Otitis media: Difference between revisions
Hardik Patel (talk | contribs) |
Hardik Patel (talk | contribs) |
||
| Line 5: | Line 5: | ||
{{CMG}} | {{CMG}} | ||
==Treatment== | ==Treatment== | ||
Revision as of 14:24, 6 December 2012
|
Otitis media Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Otitis media On the Web |
|
American Roentgen Ray Society Images of Otitis media |
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Treatment
Acute otitis media
Treatment of acute otitis media is controversial. Much of the controversy centers around the difficulty of distinguishing viral infection from bacterial infection and the fact that viral infection can progress to bacterial infection at any time. Primary care providers, such as general practitioners and pediatricians, often have a monocular otoscope and perhaps a tympanometer as their only diagnostic tools, which makes this distinction difficult, especially if the canal is small and there is wax in the ear that obscures a clear view of the eardrum. Also, an upset child's crying can cause the eardrum to look inflamed due to causing distention of the small blood vessels on it, mimicking the redness associated with otitis media. Because of a tradition of inappropriate prescribing of antibiotics for viral acute otitis media, their use has recently been condemned by many primary care practitioners for most cases of acute otitis media. Ear specialists tend to disagree with this philosophy and promote efforts to distinguish between viral and bacterial infection, so as to optimize treatment results by giving antibiotics only for bacterial infection. Acute bacterial otitis media can cause pain that leads to sleepless nights for both children and parents, can cause eardrum perforations, not all of which heal, and can spread to cause mastoiditis and/or meningitis, brain abscess, and even death if a severe infection goes untreated long enough. High fever can occur and can cause febrile seizures. Appropriate antibiotic administration prevents most such complications. On the other hand, it is generally agreed that acute otitis media that is purely viral will usually resolve without antibiotic treatment, although associated persistent middle ear effusions may require medical intervention.[1][2][3]
Many guidelines now suggest deferring the start of antibiotics for one to three days[4] avoiding the need for antibiotics for two out of three children[5] without adverse effect on longterm outcomes for those whose treatment is deferred.[6] First line antibiotic treatment, if warranted, is amoxicillin. If the bacteria is resistant, then amoxicillin-clavulanate or another penicillin derivative plus beta lactamase inhibitor is second line.
Prior to the invention of antibiotics, severe acute otits media was mainly remedied surgically by Myringotomy. An outpatient procedure, it consists of making a small incision in the tympanic membrane to relieve pressure build-up.
Chronic cases or with effusion
In chronic cases or with effusions present for months, surgery is sometimes performed by an otolaryngologist (ear, nose, and throat specialist) or by an otologist (ear specialist), to insert a grommet (called a "tympanostomy tube") into the eardrum to allow air to pass through into the middle ear, and thus release any pressure buildup and help clear excess fluid within.
For chronic cases (glue ear), it is possible to use the Valsalva maneuver to reestablish middle ear ventilation, although repeated use of the Valsalva maneuver can cause infected matter to enter the eye cavity and cause conjunctivitis.
Alternative therapies
Alternatives to conventional medical approaches include chiropractic and osteopathic spinal manipulations, targeted to relieve muscle tension to enhance lymphatic flow and allow normal opening of the Eustachian tube. Such alternatives are becoming increasingly widely used. Otitis Media has also been found to respond to homeopathic remedies.[7] Eardoc treatment reduces the fluids in the middle ear by opening the Eustachian tube. Its efficiency can be viewed and tested with a tympanometer.
Gallery
-
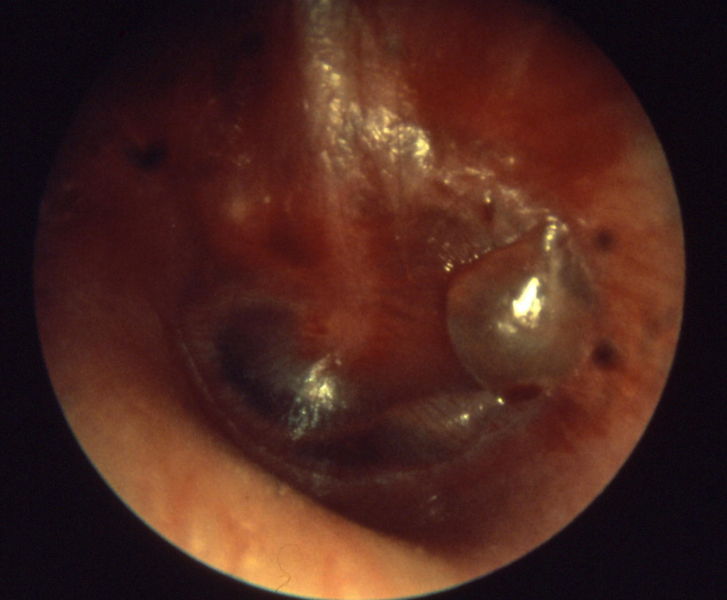
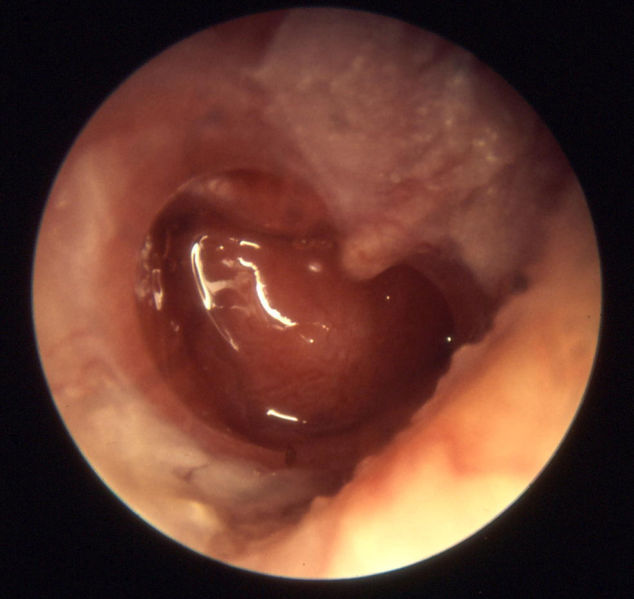
Otitis media acuta - Myringitis bullosa
-

-
Influenza
-
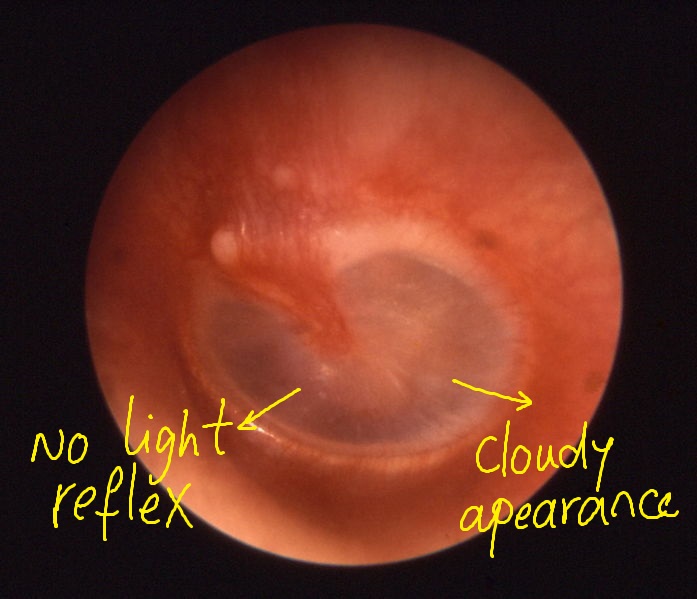
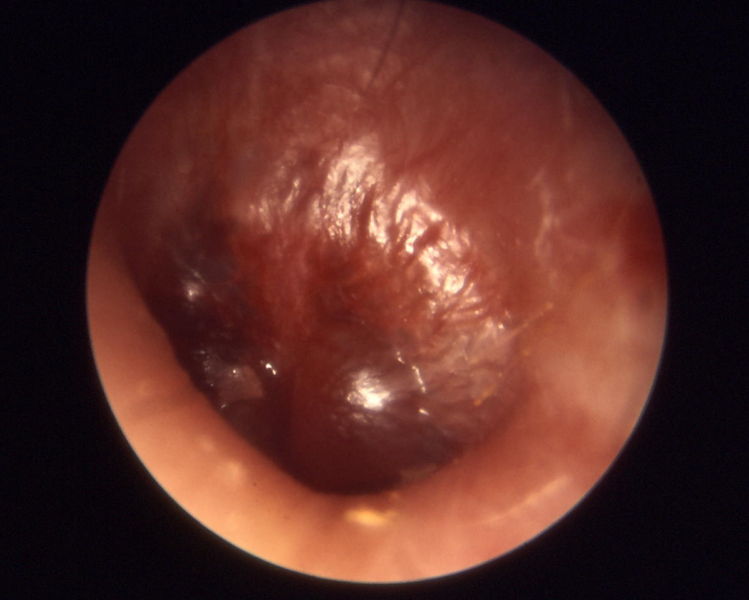
Otitis media acuta
-
Otitis media acuta
-
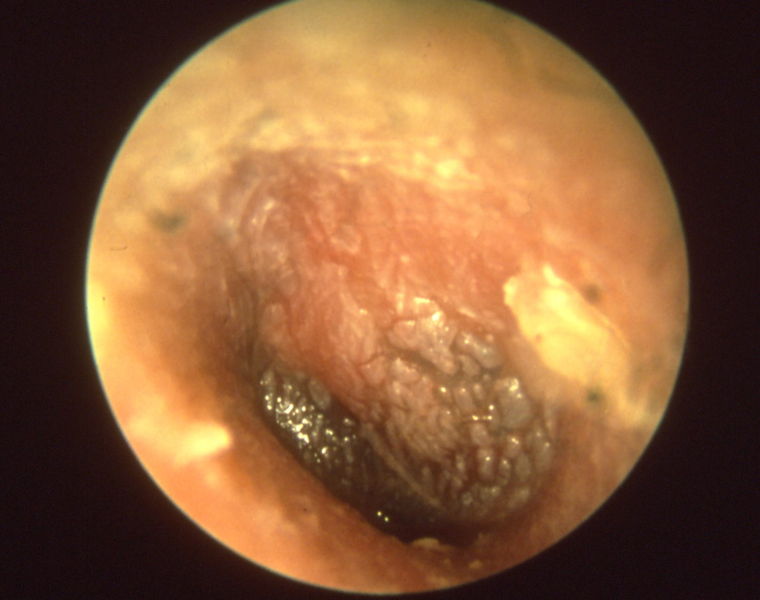
Otitis media chronica mesotympanalis
-

Otitis media chronica mesotympanalis
-
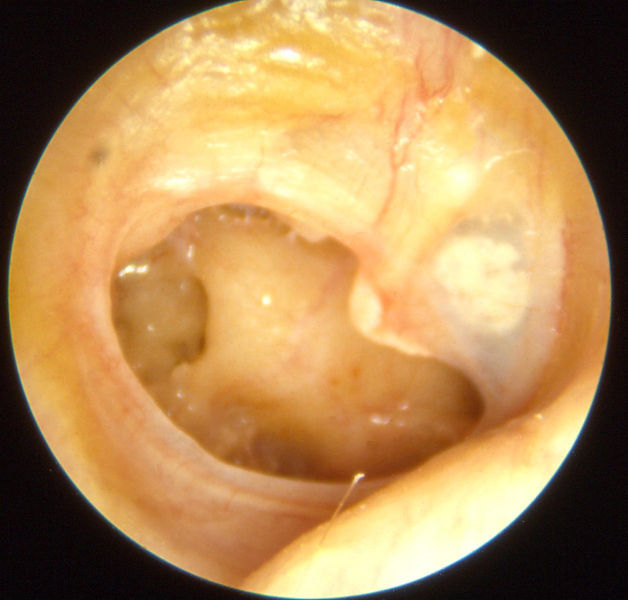
Otitis media chronica mesotympanalis
-
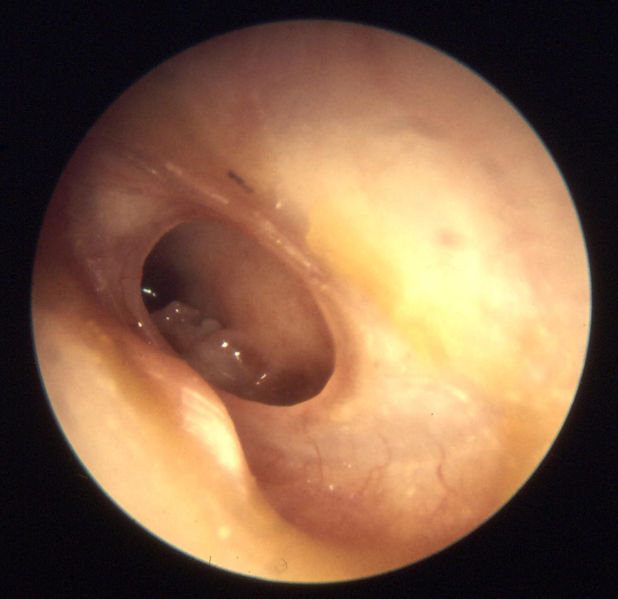
Otitis media chronica mesotympanalis









Sources
Template:Diseases of the ear and mastoid process Template:Common Cold ay:Jinchu usu bg:Отит da:Mellemørebetændelse de:Akute Mittelohrentzündung id:Otitis media it:Otite media la:Otitis media acuta nl:Middenoorontsteking qu:Rinri nanay fi:Korvatulehdus sv:Öroninflammation
- ↑ Damoiseaux R, van Balen F, Hoes A, Verheij T, de Melker R (2000). "Primary care based randomised, double blind trial of amoxicillin versus placebo for acute otitis media in children aged under 2 years". BMJ. 320 (7231): 350–4. PMID 10657332.
- ↑ Arroll B (2005). "Antibiotics for upper respiratory tract infections: an overview of Cochrane reviews". Respir Med. 99 (3): 255–61. PMID 15733498.
- ↑ Rovers MM, Glasziou P, Appelman CL, Burke P, McCormick DP, Damoiseaux RA, Gaboury I, Little P, Hoes AW. (2006). "Antibiotics for acute otitis media: a meta-analysis with individual patient data". Lancet. 368 (9545): 1429–35. PMID 17055944.
- ↑ Damoiseaux R (2005). "Antibiotic treatment for acute otitis media: time to think again". CMAJ. 172 (5): 657–8. PMID 15738492.
- ↑ Marchetti F, Ronfani L, Nibali S, Tamburlini G (2005). "Delayed prescription may reduce the use of antibiotics for acute otitis media: a prospective observational study in primary care". Arch Pediatr Adolesc Med. 159 (7): 679–84. PMID 15997003.
- ↑ Little P, Moore M, Warner G, Dunleavy J, Williamson I (2006). "Longer term outcomes from a randomised trial of prescribing strategies in otitis media". Br J Gen Pract. 56 (524): 176–82. PMID 16536957.
- ↑ Michael A. Schmidt (2003). Childhood Ear Infections: A Parent's Guide to Alternative Treatments. North Atlantic Books. ISBN 1556434421. [2] [3]