,9,10,11) | |||
| InChIKey = WRUUGTRCQOWXEG-UHFFFAOYAH | |||
| StdInChI_Ref = {{stdinchicite|correct|chemspider}} | |||
| StdInChI = 1S/C3H11NO7P2/c4-2-1-3(5,12(6,7)8)13(9,10)11/h5H,1-2,4H2,(H2,6,7,8)(H2,9,10,11) | |||
| StdInChIKey_Ref = {{stdinchicite|correct|chemspider}} | |||
| StdInChIKey = WRUUGTRCQOWXEG-UHFFFAOYSA-N | |||
}} | |||
<!--Mechanism of Action--> | |||
|mechAction=* The principal pharmacologic action of pamidronate disodium is inhibition of bone resorption. Although the mechanism of antiresorptive action is not completely understood, several factors are thought to contribute to this action. Pamidronate disodium adsorbs to calcium phosphate (hydroxyapatite) crystals in bone and may directly block dissolution of this mineral component of bone. In vitro studies also suggest that inhibition of osteoclast activity contributes to inhibition of bone resorption. In animal studies, at doses recommended for the treatment of [[hypercalcemia]], pamidronate disodium inhibits bone resorption apparently without inhibiting bone formation and mineralization. Of relevance to the treatment of [[hypercalcemia]] of malignancy is the finding that pamidronate disodium inhibits the accelerated bone resorption that results from osteoclast hyperactivity induced by various tumors in animal studies. | |||
<!--Structure--> | |||
|structure=* Pamidronate Disodium is a sterile bone-resorption inhibitor available in 30 mg and 90 mg vials for intravenous administration. The pamidronate disodium obtained by combining pamidronic acid and sodium hydroxide is provided in a sterile, ready to use solution for injection. Each mL of the 30 mg vial contains, 3 mg Pamidronate Disodium, 47 mg Mannitol, USP; Water for Injection, USP, q.s.; Phosphoric acid to adjust pH. Each mL of the 90 mg vial contains, 9 mg Pamidronate Disodium, 37.5 mg Mannitol, USP; Water for Injection, USP, q.s.; Phosphoric acid to adjust pH. The pH of a 1% solution of pamidronate disodium in distilled water is approximately 8.3. Pamidronate, a member of the group of chemical compounds known as bisphosphonates, is an analog of pyrophosphate. Pamidronate disodium is designated chemically as phosphonic acid (3-amino-1-hydroxypropylidene) bis-, disodium salt, and its structural formula is: | |||
: [[File:{{PAGENAME}}12.png|thumb|none|600px|This image is provided by the National Library of Medicine.]] | |||
*Pamidronate disodium is soluble in water and in 2N sodium hydroxide, sparingly soluble in 0.1N hydrochloric acid and in 0.1N acetic acid, and practically insoluble in organic solvents. Its molecular formula is C3H9NO7P2Na2 and its molecular weight is 279.1 (calculated as the anhydrous form). | |||
*Inactive Ingredients: Mannitol, Phosphoric acid (for adjustment to pH range of 6.0 to 7.0) and Water for Injection. | |||
<!--Pharmacodynamics--> | |||
|PD=*Serum phosphate levels have been noted to decrease after administration of pamidronate disodium, presumably because of decreased release of phosphate from bone and increased renal excretion as parathyroid hormone levels, which are usually suppressed in [[hypercalcemia]] associated with malignancy, return toward normal. Phosphate therapy was administered in 30% of the patients in response to a decrease in serum phosphate levels. Phosphate levels usually returned toward normal within 7 to 10 days. | |||
*Urinary calcium/creatinine and urinary hydroxyproline/creatinine ratios decrease and usually return to within or below normal after treatment with pamidronate disodium. These changes occur within the first week after treatment, as do decreases in serum calcium levels, and are consistent with an antiresorptive pharmacologic action. | |||
*Hypercalcemia of Malignancy | |||
:*Osteoclastic hyperactivity resulting in excessive bone resorption is the underlying pathophysiologic derangement in metastatic bone disease and hypercalcemia of malignancy. Excessive release of calcium into the blood as bone is resorbed results in polyuria and gastrointestinal disturbances, with progressive dehydration and decreasing glomerular filtration rate. This, in turn, results in increased renal resorption of calcium, setting up a cycle of worsening systemic [[hypercalcemia]]. Correction of excessive bone resorption and adequate fluid administration to correct volume deficits are therefore essential to the management of [[hypercalcemia]]. | |||
:*Most cases of hypercalcemia associated with malignancy occur in patients who have breast cancer; squamous-cell tumors of the lung or head and neck; renal-cell carcinoma; and certain hematologic malignancies, such as [[multiple myeloma]] and some types of lymphomas. A few less-common malignancies, including vasoactive intestinal-peptide-producing tumors and cholangiocarcinoma, have a high incidence of hypercalcemia as a metabolic complication. Patients who have hypercalcemia of malignancy can generally be divided into two groups, according to the pathophysiologic mechanism involved. | |||
:*In humoral [[hypercalcemia]], osteoclasts are activated and bone resorption is stimulated by factors such as parathyroid-hormone-related protein, which are elaborated by the tumor and circulate systemically. Humoral [[hypercalcemia]] usually occurs in squamous-cell malignancies of the lung or head and neck or in genitourinary tumors such as renal-cell carcinoma or ovarian cancer. Skeletal metastases may be absent or minimal in these patients. | |||
:*Extensive invasion of bone by tumor cells can also result in hypercalcemia due to local tumor products that stimulate bone resorption by [[osteoclasts]]. Tumors commonly associated with locally mediated hypercalcemia include breast cancer and [[multiple myeloma]]. | |||
:*Total serum calcium levels in patients who have hypercalcemia of malignancy may not reflect the severity of [[hypercalcemia]], since concomitant [[hypoalbuminemia]] is commonly present. Ideally, ionized calcium levels should be used to diagnose and follow hypercalcemic conditions; however, these are not commonly or rapidly available in many clinical situations. Therefore, adjustment of the total serum calcium value for differences in albumin levels is often used in place of measurement of ionized calcium; several nomograms are in use for this type of calculation. | |||
<!--Pharmacokinetics--> | |||
|PK=*The principal pharmacologic action of pamidronate disodium is inhibition of bone resorption. Although the mechanism of antiresorptive action is not completely understood, several factors are thought to contribute to this action. Pamidronate disodium adsorbs to calcium phosphate (hydroxyapatite) crystals in bone and may directly block dissolution of this mineral component of bone. In vitro studies also suggest that inhibition of osteoclast activity contributes to inhibition of bone resorption. In animal studies, at doses recommended for the treatment of [[hypercalcemia]], pamidronate disodium inhibits bone resorption apparently without inhibiting bone formation and mineralization. Of relevance to the treatment of hypercalcemia of malignancy is the finding that pamidronate disodium inhibits the accelerated bone resorption that results from osteoclast hyperactivity induced by various tumors in animal studies. | |||
*Pharmacokinetics | |||
:*Cancer patients (n=24) who had minimal or no bony involvement were given an intravenous infusion of 30, 60, or 90 mg of pamidronate disodium over 4 hours and 90 mg of pamidronate disodium over 24 hours (Table 1). | |||
*Distribution | |||
:*The mean ± SD body retention of pamidronate was calculated to be 54 ± 16% of the dose over 120 hours. | |||
*Metabolism | |||
:*Pamidronate is not metabolized and is exclusively eliminated by renal excretion. | |||
*Excretion | |||
:*After administration of 30, 60, and 90 mg of pamidronate disodium over 4 hours, and 90 mg of pamidronate disodium over 24 hours, an overall mean ± SD of 46 ± 16% of the drug was excreted unchanged in the urine within 120 hours. Cumulative urinary excretion was linearly related to dose. The mean ± SD elimination half-life is 28 ± 7 hours. Mean ± SD total and renal clearances of pamidronate were 107 ± 50 mL/min and 49 ± 28 mL/min, respectively. The rate of elimination from bone has not been determined. | |||
*Special Populations | |||
:*There are no data available on the effects of age, gender, or race on the pharmacokinetics of pamidronate. | |||
*Pediatric | |||
:*Pamidronate is not labeled for use in the pediatric population. | |||
*Renal Insufficiency | |||
:*The pharmacokinetics of pamidronate were studied in cancer patients (n=19) with normal and varying degrees of renal impairment. Each patient received a single 90 mg dose of pamidronate disodium infused over 4 hours. The renal clearance of pamidronate in patients was found to closely correlate with creatinine clearance (see Figure 1). A trend toward a lower percentage of drug excreted unchanged in urine was observed in renally impaired patients. Adverse experiences noted were not found to be related to changes in renal clearance of pamidronate. Given the recommended dose, 90 mg infused over 4 hours, excessive accumulation of pamidronate in renally impaired patients is not anticipated if pamidronate disodium is administered on a monthly basis. | |||
: [[File:{{PAGENAME}}11.png|thumb|none|600px|This image is provided by the National Library of Medicine.]] | |||
*Hepatic Insufficiency | |||
:*The pharmacokinetics of pamidronate were studied in male cancer patients at risk for bone metastases with normal hepatic function (n=6) and mild to moderate hepatic dysfunction (n=7). Each patient received a single 90 mg dose of pamidronate disodium infused over 4 hours. Although there was a statistically significant difference in the pharmacokinetics between patients with normal and impaired hepatic function, the difference was not considered clinically relevant. Patients with hepatic impairment exhibited higher mean AUC (53%) and Cmax (29%), and decreased plasma clearance (33%) values. Nevertheless, pamidronate was still rapidly cleared from the plasma. Drug levels were not detectable in patients by 12 to 36 hours after drug infusion. Because pamidronate disodium is administered on a monthly basis, drug accumulation is not expected. No changes in pamidronate disodium dosing regimen are recommended for patients with mild to moderate abnormal hepatic function. Pamidronate disodium has not been studied in patients with severe [[hepatic impairment]]. | |||
*Drug – Drug Interactions | |||
:*There are no human pharmacokinetic data for drug interactions with pamidronate disodium. | |||
: [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]] | |||
:*After intravenous administration of radiolabeled pamidronate in rats, approximately 50% to 60% of the compound was rapidly adsorbed by bone and slowly eliminated from the body by the kidneys. In rats given 10 mg/kg bolus injections of radiolabeled pamidronate disodium, approximately 30% of the compound was found in the liver shortly after administration and was then redistributed to bone or eliminated by the kidneys over 24 to 48 hours. Studies in rats injected with radiolabeled pamidronate disodium showed that the compound was rapidly cleared from the circulation and taken up mainly by bones, liver, spleen, teeth, and tracheal cartilage. Radioactivity was eliminated from most soft tissues within 1 to 4 days; was detectable in liver and spleen for 1 and 3 months, respectively; and remained high in bones, trachea, and teeth for 6 months after dosing. Bone uptake occurred preferentially in areas of high bone turnover. The terminal phase of elimination half-life in bone was estimated to be approximately 300 days. | |||
<!--Nonclinical Toxicology--> | |||
|nonClinToxic=*In a 104 week carcinogenicity study (daily oral administration) in rats, there was a positive dose response relationship for benign adrenal [[pheochromocytoma]] in males (P<0.00001). Although this condition was also observed in females, the incidence was not statistically significant. When the dose calculations were adjusted to account for the limited oral bioavailability of pamidronate disodium in rats, the lowest daily dose associated with adrenal pheochromocytoma was similar to the intended clinical dose. Adrenal pheochromocytoma was also observed in low numbers in the control animals and is considered a relatively common spontaneous neoplasm in the rat. Pamidronate disodium (daily oral administration) was not carcinogenic in an 80 week study in mice. | |||
*Pamidronate disodium was nonmutagenic in six mutagenicity assays: Ames test, Salmonella and Escherichia/liver-microsome test, nucleus-anomaly test, sister-chromatid-exchange study, point-mutation test, and micronucleus test in the rat. | |||
*In rats, decreased fertility occurred in first-generation offspring of parents who had received 150 mg/kg of pamidronate disodium orally; however, this occurred only when animals were mated with members of the same dose group. Pamidronate disodium has not been administered intravenously in such a study. | |||
*Animal Toxicology | |||
:*In both rats and dogs, nephropathy has been associated with intravenous (bolus and infusion) administration of pamidronate disodium. | |||
:*Two 7 day intravenous infusion studies were conducted in the dog wherein pamidronate disodium was given for 1, 4, or 24 hours at doses of 1 to 20 mg/kg for up to 7 days. In the first study, the compound was well tolerated at 3 mg/kg (1.7 x highest recommended human dose [HRHD] for a single intravenous infusion) when administered for 4 or 24 hours, but renal findings such as elevated BUN and creatinine levels and renal tubular necrosis occurred when 3 mg/kg was infused for 1 hour and at doses of ≥10 mg/kg. In the second study, slight renal tubular necrosis was observed in 1 male at 1 mg/kg when infused for 4 hours. Additional findings included elevated BUN levels in several treated animals and renal tubular dilation and/or inflammation at ≥1 mg/kg after each infusion time. | |||
:*Pamidronate disodium was given to rats at doses of 2, 6, and 20 mg/kg and to dogs at doses of 2, 4, 6, and 20 mg/kg as a 1 hour infusion, once a week, for 3 months followed by a 1 month recovery period. In rats, nephrotoxicity was observed at ≥6 mg/kg and included increased BUN and creatinine levels and tubular degeneration and necrosis. These findings were still present at 20 mg/kg at the end of the recovery period. In dogs, moribundity/death and renal toxicity occurred at 20 mg/kg as did kidney findings of elevated BUN and creatinine levels at ≥6 mg/kg and renal tubular degeneration at ≥4 mg/kg. The kidney changes were partially reversible at 6 mg/kg. In both studies, the dose level that produced no adverse renal effects was considered to be 2 mg/kg (1.1 x HRHD for a single intravenous infusion). | |||
<!--Clinical Studies--> | |||
|clinicalStudies=*In one double-blind clinical trial, 52 patients who had [[hypercalcemia]] of [[malignancy]] were enrolled to receive 30 mg, 60 mg, or 90 mg of pamidronate disodium as a single 24 hour intravenous infusion if their corrected serum calcium levels were ≥12 mg/dL after 48 hours of saline hydration. | |||
*The mean baseline-corrected serum calcium for the 30 mg, 60 mg, and 90 mg groups were 13.8 mg/dL, 13.8 mg/dL, and 13.3 mg/dL, respectively. | |||
*The majority of patients (64%) had decreases in albumin-corrected serum calcium levels by 24 hours after initiation of treatment. Mean-corrected serum calcium levels at days 2 to 7 after initiation of treatment with pamidronate disodium were significantly reduced from baseline in all three dosage groups. As a result, by 7 days after initiation of treatment with pamidronate disodium, 40%, 61%, and 100% of the patients receiving 30 mg, 60 mg, and 90 mg of pamidronate disodium, respectively, had normal-corrected serum calcium levels. Many patients (33% to 53%) in the 60 mg and 90 mg dosage groups continued to have normal-corrected serum calcium levels, or a partial response (≥15% decrease of corrected serum calcium from baseline), at Day 14. | |||
*In a second double-blind, controlled clinical trial, 65 cancer patients who had corrected serum calcium levels of ≥12.0 mg/dL after at least 24 hours of saline hydration were randomized to receive either 60 mg of pamidronate disodium as a single 24 hour intravenous infusion or 7.5 mg/kg of etidronate disodium as a 2 hour intravenous infusion daily for 3 days. Thirty patients were randomized to receive pamidronate disodium and 35 to receive etidronate disodium. | |||
*The mean baseline-corrected serum calcium for the pamidronate disodium 60 mg and etidronate disodium groups were 14.6 mg/dL and 13.8 mg/dL, respectively. | |||
*By Day 7, 70% of the patients in the pamidronate disodium group and 41% of the patients in the etidronate disodium group had normal-corrected serum calcium levels (P<0.05). When partial responders (≥15% decrease of serum calcium from baseline) were also included, the response rates were 97% for the pamidronate disodium group and 65% for the etidronate disodium group (P<0.01). Mean-corrected serum calcium for the pamidronate disodium and etidronate disodium groups decreased from baseline values to 10.4 and 11.2 mg/dL, respectively, on Day 7. At Day 14, 43% of patients in the pamidronate disodium group and 18% of patients in the etidronate disodium group still had normal-corrected serum calcium levels, or maintenance of a partial response. For responders in the pamidronate disodium and etidronate disodium groups, the median duration of response was similar (7 and 5 days, respectively). The time course of effect on corrected serum calcium is summarized in the following table. | |||
: [[File:{{PAGENAME}}02.png|thumb|none|600px|This image is provided by the National Library of Medicine.]] | |||
*In a third multicenter, randomized, parallel double-blind trial, a group of 69 cancer patients with hypercalcemia was enrolled to receive 60 mg of pamidronate disodium as a 4 or 24 hour infusion, which was compared to a saline treatment group. Patients who had a corrected serum calcium level of ≥12.0 mg/dL after 24 hours of saline hydration were eligible for this trial. | |||
*The mean baseline-corrected serum calcium levels for pamidronate disodium 60 mg 4 hour infusion, pamidronate disodium 60 mg 24 hour infusion, and saline infusion were 14.2 mg/dL, 13.7 mg/dL, and 13.7 mg/dL, respectively. | |||
*By Day 7 after initiation of treatment, 78%, 61%, and 22% of the patients had normal-corrected serum calcium levels for the 60 mg 4 hour infusion, 60 mg 24 hour infusion, and saline infusion, respectively. At Day 14, 39% of the patients in the pamidronate disodium 60 mg 4 hour infusion group and 26% of the patients in the pamidronate disodium 60 mg 24 hour infusion group had normal-corrected serum calcium levels or maintenance of a partial response. | |||
*For responders, the median duration of complete responses was 4 days and 6.5 days for pamidronate disodium 60 mg 4 hour infusion and pamidronate disodium 60 mg 24 hour infusion, respectively. | |||
*In all three trials, patients treated with pamidronate disodium had similar response rates in the presence or absence of bone metastases. Concomitant administration of [[furosemide]] did not affect response rates. | |||
*Thirty-two patients who had recurrent or refractory [[hypercalcemia]] of malignancy were given a second course of 60 mg of pamidronate disodium over a 4 or 24 hour period. Of these, 41% showed a complete response and 16% showed a partial response to the retreatment, and these responders had about a 3 mg/dL fall in mean-corrected serum calcium levels 7 days after retreatment. | |||
*In a fourth multicenter, randomized, double-blind trial, 103 patients with cancer and hypercalcemia (corrected serum calcium ≥12.0 mg/dL) received 90 mg of pamidronate disodium as a 2 hour infusion. The mean baseline corrected serum calcium was 14.0 mg/dL. Patients were not required to receive IV hydration prior to drug administration, but all subjects did receive at least 500 mL of IV saline hydration concomitantly with the pamidronate infusion. By Day 10 after drug infusion, 70% of patients had normal corrected serum calcium levels (<10.8 mg/dL). | |||
*Paget’s Disease | |||
:*[[Paget’s disease of bone]] ([[osteitis deformans]]) is an idiopathic disease characterized by chronic, focal areas of bone destruction complicated by concurrent excessive bone repair, affecting one or more bones. These changes result in thickened but weakened bones that may fracture or bend under stress. Signs and symptoms may be bone pain, deformity, fractures, neurological disorders resulting from cranial and spinal nerve entrapment and from spinal cord and brain stem compression, increased cardiac output to the involved bone, increased serum alkaline phosphatase levels (reflecting increased bone formation) and/or urine hydroxyproline excretion (reflecting increased bone resorption). | |||
*Clinical Trials | |||
:*In one double-blind clinical trial, 64 patients with moderate to severe Paget’s disease of bone were enrolled to receive 5 mg, 15 mg, or 30 mg of pamidronate disodium as a single 4 hour infusion on 3 consecutive days, for total doses of 15 mg, 45 mg, and 90 mg of pamidronate disodium. | |||
:*The mean baseline serum alkaline phosphatase levels were 1409 U/L, 983 U/L, and 1085 U/L, and the mean baseline urine hydroxyproline/[[creatinine]] ratios were 0.25, 0.19, and 0.19 for the 15 mg, 45 mg, and 90 mg groups, respectively. | |||
:*The effects of pamidronate disodium on serum [[alkaline phosphatase]] (SAP) and urine hydroxyproline/creatinine ratios (UOHP/C) are summarized in the following table: | |||
: [[File:{{PAGENAME}}03.png|thumb|none|600px|This image is provided by the National Library of Medicine.]] | |||
:*The median maximum percent decreases from baseline in serum alkaline phosphatase and urine hydroxyproline/creatinine ratios were 25%, 41%, and 57%, and 25%, 47%, and 61% for the 15 mg, 45 mg, and 90 mg groups, respectively. The median time to response (≥50% decrease) for serum alkaline phosphatase was approximately 1 month for the 90 mg group, and the response duration ranged from 1 to 372 days. | |||
:*No statistically significant differences between treatment groups, or statistically significant changes from baseline were observed for the bone pain response, mobility, and global evaluation in the 45 mg and 90 mg groups. Improvement in radiologic lesions occurred in some patients in the 90 mg group. | |||
:*Twenty-five patients who had Paget’s disease were retreated with 90 mg of pamidronate disodium. Of these, 44% had a ≥50% decrease in serum alkaline phosphatase from baseline after treatment, and 39% had a ≥50% decrease in urine hydroxyproline/creatinine ratio from baseline after treatment. | |||
*Osteolytic Bone Metastases of Breast Cancer and Osteolytic Lesions of Multiple Myeloma | |||
:*Osteolytic bone metastases commonly occur in patients with [[multiple myeloma]] or [[breast cancer]]. These cancers demonstrate a phenomenon known as osteotropism, meaning they possess an extraordinary affinity for bone. The distribution of osteolytic bone metastases in these cancers is predominantly in the axial skeleton, particularly the spine, pelvis, and ribs, rather than the appendicular skeleton, although lesions in the proximal femur and humerus are not uncommon. This distribution is similar to the red bone marrow in which slow blood flow possibly assists attachment of metastatic cells. The surface-to-volume ratio of trabecular bone is much higher than cortical bone, and therefore disease processes tend to occur more floridly in trabecular bone than at sites of cortical tissue. | |||
:*These bone changes can result in patients having evidence of osteolytic skeletal destruction leading to severe bone pain that requires either radiation therapy or narcotic analgesics (or both) for symptomatic relief. These changes also cause pathologic fractures of bone in both the axial and appendicular skeleton. Axial skeletal fractures of the vertebral bodies may lead to [[spinal cord compression]] or vertebral body collapse with significant neurologic complications. Also, patients may experience episode(s) of [[hypercalcemia]]. | |||
*Clinical Trials | |||
:*In a double-blind, randomized, placebo-controlled trial, 392 patients with advanced multiple myeloma were enrolled to receive pamidronate disodium or placebo in addition to their underlying antimyeloma therapy to determine the effect of pamidronate disodium on the occurrence of skeletal-related events (SREs). SREs were defined as episodes of pathologic fractures, radiation therapy to bone, surgery to bone, and [[spinal cord compression]]. Patients received either 90 mg of pamidronate disodium or placebo as a monthly 4 hour intravenous infusion for 9 months. Of the 392 patients, 377 were evaluable for efficacy (196 pamidronate disodium, 181 placebo). The proportion of patients developing any SRE was significantly smaller in the pamidronate disodium group (24% vs 41%, P<0.001), and the mean skeletal morbidity rate (#SRE/year) was significantly smaller for pamidronate disodium patients than for placebo patients (mean: 1.1 vs 2.1, P<0.02). The times to the first SRE occurrence, pathologic fracture, and radiation to bone were significantly longer in the pamidronate disodium group (P=.001, .006, and .046, respectively). Moreover, fewer pamidronate disodium patients suffered any pathologic fracture (17% vs 30%, P=.004) or needed radiation to bone (14% vs 22%, P=.049). | |||
:*In addition, decreases in pain scores from baseline occurred at the last measurement for those pamidronate disodium patients with pain at baseline (P=.026) but not in the placebo group. At the last measurement, a worsening from baseline was observed in the placebo group for the Spitzer quality of life variable (P<.001) and ECOG performance status (P<.011) while there was no significant deterioration from baseline in these parameters observed in pamidronate disodium-treated patients.* | |||
:*After 21 months, the proportion of patients experiencing any skeletal event remained significantly smaller in the pamidronate disodium group than the placebo group (P=.015). In addition, the mean skeletal morbidity rate (#SRE/year) was 1.3 vs 2.2 for pamidronate disodium patients vs placebo patients (P=.008), and time to first SRE was significantly longer in the pamidronate disodium group compared to placebo (P=.016). Fewer pamidronate disodium patients suffered vertebral pathologic fractures (16% vs 27%, P=.005). Survival of all patients was not different between treatment groups. | |||
:*Two double-blind, randomized, placebo-controlled trials compared the safety and efficacy of 90 mg of pamidronate disodium infused over 2 hours every 3 to 4 weeks for 24 months to that of placebo in preventing SREs in breast cancer patients with osteolytic bone metastases who had one or more predominantly lytic metastases of at least 1 cm in diameter: one in patients being treated with antineoplastic chemotherapy and the second in patients being treated with hormonal antineoplastic therapy at trial entry. | |||
:*382 patients receiving chemotherapy were randomized, 185 to pamidronate disodium and 197 to placebo. 372 patients receiving hormonal therapy were randomized, 182 to pamidronate disodium and 190 to placebo. All but three patients were evaluable for efficacy. Patients were followed for 24 months of therapy or until they went off study. Median duration of follow-up was 13 months in patients receiving chemotherapy and 17 months in patients receiving hormone therapy. Twenty-five percent of the patients in the chemotherapy study and 37% of the patients in the hormone therapy study received pamidronate disodium for 24 months. The efficacy results are shown in the table below: | |||
: [[File:{{PAGENAME}}04.png|thumb|none|600px|This image is provided by the National Library of Medicine.]] | |||
:*Bone lesion response was radiographically assessed at baseline and at 3, 6, and 12 months. The complete + partial response rate was 33% in pamidronate disodium patients and 18% in placebo patients treated with chemotherapy (P=.001). No difference was seen between pamidronate disodium and placebo in hormonally-treated patients. | |||
:*Pain and analgesic scores, ECOG performance status and Spitzer quality of life index were measured at baseline and periodically during the trials. The changes from baseline to the last measurement carried forward are shown in the following table: | |||
: [[File:{{PAGENAME}}05.png|thumb|none|600px|This image is provided by the National Library of Medicine.]] | |||
<!--How Supplied--> | |||
|howSupplied=* Pamidronate Disodium Injection is available as follows: | |||
*Vials – 3 mg/mL, 10 mL vial - each contains 30 mg of Pamidronate Disodium and 470 mg of Mannitol, USP in 10 mL Water for Injection, USP. | |||
:*Carton of 1 vial. NDC 67457-472-10. | |||
*Vials – 9 mg/mL, 10 mL vial - each contains 90 mg of Pamidronate Disodium and 375 mg of Mannitol, USP in 10 mL Water for Injection, USP. | |||
:*Carton of 1 vial. NDC 67457-610-10. | |||
*Storage: Store at 20° to 25°C (68° to 77°F.) | |||
<!--Patient Counseling Information--> | |||
|fdaPatientInfo=There is limited information regarding <i>Patient Counseling Information</i> of {{PAGENAME}} in the drug label. | |||
<!--Precautions with Alcohol--> | |||
|alcohol=* Alcohol-{{PAGENAME}} interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication. | |||
<!--Brand Names--> | |||
|brandNames=* PAMIDRONATE DISODIUM®<ref>{{Cite web | title = PAMIDRONATE DISODIUM pamidronate disodium injection | url = http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=82e8deb5-2368-4267-8286-b7782acca952 }}</ref> | |||
<!--Look-Alike Drug Names--> | |||
|lookAlike=<!--Drug Shortage Status--> | |||
|drugShortage= | |||
}} | |||
{{PillImage | |||
|fileName=No image.jpg | |||
}} | |||
{{LabelImage | |||
|fileName={{PAGENAME}}09.png | |||
}} | }} | ||
{{LabelImage | |||
|fileName={{PAGENAME}}10.png | |||
}} | |||
<!--Pill Image--> | |||
<!--Label Display Image--> | |||
<!--Category--> | |||
< | |||
[[Category:Drug]] | |||
Latest revision as of 15:28, 20 February 2015
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Vignesh Ponnusamy, M.B.B.S. [2]
Disclaimer
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Overview
Pamidronic acid is a bisphosphonate that is FDA approved for the treatment of hypercalcemia of malignancy, Paget's disease, osteolytic bone metastases of breast cancer and osteolytic lesions of multiple myeloma. Common adverse reactions include hypertension, injection site reactiion, hypocalcemia, hypokalemia, hypomagnesemia, hypophosphatemia, loss of appetite, nausea, vomiting, anemia, urinary tract infectious disease, cough, dyspnea, fatigue, and malaise.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Hypercalcemia of Malignancy
- Pamidronate disodium, in conjunction with adequate hydration, is indicated for the treatment of moderate or severe hypercalcemia associated with malignancy, with or without bone metastases. Patients who have either epidermoid or non-epidermoid tumors respond to treatment with pamidronate disodium. Vigorous saline hydration, an integral part of hypercalcemia therapy, should be initiated promptly and an attempt should be made to restore the urine output to about 2 L/day throughout treatment. Mild or asymptomatic hypercalcemia may be treated with conservative measures (i.e., saline hydration, with or without loop diuretics). Patients should be hydrated adequately throughout the treatment, but overhydration, especially in those patients who have cardiac failure, must be avoided. Diuretic therapy should not be employed prior to correction of hypovolemia. The safety and efficacy of pamidronate disodium in the treatment of hypercalcemia associated with hyperparathyroidism or with other non-tumor-related conditions has not been established.
- Moderate Hypercalcemia
- The recommended dose of pamidronate disodium in moderate hypercalcemia (corrected serum calcium* of approximately 12 to 13.5 mg/dL) is 60 to 90 mg given as a SINGLE-DOSE, intravenous infusion over 2 to 24 hours. Longer infusions (i.e., >2 hours) may reduce the risk of renal toxicity, particularly in patients with preexisting renal insufficiency.
- Severe Hypercalcemia
- The recommended dose of pamidronate disodium in severe hypercalcemia (corrected serum calcium* >13.5 mg/dL) is 90 mg given as a SINGLE-DOSE, intravenous infusion over 2 to 24 hours. Longer infusions (i.e., >2 hours) may reduce the risk of renal toxicity, particularly in patients with preexisting renal insufficiency.
- Albumin-corrected serum calcium (CCa, mg/dL) = serum calcium, mg/dL + 0.8 (4.0-serum albumin, g/dL).
- Retreatment
- A limited number of patients have received more than one treatment with pamidronate disodium for hypercalcemia. Retreatment with pamidronate disodium, in patients who show complete or partial response initially, may be carried out if serum calcium does not return to normal or remain normal after initial treatment. It is recommended that a minimum of 7 days elapse before retreatment, to allow for full response to the initial dose. The dose and manner of retreatment is identical to that of the initial therapy.
Paget’s Disease
- Pamidronate disodium is indicated for the treatment of patients with moderate to severe Paget’s disease of bone. The effectiveness of pamidronate disodium was demonstrated primarily in patients with serum alkaline phosphatase ≥3 times the upper limit of normal. Pamidronate disodium therapy in patients with Paget’s disease has been effective in reducing serum alkaline phosphatase and urinary hydroxyproline levels by ≥50% in at least 50% of patients, and by ≥30% in at least 80% of patients. Pamidronate disodium therapy has also been effective in reducing these biochemical markers in patients with Paget’s disease who failed to respond, or no longer responded to other treatments.
- The recommended dose of pamidronate disodium in patients with moderate to severe Paget’s disease of bone is 30 mg daily, administered as a 4 hour infusion on 3 consecutive days for a total dose of 90 mg.
- Retreatment
- A limited number of patients with Paget’s disease have received more than one treatment of pamidronate disodium in clinical trials. When clinically indicated, patients should be retreated at the dose of initial therapy.
Osteolytic Bone Metastases of Breast Cancer and Osteolytic Lesions of Multiple Myeloma
- Pamidronate disodium is indicated, in conjunction with standard antineoplastic therapy, for the treatment of osteolytic bone metastases of breast cancer and osteolytic lesions of multiple myeloma. The pamidronate disodium treatment effect appeared to be smaller in the study of breast cancer patients receiving hormonal therapy than in the study of those receiving chemotherapy, however, overall evidence of clinical benefit has been demonstrated.
- Osteolytic Bone Lesions of Multiple Myeloma
- The recommended dose of pamidronate disodium in patients with osteolytic bone lesions of multiple myeloma is 90 mg administered as a 4 hour infusion given on a monthly basis.
- Patients with marked Bence-Jones proteinuria and dehydration should receive adequate hydration prior to pamidronate disodium infusion.
- Limited information is available on the use of pamidronate disodium in multiple myeloma patients with a serum creatinine ≥3.0 mg/dL.
- Patients who receive pamidronate disodium should have serum creatinine assessed prior to each treatment. Treatment should be withheld for renal deterioration. In a clinical study, renal deterioration was defined as follows:
- For patients with normal baseline creatinine, increase of 0.5 mg/dL.
- For patients with abnormal baseline creatinine, increase of 1.0 mg/dL.
- In this clinical study, pamidronate disodium treatment was resumed only when the creatinine returned to within 10% of the baseline value.
- The optimal duration of therapy is not yet known, however, in a study of patients with myeloma, final analysis after 21 months demonstrated overall benefits (see Clinical Trials section).
- Osteolytic Bone Metastases of Breast Cancer
- The recommended dose of pamidronate disodium in patients with osteolytic bone metastases is 90 mg administered over a 2 hour infusion given every 3 to 4 weeks.
- Pamidronate disodium has been frequently used with doxorubicin, fluorouracil, cyclophosphamide, methotrexate, mitoxantrone, vinblastine, dexamethasone, prednisone, melphalan, vincristine, megesterol, and tamoxifen. It has been given less frequently with etoposide, cisplatin, cytarabine, paclitaxel, and aminoglutethimide.
- Patients who receive pamidronate disodium should have serum creatinine assessed prior to each treatment. Treatment should be withheld for renal deterioration. In a clinical study, renal deterioration was defined as follows:
- For patients with normal baseline creatinine, increase of 0.5 mg/dL.
- For patients with abnormal baseline creatinine, increase of 1.0 mg/dL.
- In this clinical study, pamidronate disodium treatment was resumed only when the creatinine returned to within 10% of the baseline value.
- The optimal duration of therapy is not known, however, in two breast cancer studies, final analyses performed after 24 months of therapy demonstrated overall benefit.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Pamidronic acid in adult patients.
Non–Guideline-Supported Use
Complex regional pain syndrome, type I
- IV pamidronate 60 mg administered once daily over an interval of 3 consecutive days.[1]
Disorder of joint of spine
- 6 months a monthly IV infusion of pamidronate 60 mg.[2]
Drug-induced osteoporosis; Prophylaxis - Gonad regulating hormone adverse reaction
- IV pamidronate 60 mg.[3]
Hypercalcemia, Associated with tamoxifen-induced tumor flare
- Single IV infusion of pamidronate, at doses ranging from 30 to 90 mg. (determined by severity of hypercalcemia).[4]
Osteopenia (Acute); Prophylaxis - Total replacement of hip
- Single postoperative IV infusion of pamidronate 90 mg.[5]
Osteoporosis due to corticosteroids
- Oral pamidronate for 12 months.[6]
Postmenopausal osteoporosis
- 300 mg pamidronate orally once daily for 4 weeks every 16 weeks.[7]
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Pamidronic acid in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Pamidronic acid in pediatric patients.
Non–Guideline-Supported Use
Osteogenesis imperfecta
- Pamidronate by slow IV infusion over 3 hours for 3 consecutive days.[8]
Osteopenia - Tetraplegic cerebral palsy
- IV pamidronate dosed at 1 mg/kg (total daily dose not less than 15 mg or greater than 30 mg) and given daily for 3 consecutive days every 3 months for 1 year.[9]
Contraindications
- Pamidronate disodium is contraindicated in patients with clinically significant hypersensitivity to pamidronate disodium or other bisphosphonates.
Warnings
- Deterioration in Renal Function
- Bisphosphonates, including pamidronate disodium, have been associated with renal toxicity manifested as deterioration of renal function and potential renal failure.
- Due to the risk of clinically significant deterioration in renal function, which may progress to renal failure, single doses of pamidronate disodium should not exceed 90 mg. Renal deterioration, progression to renal failure, and dialysis have been reported in patients after the initial or a single dose of pamidronate disodium.
- Focal segmental glomerulosclerosis (including the collapsing variant) with or without nephrotic syndrome, which may lead to renal failure, has been reported in pamidronate disodium–treated patients, particularly in the setting of multiple myeloma and breast cancer. Some of these patients had gradual improvement in renal status after pamidronate disodium was discontinued.
- Patients who receive pamidronate disodium should have serum creatinine assessed prior to each treatment. Patients treated with pamidronate disodium for bone metastases should have the dose withheld if renal function has deteriorated.
- PREGNANCY: pamidronate disodium should not be used during pregnancy
- Pamidronate disodium may cause fetal harm when administered to a pregnant woman.
- There are no studies in pregnant women using pamidronate disodium. If the patient becomes pregnant while taking this drug, the patient should be apprised of the potential harm to the fetus. Women of childbearing potential should be advised to avoid becoming pregnant.
- Studies conducted in young rats have reported the disruption of dental dentine formation following single- and multi-dose administration of bisphosphonates. The clinical significance of these findings is unknown.
Precautions
- General
- Standard hypercalcemia-related metabolic parameters, such as serum levels of calcium, phosphate, magnesium, and potassium, should be carefully monitored following initiation of therapy with pamidronate disodium. Cases of asymptomatic hypophosphatemia (12%), hypokalemia (7%), hypomagnesemia (11%), and hypocalcemia (5% to 12%), were reported in pamidronate disodium-treated patients. Rare cases of symptomatic hypocalcemia (including tetany) have been reported in association with pamidronate therapy. If hypocalcemia occurs, short-term calcium therapy may be necessary. In Paget’s disease of bone, 17% of patients treated with 90 mg of pamidronate disodium showed serum calcium levels below 8 mg/dL.
- Patients with a history of thyroid surgery may have relative hypoparathyroidism that may predispose to hypocalcemia with pamidronate disodium.
- Renal Insufficiency
- Pamidronate disodium is excreted intact primarily via the kidney, and the risk of renal adverse reactions may be greater in patients with impaired renal function. Patients who receive pamidronate disodium should have serum creatinine assessed prior to each treatment. In patients receiving pamidronate disodium for bone metastases, who show evidence of deterioration in renal function, pamidronate disodium treatment should be withheld until renal function returns to baseline.
- In clinical trials, patients with renal impairment (serum creatinine >3.0 mg/dL) have not been studied. Limited pharmacokinetic data exist in patients with creatinine clearance <;<30 mL/min. For the treatment of bone metastases, the use of pamidronate disodium in patients with severe renal impairment is not recommended. In other indications, clinical judgement should determine whether the potential benefit outweighs the potential risk in such patients.
- Osteonecrosis of the Jaw
- Osteonecrosis of the jaw (ONJ) has been reported predominantly in cancer patients treated with intravenous biphosphonates, including pamidronate disodium. Many of these patients were also receiving chemotherapy and corticosteroids which may be risk factors for ONJ. Postmarketing experience and the literature suggest a greater frequency of reports of ONJ based on tumor type (advanced breast cancer, multiple myeloma), and dental status (dental extraction, periodontal disease, local trauma including poorly fitting dentures). Many reports of ONJ involved patients with signs of local infection including osteomyelitis.
- Cancer patients should maintain good oral hygiene and should have a dental examination with preventive dentistry prior to treatment with bisphophonates.
- While on treatment, these patients should avoid invasive dental procedures if possible. For patients who develop ONJ while on bisphosphonate therapy, dental surgey may exacerbate the condition. For patients requiring dental procedures, there are no data available to suggest whether discontinuation of bisphosphonate treatment reduces the risk of ONJ. Clinical judgement of the treating physician should guide the management plan of each patient based on individual benefit/risk assessment.
- Musculoskeletal Pain
- In post-marketing experience, severe and occasionally incapacitating bone, joint, and/or muscle pain has been reported in patients taking biphosphonates. However, such reports have been infrequent. This category of drugs includes pamidronate disodium injection. The time to onset of symptoms varied from one day to several months after starting the drug. Most patients had relief of symptoms after stopping. A subset had recurrence of symptoms when rechallanged with the same drug or another biphosphonate.
- Laboratory Tests
- Patients who receive pamidronate disodium should have serum creatinine assessed prior to each treatment. Serum calcium, electrolytes, phosphate, magnesium, and CBC, differential, and hematocrit/hemoglobin must be closely monitored in patients treated with pamidronate disodium. Patients who have preexisting anemia, leukopenia, or thrombocytopenia should be monitored carefully in the first 2 weeks following treatment.
Adverse Reactions
Clinical Trials Experience
Hypercalcemia of Malignancy
- Transient mild elevation of temperature by at least 1°C was noted 24 to 48 hours after administration of pamidronate disodium in 34% of patients in clinical trials. In the saline trial, 18% of patients had a temperature elevation of at least 1°C 24 to 48 hours after treatment.
- Drug-related local soft-tissue symptoms (redness, swelling or induration and pain on palpation) at the site of catheter insertion were most common in patients treated with 90 mg of pamidronate disodium. Symptomatic treatment resulted in rapid resolution in all patients.
- Rare cases of uveitis, iritis, scleritis, and episcleritis have been reported, including one case of scleritis, and one case of uveitis upon separate rechallenges.
- Five of 231 patients (2%) who received pamidronate disodium during the four U.S. controlled hypercalcemia clinical studies were reported to have had seizures, 2 of whom had preexisting seizure disorders. None of the seizures were considered to be drug-related by the investigators. However, a possible relationship between the drug and the occurrence of seizures cannot be ruled out. It should be noted that in the saline arm 1 patient (4%) had a seizure.
- There are no controlled clinical trials comparing the efficacy and safety of 90 mg pamidronate disodium over 24 hours to 2 hours in patients with hypercalcemia of malignancy. However, a comparison of data from separate clinical trials suggests that the overall safety profile in patients who received 90 mg pamidronate disodium over 24 hours is similar to those who received 90 mg pamidronate disodium over 2 hours. The only notable differences observed were an increase in the proportion of patients in the pamidronate 24 hour group who experienced fluid overload and electrolyte/mineral abnormalities.
- At least 15% of patients treated with pamidronate disodium for hypercalcemia of malignancy also experienced the following adverse events during a clinical trial:
General
Fluid overload, generalized pain
Cardiovascular
Gastrointestinal
Abdominal pain, anorexia, constipation, nausea, vomiting
Genitourinary
Musculoskeletal
Laboratory abnormality
Anemia, hypokalemia, hypomagnesemia, hypophosphatemia
- Many of these adverse experiences may have been related to the underlying disease state. The following table lists the adverse experiences considered to be treatment-related during comparative, controlled U.S. trials.
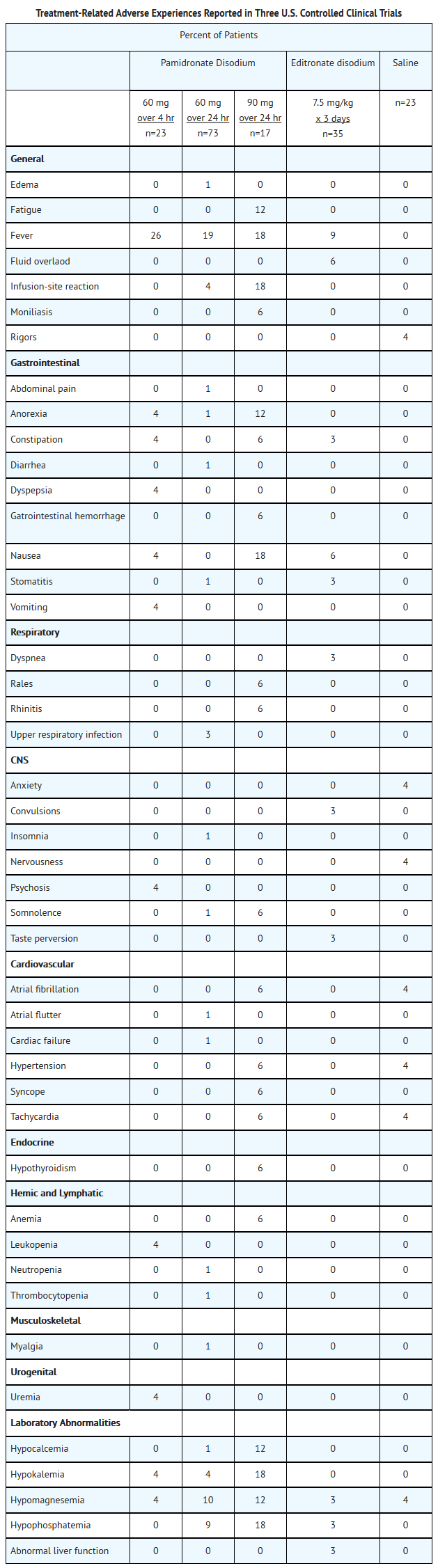
This image is provided by the National Library of Medicine.

Paget’s Disease
- Transient mild elevation of temperature >1°C above pretreatment baseline was noted within 48 hours after completion of treatment in 21% of the patients treated with 90 mg of pamidronate disodium in clinical trials.
- Drug-related musculoskeletal pain and nervous system symptoms (dizziness, headache, paresthesia, increased sweating) were more common in patients with Paget’s disease treated with 90 mg of pamidronate disodium than in patients with hypercalcemia of malignancy treated with the same dose.
- Adverse experiences considered to be related to trial drug, which occurred in at least 5% of patients with Paget’s disease treated with 90 mg of pamidronate disodium in two U.S. clinical trials, were fever, nausea, back pain, and bone pain.
- At least 10% of all pamidronate disodium-treated patients with Paget’s disease also experienced the following adverse experiences during clinical trials:
Cardiovascular
Musculoskeletal
Nervous system
- Most of these adverse experiences may have been related to the underlying disease state.
Osteolytic Bone Metastases of Breaset Cancer and Osteolytic Lesions of Multiple Myeloma
- The most commonly reported (>15%) adverse experiences occurred with similar frequencies in the pamidronate disodium and placebo treatment groups, and most of these adverse experiences may have been related to the underlying disease state or cancer therapy.
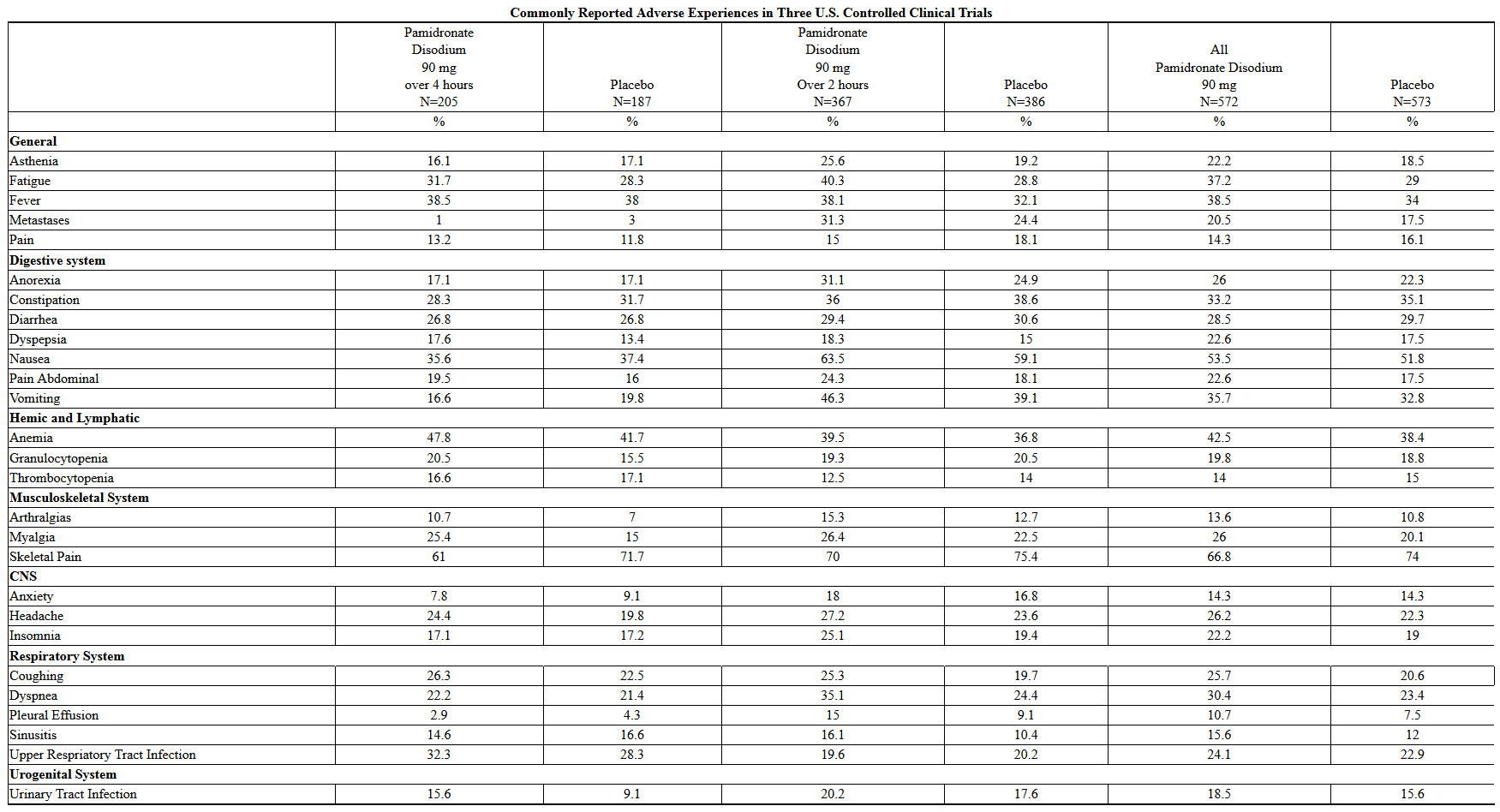
This image is provided by the National Library of Medicine.

- Of the toxicities commonly associated with chemotherapy, the frequency of vomiting, anorexia, and anemia were slightly more common in the pamidronate disodium patients whereas stomatitis and alopecia occurred at a frequency similar to that in placebo patients. In the breast cancer trials, mild elevations of serum creatinine occurred in 18.5% of pamidronate disodium patients and 12.3% of placebo patients. Mineral and electrolyte disturbances, including hypocalcemia, were reported rarely and in similar percentages of pamidronate disodium-treated patients compared with those in the placebo group. The reported frequencies of hypocalcemia, hypokalemia, hypophophatemia, and hypomagnesemia for pamidronate disodium-treated patients were 3.3%, 10.5%, 1.7%, and 4.4%, respectively, and for placebo-treated patients were 1.2%, 12%, 1.7%, and 4.5%, respectively. In previous hypercalcemia of malignancy trials, patients treated with pamidronate disodium (60 or 90 mg over 24 hours) developed electrolyte abnormalities more frequently.
- Arthralgias and myalgias were reported slightly more frequently in the pamidronate disodium group than in the placebo group (13.6% and 26% vs 10.8% and 20.1%, respectively).
- In multiple myeloma patients, there were five pamidronate disodium-related serious and unexpected adverse experiences. Four of these were reported during the 12 month extension of the multiple myeloma trial. Three of the reports were of worsening renal function developing in patients with progressive multiple myeloma or multiple myeloma-associated amyloidosis. The fourth report was the adult respiratory distress syndrome developing in a patient recovering from pneumonia and acute gangrenous cholecystitis. One pamidronate disodium-treated patient experienced an allergic reaction characterized by swollen and itchy eyes, runny nose, and scratchy throat within 24 hours after the sixth infusion.
- In the breast cancer trials, there were four pamidronate disodium-related adverse experiences, all moderate in severity, that caused a patient to discontinue participation in the trial. One was due to interstitial pneumonitis, another to malaise and dyspnea. One pamidronate disodium patient discontinued the trial due to a symptomatic hypocalcemia. Another pamidronate disodium patient discontinued therapy due to severe bone pain after each infusion, which the investigator felt was trial-drug-related.
Renal Toxicity
- In a study of the safety and efficacy of pamidronate disodium 90 mg (2 hour infusion) versus Zometa® 4 mg (15 minute infusion) in bone metastases patients with multiple myeloma or breast cancer, renal deterioration was defined as an increase in serum creatinine of 0.5 mg/dL for patients with normal baseline creatinine (<1.4 mg/dL) or an increase of 1.0 mg/dL for patients with an abnormal baseline creatinine (≥1.4 mg/dL). The following are data on the incidence of renal deterioration in patients in this trial. See table below.
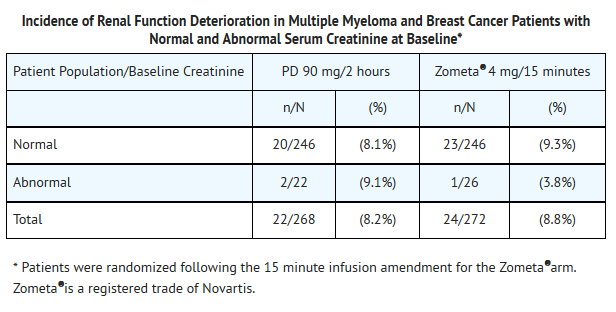
This image is provided by the National Library of Medicine.

Postmarketing Experience
- The following adverse reactions have been reported in post-marketing use: General : reactivation of Herpes simplex and Herpes zoster, influenza-like symptoms; CNS : confusion and visual hallucinations, sometimes in the presence of electrolyte imbalance; Skin : rash, pruritus; Special senses : conjunctivitis; Renal : focal segmental glomerulosclerosis including the collapsing variant, nephrotic syndrome; Laboratory abnormalities : hyperkalemia, hypernatremia, hematuria. Rare instances of allergic manifestations have been reported, including hypotension, dyspnea, or angioedema, and very rarely, anaphylactic shock. Pamidronate disodium is contraindicated in patients with clinically significant hypersensitivity to pamidronate disodium or other bisphosphonates.
- Cases of osteonecrosis (primarily involving the jaw) have been reported predominantly in cancer patients treated with intravenous bisphosphonates, including pamidronate disodium. Many of these patients were also receiving chemotherapy and corticosteroids which may be risk factors for ONJ. Data suggest a greater frequency of reports of ONJ in certain cancers, such as advanced breast cancer and multiple myeloma. The majority of the reported cases are in cancer patients following invasive dental procedures, such as tooth extraction. It is therefore prudent to avoid invasive dental procrdures as recovery may be prolonged.
Drug Interactions
- Concomitant administration of a loop diuretic had no effect on the calcium-lowering action of pamidronate disodium.
- Caution is indicated when pamidronate disodium is used with other potentially nephrotoxic drugs.
- In multiple myeloma patients, the risk of renal dysfunction may be increased when pamidronate disodium is used in combination with thalidomide.
Use in Specific Populations
Pregnancy
- Pregnancy Category D
- There are no adequate and well-controlled studies in pregnant women.
- Bolus intravenous studies conducted in rats and rabbits determined that pamidronate disodium produces maternal toxicity and embryo/fetal effects when given during organogenesis at doses of 0.6 to 8.3 times the highest recommended human dose for a single intravenous infusion. As it has been shown that pamidronate disodium can cross the placenta in rats and has produced marked maternal and nonteratogenic embryo/fetal effects in rats and rabbits, it should not be given to women during pregnancy.
- Bisphosphonates are incorporated into the bone matrix, from where they are gradually released over periods of weeks to years. The extent of bisphosphonate incorporation into adult bone, and hence, the amount available for release back into the systematic circulation, is directly related to the total dose and duration of bisphosphonate use. Although there are no data on fetal risk in humans, bisphosphonates do cause fetal harm in animals, and animal data suggest that uptake of bisphosphonates into fetal bone is greater than into maternal bone. Therefore, there is a theoretical risk of fetal harm (e.g., skeletal and other abnormalities) if a woman becomes pregnant after completing a course of bisphosphonate therapy. The impact of variables such as time between cessation of bisphosphonate therapy to conception, the particular bisphosphonate used, and the route of administration (intravenous versus oral) on this risk has not been established.
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Pamidronic acid in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Pamidronic acid during labor and delivery.
Nursing Mothers
- It is not known whether pamidronate disodium is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when pamidronate disodium is administered to a nursing woman.
Pediatric Use
- Safety and effectiveness of pamidronate disodium in pediatric patients have not been established.
Geriatic Use
- Of the total number of subjects in clinical studies of pamidronate disodium, approximately 20% were 65 and over, while approximately 15% were 75 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
Gender
There is no FDA guidance on the use of Pamidronic acid with respect to specific gender populations.
Race
There is no FDA guidance on the use of Pamidronic acid with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Pamidronic acid in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Pamidronic acid in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Pamidronic acid in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Pamidronic acid in patients who are immunocompromised.
Administration and Monitoring
Administration
- Intravenous
Monitoring
There is limited information regarding Monitoring of Pamidronic acid in the drug label.
IV Compatibility
There is limited information regarding IV Compatibility of Pamidronic acid in the drug label.
Overdosage
Acute Overdose
- There have been several cases of drug maladministration of intravenous pamidronate disodium in hypercalcemia patients with total doses of 225 mg to 300 mg given over 21/2 to 4 days. All of these patients survived, but they experienced hypocalcemia that required intravenous and/or oral administration of calcium. Single doses of pamidronate disodium should not exceed 90 mg and the duration of the intravenous infusion should be no less than 2 hours.
- In addition, one obese woman (95 kg) who was treated with 285 mg of pamidronate disodium/day for 3 days experienced high fever (39.5°C), hypotension (from 170/90 mmHg to 90/60 mmHg), and transient taste perversion, noted about 6 hours after the first infusion. The fever and hypotension were rapidly corrected with steroids.
- If overdosage occurs, symptomatic hypocalcemia could also result; such patients should be treated with short-term intravenous calcium.
Chronic Overdose
There is limited information regarding Chronic Overdose of Pamidronic acid in the drug label.
Pharmacology

| |
Pamidronic acid
| |
| Systematic (IUPAC) name | |
| (3-amino-1-hydroxypropane-1,1-diyl)bis(phosphonic acid) | |
| Identifiers | |
| CAS number | |
| ATC code | M05 |
| PubChem | |
| DrugBank | |
| Chemical data | |
| Formula | Template:OrganicBox atomTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox |
| Mol. mass | 235.07 g/mol |
| SMILES | & |
| Pharmacokinetic data | |
| Bioavailability | n/a |
| Protein binding | 54% |
| Metabolism | Nil |
| Half life | 28 ± 7 hours |
| Excretion | Renal |
| Therapeutic considerations | |
| Pregnancy cat. | |
| Legal status |
POM(UK) [[Prescription drug|Template:Unicode-only]](US) |
| Routes | Intravenous |
Mechanism of Action
- The principal pharmacologic action of pamidronate disodium is inhibition of bone resorption. Although the mechanism of antiresorptive action is not completely understood, several factors are thought to contribute to this action. Pamidronate disodium adsorbs to calcium phosphate (hydroxyapatite) crystals in bone and may directly block dissolution of this mineral component of bone. In vitro studies also suggest that inhibition of osteoclast activity contributes to inhibition of bone resorption. In animal studies, at doses recommended for the treatment of hypercalcemia, pamidronate disodium inhibits bone resorption apparently without inhibiting bone formation and mineralization. Of relevance to the treatment of hypercalcemia of malignancy is the finding that pamidronate disodium inhibits the accelerated bone resorption that results from osteoclast hyperactivity induced by various tumors in animal studies.
Structure
- Pamidronate Disodium is a sterile bone-resorption inhibitor available in 30 mg and 90 mg vials for intravenous administration. The pamidronate disodium obtained by combining pamidronic acid and sodium hydroxide is provided in a sterile, ready to use solution for injection. Each mL of the 30 mg vial contains, 3 mg Pamidronate Disodium, 47 mg Mannitol, USP; Water for Injection, USP, q.s.; Phosphoric acid to adjust pH. Each mL of the 90 mg vial contains, 9 mg Pamidronate Disodium, 37.5 mg Mannitol, USP; Water for Injection, USP, q.s.; Phosphoric acid to adjust pH. The pH of a 1% solution of pamidronate disodium in distilled water is approximately 8.3. Pamidronate, a member of the group of chemical compounds known as bisphosphonates, is an analog of pyrophosphate. Pamidronate disodium is designated chemically as phosphonic acid (3-amino-1-hydroxypropylidene) bis-, disodium salt, and its structural formula is:
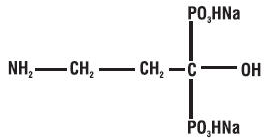
This image is provided by the National Library of Medicine.

- Pamidronate disodium is soluble in water and in 2N sodium hydroxide, sparingly soluble in 0.1N hydrochloric acid and in 0.1N acetic acid, and practically insoluble in organic solvents. Its molecular formula is C3H9NO7P2Na2 and its molecular weight is 279.1 (calculated as the anhydrous form).
- Inactive Ingredients: Mannitol, Phosphoric acid (for adjustment to pH range of 6.0 to 7.0) and Water for Injection.
Pharmacodynamics
- Serum phosphate levels have been noted to decrease after administration of pamidronate disodium, presumably because of decreased release of phosphate from bone and increased renal excretion as parathyroid hormone levels, which are usually suppressed in hypercalcemia associated with malignancy, return toward normal. Phosphate therapy was administered in 30% of the patients in response to a decrease in serum phosphate levels. Phosphate levels usually returned toward normal within 7 to 10 days.
- Urinary calcium/creatinine and urinary hydroxyproline/creatinine ratios decrease and usually return to within or below normal after treatment with pamidronate disodium. These changes occur within the first week after treatment, as do decreases in serum calcium levels, and are consistent with an antiresorptive pharmacologic action.
- Hypercalcemia of Malignancy
- Osteoclastic hyperactivity resulting in excessive bone resorption is the underlying pathophysiologic derangement in metastatic bone disease and hypercalcemia of malignancy. Excessive release of calcium into the blood as bone is resorbed results in polyuria and gastrointestinal disturbances, with progressive dehydration and decreasing glomerular filtration rate. This, in turn, results in increased renal resorption of calcium, setting up a cycle of worsening systemic hypercalcemia. Correction of excessive bone resorption and adequate fluid administration to correct volume deficits are therefore essential to the management of hypercalcemia.
- Most cases of hypercalcemia associated with malignancy occur in patients who have breast cancer; squamous-cell tumors of the lung or head and neck; renal-cell carcinoma; and certain hematologic malignancies, such as multiple myeloma and some types of lymphomas. A few less-common malignancies, including vasoactive intestinal-peptide-producing tumors and cholangiocarcinoma, have a high incidence of hypercalcemia as a metabolic complication. Patients who have hypercalcemia of malignancy can generally be divided into two groups, according to the pathophysiologic mechanism involved.
- In humoral hypercalcemia, osteoclasts are activated and bone resorption is stimulated by factors such as parathyroid-hormone-related protein, which are elaborated by the tumor and circulate systemically. Humoral hypercalcemia usually occurs in squamous-cell malignancies of the lung or head and neck or in genitourinary tumors such as renal-cell carcinoma or ovarian cancer. Skeletal metastases may be absent or minimal in these patients.
- Extensive invasion of bone by tumor cells can also result in hypercalcemia due to local tumor products that stimulate bone resorption by osteoclasts. Tumors commonly associated with locally mediated hypercalcemia include breast cancer and multiple myeloma.
- Total serum calcium levels in patients who have hypercalcemia of malignancy may not reflect the severity of hypercalcemia, since concomitant hypoalbuminemia is commonly present. Ideally, ionized calcium levels should be used to diagnose and follow hypercalcemic conditions; however, these are not commonly or rapidly available in many clinical situations. Therefore, adjustment of the total serum calcium value for differences in albumin levels is often used in place of measurement of ionized calcium; several nomograms are in use for this type of calculation.
Pharmacokinetics
- The principal pharmacologic action of pamidronate disodium is inhibition of bone resorption. Although the mechanism of antiresorptive action is not completely understood, several factors are thought to contribute to this action. Pamidronate disodium adsorbs to calcium phosphate (hydroxyapatite) crystals in bone and may directly block dissolution of this mineral component of bone. In vitro studies also suggest that inhibition of osteoclast activity contributes to inhibition of bone resorption. In animal studies, at doses recommended for the treatment of hypercalcemia, pamidronate disodium inhibits bone resorption apparently without inhibiting bone formation and mineralization. Of relevance to the treatment of hypercalcemia of malignancy is the finding that pamidronate disodium inhibits the accelerated bone resorption that results from osteoclast hyperactivity induced by various tumors in animal studies.
- Pharmacokinetics
- Cancer patients (n=24) who had minimal or no bony involvement were given an intravenous infusion of 30, 60, or 90 mg of pamidronate disodium over 4 hours and 90 mg of pamidronate disodium over 24 hours (Table 1).
- Distribution
- The mean ± SD body retention of pamidronate was calculated to be 54 ± 16% of the dose over 120 hours.
- Metabolism
- Pamidronate is not metabolized and is exclusively eliminated by renal excretion.
- Excretion
- After administration of 30, 60, and 90 mg of pamidronate disodium over 4 hours, and 90 mg of pamidronate disodium over 24 hours, an overall mean ± SD of 46 ± 16% of the drug was excreted unchanged in the urine within 120 hours. Cumulative urinary excretion was linearly related to dose. The mean ± SD elimination half-life is 28 ± 7 hours. Mean ± SD total and renal clearances of pamidronate were 107 ± 50 mL/min and 49 ± 28 mL/min, respectively. The rate of elimination from bone has not been determined.
- Special Populations
- There are no data available on the effects of age, gender, or race on the pharmacokinetics of pamidronate.
- Pediatric
- Pamidronate is not labeled for use in the pediatric population.
- Renal Insufficiency
- The pharmacokinetics of pamidronate were studied in cancer patients (n=19) with normal and varying degrees of renal impairment. Each patient received a single 90 mg dose of pamidronate disodium infused over 4 hours. The renal clearance of pamidronate in patients was found to closely correlate with creatinine clearance (see Figure 1). A trend toward a lower percentage of drug excreted unchanged in urine was observed in renally impaired patients. Adverse experiences noted were not found to be related to changes in renal clearance of pamidronate. Given the recommended dose, 90 mg infused over 4 hours, excessive accumulation of pamidronate in renally impaired patients is not anticipated if pamidronate disodium is administered on a monthly basis.
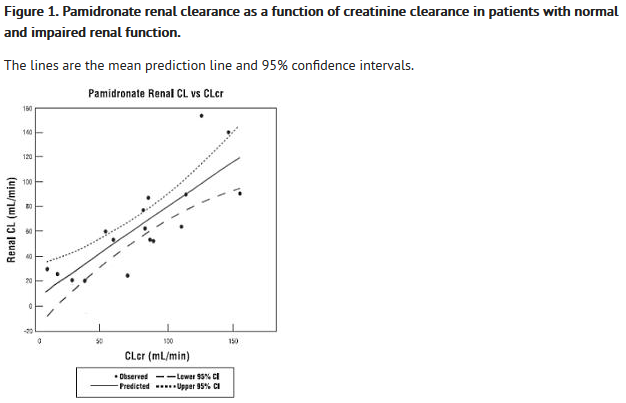
This image is provided by the National Library of Medicine.

- Hepatic Insufficiency
- The pharmacokinetics of pamidronate were studied in male cancer patients at risk for bone metastases with normal hepatic function (n=6) and mild to moderate hepatic dysfunction (n=7). Each patient received a single 90 mg dose of pamidronate disodium infused over 4 hours. Although there was a statistically significant difference in the pharmacokinetics between patients with normal and impaired hepatic function, the difference was not considered clinically relevant. Patients with hepatic impairment exhibited higher mean AUC (53%) and Cmax (29%), and decreased plasma clearance (33%) values. Nevertheless, pamidronate was still rapidly cleared from the plasma. Drug levels were not detectable in patients by 12 to 36 hours after drug infusion. Because pamidronate disodium is administered on a monthly basis, drug accumulation is not expected. No changes in pamidronate disodium dosing regimen are recommended for patients with mild to moderate abnormal hepatic function. Pamidronate disodium has not been studied in patients with severe hepatic impairment.
- Drug – Drug Interactions
- There are no human pharmacokinetic data for drug interactions with pamidronate disodium.
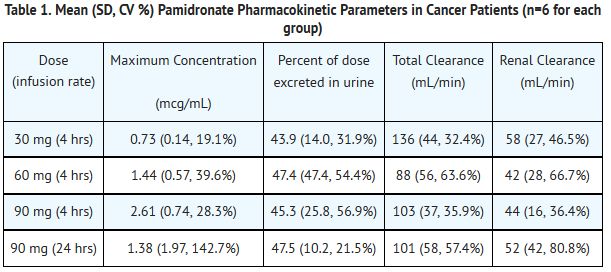
This image is provided by the National Library of Medicine.

- After intravenous administration of radiolabeled pamidronate in rats, approximately 50% to 60% of the compound was rapidly adsorbed by bone and slowly eliminated from the body by the kidneys. In rats given 10 mg/kg bolus injections of radiolabeled pamidronate disodium, approximately 30% of the compound was found in the liver shortly after administration and was then redistributed to bone or eliminated by the kidneys over 24 to 48 hours. Studies in rats injected with radiolabeled pamidronate disodium showed that the compound was rapidly cleared from the circulation and taken up mainly by bones, liver, spleen, teeth, and tracheal cartilage. Radioactivity was eliminated from most soft tissues within 1 to 4 days; was detectable in liver and spleen for 1 and 3 months, respectively; and remained high in bones, trachea, and teeth for 6 months after dosing. Bone uptake occurred preferentially in areas of high bone turnover. The terminal phase of elimination half-life in bone was estimated to be approximately 300 days.
Nonclinical Toxicology
- In a 104 week carcinogenicity study (daily oral administration) in rats, there was a positive dose response relationship for benign adrenal pheochromocytoma in males (P<0.00001). Although this condition was also observed in females, the incidence was not statistically significant. When the dose calculations were adjusted to account for the limited oral bioavailability of pamidronate disodium in rats, the lowest daily dose associated with adrenal pheochromocytoma was similar to the intended clinical dose. Adrenal pheochromocytoma was also observed in low numbers in the control animals and is considered a relatively common spontaneous neoplasm in the rat. Pamidronate disodium (daily oral administration) was not carcinogenic in an 80 week study in mice.
- Pamidronate disodium was nonmutagenic in six mutagenicity assays: Ames test, Salmonella and Escherichia/liver-microsome test, nucleus-anomaly test, sister-chromatid-exchange study, point-mutation test, and micronucleus test in the rat.
- In rats, decreased fertility occurred in first-generation offspring of parents who had received 150 mg/kg of pamidronate disodium orally; however, this occurred only when animals were mated with members of the same dose group. Pamidronate disodium has not been administered intravenously in such a study.
- Animal Toxicology
- In both rats and dogs, nephropathy has been associated with intravenous (bolus and infusion) administration of pamidronate disodium.
- Two 7 day intravenous infusion studies were conducted in the dog wherein pamidronate disodium was given for 1, 4, or 24 hours at doses of 1 to 20 mg/kg for up to 7 days. In the first study, the compound was well tolerated at 3 mg/kg (1.7 x highest recommended human dose [HRHD] for a single intravenous infusion) when administered for 4 or 24 hours, but renal findings such as elevated BUN and creatinine levels and renal tubular necrosis occurred when 3 mg/kg was infused for 1 hour and at doses of ≥10 mg/kg. In the second study, slight renal tubular necrosis was observed in 1 male at 1 mg/kg when infused for 4 hours. Additional findings included elevated BUN levels in several treated animals and renal tubular dilation and/or inflammation at ≥1 mg/kg after each infusion time.
- Pamidronate disodium was given to rats at doses of 2, 6, and 20 mg/kg and to dogs at doses of 2, 4, 6, and 20 mg/kg as a 1 hour infusion, once a week, for 3 months followed by a 1 month recovery period. In rats, nephrotoxicity was observed at ≥6 mg/kg and included increased BUN and creatinine levels and tubular degeneration and necrosis. These findings were still present at 20 mg/kg at the end of the recovery period. In dogs, moribundity/death and renal toxicity occurred at 20 mg/kg as did kidney findings of elevated BUN and creatinine levels at ≥6 mg/kg and renal tubular degeneration at ≥4 mg/kg. The kidney changes were partially reversible at 6 mg/kg. In both studies, the dose level that produced no adverse renal effects was considered to be 2 mg/kg (1.1 x HRHD for a single intravenous infusion).
Clinical Studies
- In one double-blind clinical trial, 52 patients who had hypercalcemia of malignancy were enrolled to receive 30 mg, 60 mg, or 90 mg of pamidronate disodium as a single 24 hour intravenous infusion if their corrected serum calcium levels were ≥12 mg/dL after 48 hours of saline hydration.
- The mean baseline-corrected serum calcium for the 30 mg, 60 mg, and 90 mg groups were 13.8 mg/dL, 13.8 mg/dL, and 13.3 mg/dL, respectively.
- The majority of patients (64%) had decreases in albumin-corrected serum calcium levels by 24 hours after initiation of treatment. Mean-corrected serum calcium levels at days 2 to 7 after initiation of treatment with pamidronate disodium were significantly reduced from baseline in all three dosage groups. As a result, by 7 days after initiation of treatment with pamidronate disodium, 40%, 61%, and 100% of the patients receiving 30 mg, 60 mg, and 90 mg of pamidronate disodium, respectively, had normal-corrected serum calcium levels. Many patients (33% to 53%) in the 60 mg and 90 mg dosage groups continued to have normal-corrected serum calcium levels, or a partial response (≥15% decrease of corrected serum calcium from baseline), at Day 14.
- In a second double-blind, controlled clinical trial, 65 cancer patients who had corrected serum calcium levels of ≥12.0 mg/dL after at least 24 hours of saline hydration were randomized to receive either 60 mg of pamidronate disodium as a single 24 hour intravenous infusion or 7.5 mg/kg of etidronate disodium as a 2 hour intravenous infusion daily for 3 days. Thirty patients were randomized to receive pamidronate disodium and 35 to receive etidronate disodium.
- The mean baseline-corrected serum calcium for the pamidronate disodium 60 mg and etidronate disodium groups were 14.6 mg/dL and 13.8 mg/dL, respectively.
- By Day 7, 70% of the patients in the pamidronate disodium group and 41% of the patients in the etidronate disodium group had normal-corrected serum calcium levels (P<0.05). When partial responders (≥15% decrease of serum calcium from baseline) were also included, the response rates were 97% for the pamidronate disodium group and 65% for the etidronate disodium group (P<0.01). Mean-corrected serum calcium for the pamidronate disodium and etidronate disodium groups decreased from baseline values to 10.4 and 11.2 mg/dL, respectively, on Day 7. At Day 14, 43% of patients in the pamidronate disodium group and 18% of patients in the etidronate disodium group still had normal-corrected serum calcium levels, or maintenance of a partial response. For responders in the pamidronate disodium and etidronate disodium groups, the median duration of response was similar (7 and 5 days, respectively). The time course of effect on corrected serum calcium is summarized in the following table.
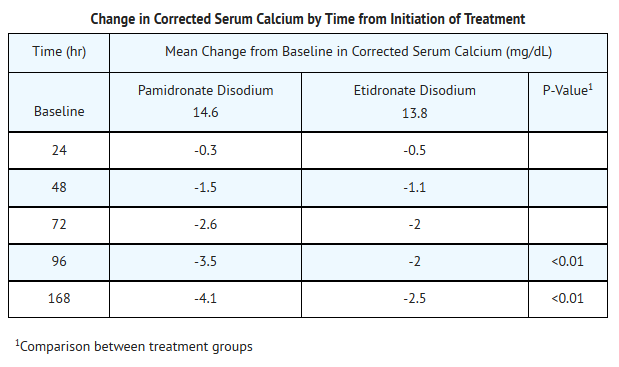
This image is provided by the National Library of Medicine.

- In a third multicenter, randomized, parallel double-blind trial, a group of 69 cancer patients with hypercalcemia was enrolled to receive 60 mg of pamidronate disodium as a 4 or 24 hour infusion, which was compared to a saline treatment group. Patients who had a corrected serum calcium level of ≥12.0 mg/dL after 24 hours of saline hydration were eligible for this trial.
- The mean baseline-corrected serum calcium levels for pamidronate disodium 60 mg 4 hour infusion, pamidronate disodium 60 mg 24 hour infusion, and saline infusion were 14.2 mg/dL, 13.7 mg/dL, and 13.7 mg/dL, respectively.
- By Day 7 after initiation of treatment, 78%, 61%, and 22% of the patients had normal-corrected serum calcium levels for the 60 mg 4 hour infusion, 60 mg 24 hour infusion, and saline infusion, respectively. At Day 14, 39% of the patients in the pamidronate disodium 60 mg 4 hour infusion group and 26% of the patients in the pamidronate disodium 60 mg 24 hour infusion group had normal-corrected serum calcium levels or maintenance of a partial response.
- For responders, the median duration of complete responses was 4 days and 6.5 days for pamidronate disodium 60 mg 4 hour infusion and pamidronate disodium 60 mg 24 hour infusion, respectively.
- In all three trials, patients treated with pamidronate disodium had similar response rates in the presence or absence of bone metastases. Concomitant administration of furosemide did not affect response rates.
- Thirty-two patients who had recurrent or refractory hypercalcemia of malignancy were given a second course of 60 mg of pamidronate disodium over a 4 or 24 hour period. Of these, 41% showed a complete response and 16% showed a partial response to the retreatment, and these responders had about a 3 mg/dL fall in mean-corrected serum calcium levels 7 days after retreatment.
- In a fourth multicenter, randomized, double-blind trial, 103 patients with cancer and hypercalcemia (corrected serum calcium ≥12.0 mg/dL) received 90 mg of pamidronate disodium as a 2 hour infusion. The mean baseline corrected serum calcium was 14.0 mg/dL. Patients were not required to receive IV hydration prior to drug administration, but all subjects did receive at least 500 mL of IV saline hydration concomitantly with the pamidronate infusion. By Day 10 after drug infusion, 70% of patients had normal corrected serum calcium levels (<10.8 mg/dL).
- Paget’s Disease
- Paget’s disease of bone (osteitis deformans) is an idiopathic disease characterized by chronic, focal areas of bone destruction complicated by concurrent excessive bone repair, affecting one or more bones. These changes result in thickened but weakened bones that may fracture or bend under stress. Signs and symptoms may be bone pain, deformity, fractures, neurological disorders resulting from cranial and spinal nerve entrapment and from spinal cord and brain stem compression, increased cardiac output to the involved bone, increased serum alkaline phosphatase levels (reflecting increased bone formation) and/or urine hydroxyproline excretion (reflecting increased bone resorption).
- Clinical Trials
- In one double-blind clinical trial, 64 patients with moderate to severe Paget’s disease of bone were enrolled to receive 5 mg, 15 mg, or 30 mg of pamidronate disodium as a single 4 hour infusion on 3 consecutive days, for total doses of 15 mg, 45 mg, and 90 mg of pamidronate disodium.
- The mean baseline serum alkaline phosphatase levels were 1409 U/L, 983 U/L, and 1085 U/L, and the mean baseline urine hydroxyproline/creatinine ratios were 0.25, 0.19, and 0.19 for the 15 mg, 45 mg, and 90 mg groups, respectively.
- The effects of pamidronate disodium on serum alkaline phosphatase (SAP) and urine hydroxyproline/creatinine ratios (UOHP/C) are summarized in the following table:
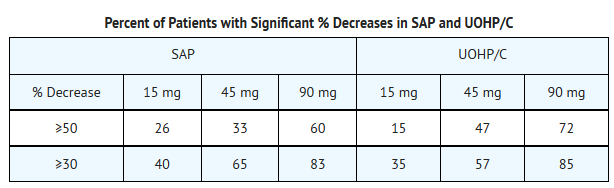
This image is provided by the National Library of Medicine.

- The median maximum percent decreases from baseline in serum alkaline phosphatase and urine hydroxyproline/creatinine ratios were 25%, 41%, and 57%, and 25%, 47%, and 61% for the 15 mg, 45 mg, and 90 mg groups, respectively. The median time to response (≥50% decrease) for serum alkaline phosphatase was approximately 1 month for the 90 mg group, and the response duration ranged from 1 to 372 days.
- No statistically significant differences between treatment groups, or statistically significant changes from baseline were observed for the bone pain response, mobility, and global evaluation in the 45 mg and 90 mg groups. Improvement in radiologic lesions occurred in some patients in the 90 mg group.
- Twenty-five patients who had Paget’s disease were retreated with 90 mg of pamidronate disodium. Of these, 44% had a ≥50% decrease in serum alkaline phosphatase from baseline after treatment, and 39% had a ≥50% decrease in urine hydroxyproline/creatinine ratio from baseline after treatment.
- Osteolytic Bone Metastases of Breast Cancer and Osteolytic Lesions of Multiple Myeloma
- Osteolytic bone metastases commonly occur in patients with multiple myeloma or breast cancer. These cancers demonstrate a phenomenon known as osteotropism, meaning they possess an extraordinary affinity for bone. The distribution of osteolytic bone metastases in these cancers is predominantly in the axial skeleton, particularly the spine, pelvis, and ribs, rather than the appendicular skeleton, although lesions in the proximal femur and humerus are not uncommon. This distribution is similar to the red bone marrow in which slow blood flow possibly assists attachment of metastatic cells. The surface-to-volume ratio of trabecular bone is much higher than cortical bone, and therefore disease processes tend to occur more floridly in trabecular bone than at sites of cortical tissue.
- These bone changes can result in patients having evidence of osteolytic skeletal destruction leading to severe bone pain that requires either radiation therapy or narcotic analgesics (or both) for symptomatic relief. These changes also cause pathologic fractures of bone in both the axial and appendicular skeleton. Axial skeletal fractures of the vertebral bodies may lead to spinal cord compression or vertebral body collapse with significant neurologic complications. Also, patients may experience episode(s) of hypercalcemia.
- Clinical Trials
- In a double-blind, randomized, placebo-controlled trial, 392 patients with advanced multiple myeloma were enrolled to receive pamidronate disodium or placebo in addition to their underlying antimyeloma therapy to determine the effect of pamidronate disodium on the occurrence of skeletal-related events (SREs). SREs were defined as episodes of pathologic fractures, radiation therapy to bone, surgery to bone, and spinal cord compression. Patients received either 90 mg of pamidronate disodium or placebo as a monthly 4 hour intravenous infusion for 9 months. Of the 392 patients, 377 were evaluable for efficacy (196 pamidronate disodium, 181 placebo). The proportion of patients developing any SRE was significantly smaller in the pamidronate disodium group (24% vs 41%, P<0.001), and the mean skeletal morbidity rate (#SRE/year) was significantly smaller for pamidronate disodium patients than for placebo patients (mean: 1.1 vs 2.1, P<0.02). The times to the first SRE occurrence, pathologic fracture, and radiation to bone were significantly longer in the pamidronate disodium group (P=.001, .006, and .046, respectively). Moreover, fewer pamidronate disodium patients suffered any pathologic fracture (17% vs 30%, P=.004) or needed radiation to bone (14% vs 22%, P=.049).
- In addition, decreases in pain scores from baseline occurred at the last measurement for those pamidronate disodium patients with pain at baseline (P=.026) but not in the placebo group. At the last measurement, a worsening from baseline was observed in the placebo group for the Spitzer quality of life variable (P<.001) and ECOG performance status (P<.011) while there was no significant deterioration from baseline in these parameters observed in pamidronate disodium-treated patients.*
- After 21 months, the proportion of patients experiencing any skeletal event remained significantly smaller in the pamidronate disodium group than the placebo group (P=.015). In addition, the mean skeletal morbidity rate (#SRE/year) was 1.3 vs 2.2 for pamidronate disodium patients vs placebo patients (P=.008), and time to first SRE was significantly longer in the pamidronate disodium group compared to placebo (P=.016). Fewer pamidronate disodium patients suffered vertebral pathologic fractures (16% vs 27%, P=.005). Survival of all patients was not different between treatment groups.
- Two double-blind, randomized, placebo-controlled trials compared the safety and efficacy of 90 mg of pamidronate disodium infused over 2 hours every 3 to 4 weeks for 24 months to that of placebo in preventing SREs in breast cancer patients with osteolytic bone metastases who had one or more predominantly lytic metastases of at least 1 cm in diameter: one in patients being treated with antineoplastic chemotherapy and the second in patients being treated with hormonal antineoplastic therapy at trial entry.
- 382 patients receiving chemotherapy were randomized, 185 to pamidronate disodium and 197 to placebo. 372 patients receiving hormonal therapy were randomized, 182 to pamidronate disodium and 190 to placebo. All but three patients were evaluable for efficacy. Patients were followed for 24 months of therapy or until they went off study. Median duration of follow-up was 13 months in patients receiving chemotherapy and 17 months in patients receiving hormone therapy. Twenty-five percent of the patients in the chemotherapy study and 37% of the patients in the hormone therapy study received pamidronate disodium for 24 months. The efficacy results are shown in the table below:
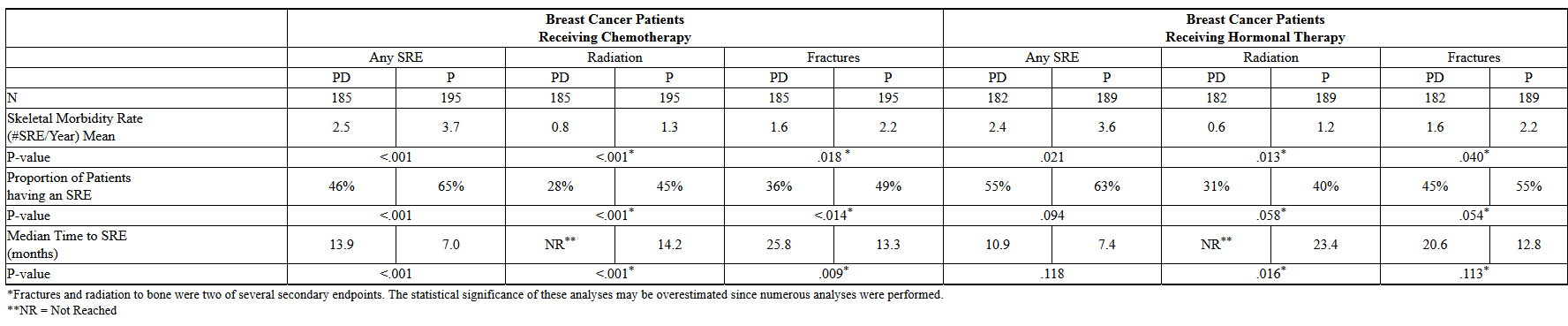
This image is provided by the National Library of Medicine.

- Bone lesion response was radiographically assessed at baseline and at 3, 6, and 12 months. The complete + partial response rate was 33% in pamidronate disodium patients and 18% in placebo patients treated with chemotherapy (P=.001). No difference was seen between pamidronate disodium and placebo in hormonally-treated patients.
- Pain and analgesic scores, ECOG performance status and Spitzer quality of life index were measured at baseline and periodically during the trials. The changes from baseline to the last measurement carried forward are shown in the following table:

This image is provided by the National Library of Medicine.

How Supplied
- Pamidronate Disodium Injection is available as follows:
- Vials – 3 mg/mL, 10 mL vial - each contains 30 mg of Pamidronate Disodium and 470 mg of Mannitol, USP in 10 mL Water for Injection, USP.
- Carton of 1 vial. NDC 67457-472-10.
- Vials – 9 mg/mL, 10 mL vial - each contains 90 mg of Pamidronate Disodium and 375 mg of Mannitol, USP in 10 mL Water for Injection, USP.
- Carton of 1 vial. NDC 67457-610-10.
- Storage: Store at 20° to 25°C (68° to 77°F.)
Storage
There is limited information regarding Pamidronic acid Storage in the drug label.
Images
Drug Images
{{#ask: Page Name::Pamidronic acid |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Pamidronic acid |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
There is limited information regarding Patient Counseling Information of Pamidronic acid in the drug label.
Precautions with Alcohol
- Alcohol-Pamidronic acid interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- PAMIDRONATE DISODIUM®[10]
Look-Alike Drug Names
There is limited information regarding Pamidronic acid Look-Alike Drug Names in the drug label.
Drug Shortage Status
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
- ↑ Kubalek I, Fain O, Paries J, Kettaneh A, Thomas M (2001). "Treatment of reflex sympathetic dystrophy with pamidronate: 29 cases". Rheumatology (Oxford). 40 (12): 1394–7. PMID 11752511.
- ↑ Maksymowych WP, Jhangri GS, Fitzgerald AA, LeClercq S, Chiu P, Yan A; et al. (2002). "A six-month randomized, controlled, double-blind, dose-response comparison of intravenous pamidronate (60 mg versus 10 mg) in the treatment of nonsteroidal antiinflammatory drug-refractory ankylosing spondylitis". Arthritis Rheum. 46 (3): 766–73. doi:10.1002/art.10139. PMID 11920413.
- ↑ Smith MR, McGovern FJ, Zietman AL, Fallon MA, Hayden DL, Schoenfeld DA; et al. (2001). "Pamidronate to prevent bone loss during androgen-deprivation therapy for prostate cancer". N Engl J Med. 345 (13): 948–55. doi:10.1056/NEJMoa010845. PMID 11575286.
- ↑ Nikolic-Tomasević Z, Jelic S, Popov I, Radosavljević D, Mitrović L (2001). "Tumor 'flare' hypercalcemia--an additional indication for bisphosphonates?". Oncology. 60 (2): 123–6. doi:55308 Check
|doi=value (help). PMID 11244326. - ↑ Wilkinson JM, Stockley I, Peel NF, Hamer AJ, Elson RA, Barrington NA; et al. (2001). "Effect of pamidronate in preventing local bone loss after total hip arthroplasty: a randomized, double-blind, controlled trial". J Bone Miner Res. 16 (3): 556–64. doi:10.1359/jbmr.2001.16.3.556. PMID 11277274.
- ↑ Reid IR, King AR, Alexander CJ, Ibbertson HK (1988). "Prevention of steroid-induced osteoporosis with (3-amino-1-hydroxypropylidene)-1,1-bisphosphonate (APD)". Lancet. 1 (8578): 143–6. PMID 2892989.
- ↑ Ryan PJ, Blake GM, Davie M, Haddaway M, Gibson T, Fogelman I (2000). "Intermittent oral disodium pamidronate in established osteoporosis: a 2 year double-masked placebo-controlled study of efficacy and safety". Osteoporos Int. 11 (2): 171–6. doi:10.1007/PL00004179. PMID 10793877.
- ↑ Alharbi M, Pinto G, Finidori G, Souberbielle JC, Guillou F, Gaubicher S; et al. (2009). "Pamidronate treatment of children with moderate-to-severe osteogenesis imperfecta: a note of caution". Horm Res. 71 (1): 38–44. doi:10.1159/000173740. PMID 19039235.
- ↑ Henderson RC, Lark RK, Kecskemethy HH, Miller F, Harcke HT, Bachrach SJ (2002). "Bisphosphonates to treat osteopenia in children with quadriplegic cerebral palsy: a randomized, placebo-controlled clinical trial". J Pediatr. 141 (5): 644–51. doi:10.1067/mpd.2002.128207. PMID 12410192.
- ↑ "PAMIDRONATE DISODIUM pamidronate disodium injection".
{{#subobject:
|Page Name=Pamidronic acid
|Pill Name=No image.jpg
|Drug Name=
|Pill Ingred=|+sep=;
|Pill Imprint=
|Pill Dosage={{{dosageValue}}} {{{dosageUnit}}}
|Pill Color=|+sep=;
|Pill Shape=
|Pill Size (mm)=
|Pill Scoring=
|Pill Image=
|Drug Author=
|NDC=
}}
{{#subobject:
|Label Page=Pamidronic acid |Label Name=Pamidronic acid09.png
}}
{{#subobject:
|Label Page=Pamidronic acid |Label Name=Pamidronic acid10.png
}}