Leiomyoma
|
WikiDoc Resources for Leiomyoma |
|
Articles |
|---|
|
Most recent articles on Leiomyoma |
|
Media |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Leiomyoma at Clinical Trials.gov Clinical Trials on Leiomyoma at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Leiomyoma
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Leiomyoma Discussion groups on Leiomyoma Directions to Hospitals Treating Leiomyoma Risk calculators and risk factors for Leiomyoma
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Leiomyoma |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
For patient information, click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Roukoz A. Karam, M.D.[2]; Cafer Zorkun, M.D., Ph.D. [3]; Shanshan Cen, M.D. [4]; Ammu Susheela, M.D. [5]
Synonyms and keywords: Uterine myoma; Fibroid; Fibroids; Uterine; Fibroid Tumor; Fibroid Uterus; Uterine fibromyoma; Leiomyomata
Overview
Uterine leiomyoma was first discovered by Hippocrates in 460-375 B.C and called it “uterine stone”. Uterine leiomyoma may be classified according to their location into 3 subtypes: submucosal, subserous, and intramural. The pathogenesis of leiomyoma is characterized by benign smooth muscle neoplasm. They can occur in any organ, but the most common forms occur in the uterus, small bowel and the esophagus. Chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q has been associated with the development of leiomyoma. Uterine leiomyoma must be differentiated from other diseases that cause uterine mass, such as: uterine adenomyoma, pregnancy, hematometra, uterine sarcoma, uterine carcinosarcoma, and metastasis. Leiomyoma is more commonly observed among patients aged 40 years and older. Common risk factors in the development of uterine leiomyoma include African-American race, early menarche, prenatal exposure to diethylstilbestrol, having one or more pregnancies extending beyond 20 weeks, obesity, significant consumption of beef and other reds meats, hypertension, family history, and alcohol consumption. Physical examination may be remarkable for enlarged, mobile uterus with an irregular contour on bimanual pelvic examination. The mainstay of therapy for uterine leiomyoma is oral contraceptive pills, either combination pills or progestin-only, Gonadotropin-releasing hormone analogs. Surgery is also part of mainstay therapy for uterine leiomyoma.
Historical Perspective
- Uterine leiomyoma was first discovered by Hippocrates, an ancient Greek physician, in 460-375 B.C and called it “uterine stone”.
- In the second century AD, Galen described the lesion as "scleromas".
- In 1860 and 1863, Rokitansky and Klob coined the term fibroid.
- In 1854, Virchow, a German pathologist, demonstrated that those tumors originated from the uterine smooth muscle.
- In 1809, the first laparotomy was conducted by Ephraim McDowell to treat leiomyoma in Danville, USA.[1]
Classification
- Uterine leiomyoma may be classified according to the International Federation of Gynecology and Obstetrics (FIGO) classification system, based on their location in the uterus, into 8 subtypes:[2]
- Intramural myomas
- FIGO types 3, 4, and 5
- Located within the uterine wall
- Submucosal myomas
- Derived from myometrial cells below the endometrium and may protrude into the uterine cavity
- May be subclassified according to this protrusion:
- Type 0: pedunculated intracavitary
- Type 1: < 50% intramural
- Type 2: ≥ 50% itramural
- Subserosal myomas
- FIGO types 6 and 7
- Derived from myometrium at the at the serous surface of the uterus
- Cervical myomas
- FIGO type 8
- Usually located in the cervix
- Intramural myomas
Pathophysiology
- The pathogenesis of leiomyoma is characterized by benign smooth muscle neoplasm. They can occur in any organ, but the most common forms occur in the uterus, small bowel and the esophagus.
- It is thought that leiomyoma is the result of either transformation of normal uterine muscle cells into abnormal cells through somatic mutations, or through the growth of abnormal uterine muscle cells into tumors.[3][4]
- Genetic mutations involved in the pathogenesis of leiomyoma include: [5]
- t(12;14)(q14-q15;q23–24)
- del(7)(q22q32)
- Rearrangements involving 6p21, 10q, trisomy 12
- Deletions of 1p3q
- On gross pathology, round, well circumscribed, non-encapsulated, solid white or tan nodules, and whorled are characteristic findings of leiomyoma.[6]
- On microscopic histopathological analysis, elongated and spindle-shaped cells with a cigar-shaped nucleus are characteristic findings of leiomyoma.[6]
-
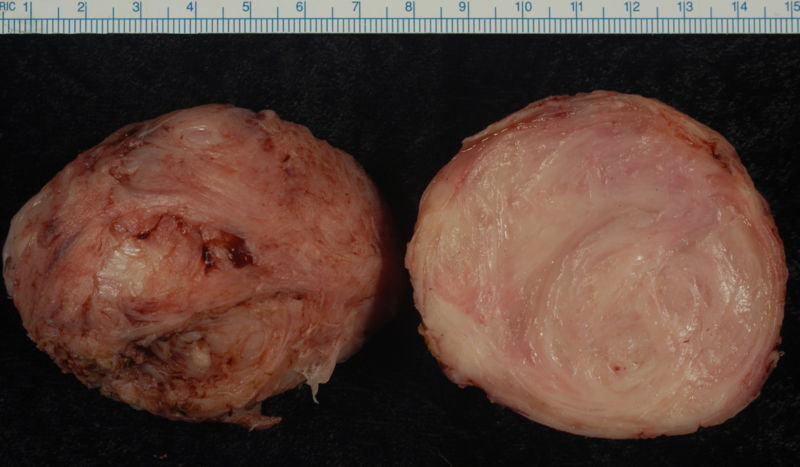
Leiomyoma enucleated from a uterus. External surface on left; cut surface on right
-
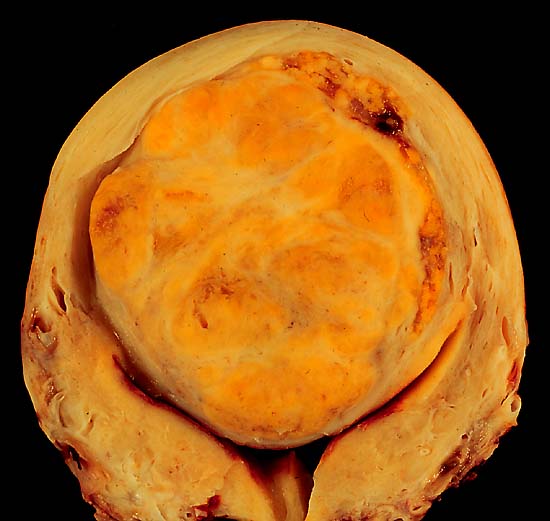
A large, solitary leiomyoma in the uterus, distoring the endometrial cavity into a Y shape by splaying and pressing it downwards.
(Image courtesy of Ed Uthman, MD)


Causes
- Chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q have been associated with the development of leiomyoma.[5]
Differentiating Leiomyoma from other Diseases
Leiomyoma is a cause of abnormal uterine bleeding and can result in infertility. There are several diseases which can result in excessive uterine bleeding and the following table is a description of various causes of excessive uterine bleeding.
| Clinical Features | Physical Examination | Diagnostic Findings | |
|---|---|---|---|
| Endometriosis |
|
|
|
| Adenomyosis[7] |
|
|
|
| Submucous uterine leiomyomas[8] |
|
|
|
| Pelvic Inflammatory disease[9] |
|
|
|
| Pelvic congestion Syndrome[10] |
|
|
|
Epidemiology and Demographics
Age
- Leiomyoma commonly affects individuals between menarche and menopause.
- The incidence increases with age during reproductive years.[11]
Race
- Leiomyoma usually affects African-American women.[11]
- Incidence rates are approximately threefold greater in African-American women than in white women.
Risk Factors
- Common risk factors in the development of uterine leiomyoma include:
Natural History, Complications and Prognosis
- The majority of patients with uterine leiomyoma remain asymptomatic for a long time; they are usually found incidentally on imaging or examined after patients start having symptoms.
- Studies have shown that 7 to 40% of premenopausal patients with leiomyoma may witness regression of fibroids over 6 months to 3 years.[18]
- At menopause most fibroids will start to shrink as menstrual cycles stop and hormone levels wane.[18]
- Common complications of uterine leiomyoma include:[19]
- Dysmenorrhea
- Dyspareunia
- Leiomyoma degeneration or torsion
- Transcervical prolapse
- Miscarriage
Diagnosis
Diagnostic Study of Choice
- The diagnosis of uterine leiomyoma is based on a clinical diagnosis, which includes a pelvic exam and pelvic ultrasound finding of leiomyomas.
- A pelvic ultrasound is indicated when patients suffer from symtoms of leiomyoma.
- A biopsy is usually not needed to make the diagnosis, but should be performed if clinician is suspicious that the mass is not a fibroid.[20]
Symptoms
- The majority of patients with leiomyoma are usually asymptomatic.
- Symptoms of uterine leiomyoma may include the following:[21]
- Abnormal uterine bleeding
- Heavy or painful periods
- Abdominal discomfort or bloating
- Back ache
- Urinary frequency or retention
- Infertility
Physical Examination
- Common physical examination findings of uterine leiomyoma include enlarged, mobile uterus with an irregular contour on bimanual pelvic examination.[21]
Imaging Findings
- Pelvic ultrasound is helpful in the diagnosis of uterine leiomyoma.
- Findings on an ultrasound diagnostic of uterine leiomyoma include fibroids as focal masses with a heterogeneous texture, which usually cause shadowing of the ultrasound beam.[22]
Other Diagnostic Studies
- Uterine leiomyoma may also be diagnosed using diagnostic hysteroscopy, magnetic resonance imaging, and hysterosalpingography.




Patient #1: MR images demonstrate large degenerating leiomyomas





Patient #2: MR images demonstrate a leiomyoma prolapsing into the endometrial canal


Hysterosalpingogram(HSG) reveals a submucosal leiomyoma


Treatment
Medical Therapy
- The mainstay of therapy for uterine leiomyoma is oral contraceptive pills, either combination pills or progestin-only, Gonadotropin-releasing hormone analogs.
Surgery
- Surgery is the mainstay of therapy for uterine leiomyoma.
- Uterine artery embolization in conjunction with laparotomic myomectomy is the most common approach to the treatment of leiomyoma.
- Hysteroscopic myomectomy can also be performed for patients with uterine leiomyoma.
References
- ↑ Bozini, Nilo; Baracat, Edmund C (2007). "The history of myomectomy at the Medical School of University of São Paulo". Clinics. 62 (3). doi:10.1590/S1807-59322007000300002. ISSN 1807-5932.
- ↑ Munro MG, Critchley HO, Fraser IS, FIGO Menstrual Disorders Working Group (2011). "The FIGO classification of causes of abnormal uterine bleeding in the reproductive years". Fertil Steril. 95 (7): 2204–8, 2208.e1–3. doi:10.1016/j.fertnstert.2011.03.079. PMID 21496802.
- ↑ Hashimoto K, Azuma C, Kamiura S, Kimura T, Nobunaga T, Kanai T; et al. (1995). "Clonal determination of uterine leiomyomas by analyzing differential inactivation of the X-chromosome-linked phosphoglycerokinase gene". Gynecol Obstet Invest. 40 (3): 204–8. doi:10.1159/000292336. PMID 8529956.
- ↑ Mashal RD, Fejzo ML, Friedman AJ, Mitchner N, Nowak RA, Rein MS; et al. (1994). "Analysis of androgen receptor DNA reveals the independent clonal origins of uterine leiomyomata and the secondary nature of cytogenetic aberrations in the development of leiomyomata". Genes Chromosomes Cancer. 11 (1): 1–6. PMID 7529041.
- ↑ 5.0 5.1 Genetics of Uterine Leiomyomas. glowm (2016). http://www.glowm.com/section_view/heading/Genetics%20of%20Uterine%20Leiomyomas/item/363 Accessed on April 19, 2016
- ↑ 6.0 6.1 Zhu X, Fei J, Zhang W, Zhou J (2015). "Uterine leiomyoma mimicking a gastrointestinal stromal tumor with chronic spontaneous hemorrhage: A case report". Oncol Lett. 9 (6): 2481–2484. doi:10.3892/ol.2015.3083. PMC 4473300. PMID 26137094.
- ↑ Parker JD, Leondires M, Sinaii N, Premkumar A, Nieman LK, Stratton P (2006). "Persistence of dysmenorrhea and nonmenstrual pain after optimal endometriosis surgery may indicate adenomyosis". Fertil Steril. 86 (3): 711–5. doi:10.1016/j.fertnstert.2006.01.030. PMID 16782099.
- ↑ Donnez J, Donnez O, Matule D, Ahrendt HJ, Hudecek R, Zatik J; et al. (2016). "Long-term medical management of uterine fibroids with ulipristal acetate". Fertil Steril. 105 (1): 165–173.e4. doi:10.1016/j.fertnstert.2015.09.032. PMID 26477496.
- ↑ Ross J, Judlin P, Jensen J, International Union against sexually transmitted infections (2014). "2012 European guideline for the management of pelvic inflammatory disease". Int J STD AIDS. 25 (1): 1–7. doi:10.1177/0956462413498714. PMID 24216035.
- ↑ Rozenblit AM, Ricci ZJ, Tuvia J, Amis ES (2001). "Incompetent and dilated ovarian veins: a common CT finding in asymptomatic parous women". AJR Am J Roentgenol. 176 (1): 119–22. doi:10.2214/ajr.176.1.1760119. PMID 11133549.
- ↑ 11.0 11.1 11.2 Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM (2003). "High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence". Am J Obstet Gynecol. 188 (1): 100–7. PMID 12548202.
- ↑ Dragomir AD, Schroeder JC, Connolly A, Kupper LL, Hill MC, Olshan AF; et al. (2010). "Potential risk factors associated with subtypes of uterine leiomyomata". Reprod Sci. 17 (11): 1029–35. doi:10.1177/1933719110376979. PMID 20693498.
- ↑ Baird DD, Newbold R (2005). "Prenatal diethylstilbestrol (DES) exposure is associated with uterine leiomyoma development". Reprod Toxicol. 20 (1): 81–4. doi:10.1016/j.reprotox.2005.01.002. PMID 15808789.
- ↑ Marshall LM, Spiegelman D, Goldman MB, Manson JE, Colditz GA, Barbieri RL; et al. (1998). "A prospective study of reproductive factors and oral contraceptive use in relation to the risk of uterine leiomyomata". Fertil Steril. 70 (3): 432–9. PMID 9757871.
- ↑ Sato F, Nishi M, Kudo R, Miyake H (1998). "Body fat distribution and uterine leiomyomas". J Epidemiol. 8 (3): 176–80. PMID 9782674.
- ↑ Chiaffarino F, Parazzini F, La Vecchia C, Chatenoud L, Di Cintio E, Marsico S (1999). "Diet and uterine myomas". Obstet Gynecol. 94 (3): 395–8. PMID 10472866.
- ↑ Wise LA, Palmer JR, Harlow BL, Spiegelman D, Stewart EA, Adams-Campbell LL; et al. (2004). "Risk of uterine leiomyomata in relation to tobacco, alcohol and caffeine consumption in the Black Women's Health Study". Hum Reprod. 19 (8): 1746–54. doi:10.1093/humrep/deh309. PMC 1876785. PMID 15218005.
- ↑ 18.0 18.1 DeWaay DJ, Syrop CH, Nygaard IE, Davis WA, Van Voorhis BJ (2002). "Natural history of uterine polyps and leiomyomata". Obstet Gynecol. 100 (1): 3–7. PMID 12100797.
- ↑ Gupta, Sahana; Manyonda, Isaac T. (2009). "Acute complications of fibroids". Best Practice & Research Clinical Obstetrics & Gynaecology. 23 (5): 609–617. doi:10.1016/j.bpobgyn.2009.01.012. ISSN 1521-6934.
- ↑ Buttram VC, Reiter RC (1981). "Uterine leiomyomata: etiology, symptomatology, and management". Fertil Steril. 36 (4): 433–45. PMID 7026295.
- ↑ 21.0 21.1 Buttram VC, Reiter RC (1981). "Uterine leiomyomata: etiology, symptomatology, and management". Fertil Steril. 36 (4): 433–45. PMID 7026295.
- ↑ Wilde S, Scott-Barrett S (2009). "Radiological appearances of uterine fibroids". Indian J Radiol Imaging. 19 (3): 222–31. doi:10.4103/0971-3026.54887. PMC 2766886. PMID 19881092.