Bile duct cyst: Difference between revisions
No edit summary |
|||
| Line 106: | Line 106: | ||
Future complications include [[cholangitis]] and a 2% risk of malignancy, which may develop in any part of the biliary tree. | Future complications include [[cholangitis]] and a 2% risk of malignancy, which may develop in any part of the biliary tree. | ||
==Diagnosis== | ==Diagnosis== | ||
==History and Symptoms== | ===History and Symptoms=== | ||
Most of them present in 1st year of life; adult presentation is rare and usually at this stage is associated with complication. | Most of them present in 1st year of life; adult presentation is rare and usually at this stage is associated with complication. | ||
| Line 125: | Line 125: | ||
* ERCP is particularly useful for type III choledochoceles, demonstrating a clubbed distal [[common bile duct]] (CBD) and a round, cyst-like, contrast-filled structure in the terminal CBD often extending into the duodenal lumen. | * ERCP is particularly useful for type III choledochoceles, demonstrating a clubbed distal [[common bile duct]] (CBD) and a round, cyst-like, contrast-filled structure in the terminal CBD often extending into the duodenal lumen. | ||
* Magnetic resonance cholangiopancreatography (MRCP) is also a available for evaluation. | * Magnetic resonance cholangiopancreatography (MRCP) is also a available for evaluation. | ||
==Treatment== | ==Treatment== | ||
Biliary duct cysts are treated by surgical excision of the cyst with the formation of a [[roux-en-Y]] anastamosis to the [[biliary duct]]. | Biliary duct cysts are treated by surgical excision of the cyst with the formation of a [[roux-en-Y]] anastamosis to the [[biliary duct]]. | ||
Revision as of 20:35, 27 July 2012
| Bile duct cyst | |
 | |
|---|---|
| MRCP: Type 4 bile duct cyst. Image courtesy of RadsWiki |
|
WikiDoc Resources for Bile duct cyst |
|
Articles |
|---|
|
Most recent articles on Bile duct cyst Most cited articles on Bile duct cyst |
|
Media |
|
Powerpoint slides on Bile duct cyst |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Bile duct cyst at Clinical Trials.gov Trial results on Bile duct cyst Clinical Trials on Bile duct cyst at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Bile duct cyst NICE Guidance on Bile duct cyst
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Bile duct cyst Discussion groups on Bile duct cyst Patient Handouts on Bile duct cyst Directions to Hospitals Treating Bile duct cyst Risk calculators and risk factors for Bile duct cyst
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Bile duct cyst |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [3] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Synonyms and Related Keywords: Choledochal cysts
Overview
Bile duct cysts are congenital conditions associated with benign cystic dilatation of bile ducts. They are uncommon in western countries[1] [2] but not as rare in East Asian nations like Japan and China.
Historical Perspective
Vachel and Stevens were the first to describe a case of cystic dilatation of the intrahepatic bile ducts in 1906, but Jacques Caroli in 1958 gave a more thorough description of a syndrome of congenital malformation of the intrahepatic ducts with segmental cystic dilatation, increased biliary lithiasis, cholangitis and liver abscesses, associated with renal cystic disease or tubular ectasia. The disease is uncommon, with about 180 cases reported in the literature.
Classification
According to the Todani system, there are five types of bile duct cysts.[3]. This classification was based on site of the cyst or dilatation. Type I to IV has been subtyped.

Type 1: Choledochal Cyst
Choledochal cysts are cystic dilatation of the common bile duct (CBD). Most common variety involving saccular or fusiform dilatation of a portion or entire common bile duct (CBD) with normal intrahepatic duct.
- Account for 80% to 90% of all bile duct cysts
- Often presents during infancy with significant liver disease.
- Characterized by fusiform dilation of the extrahepatic bile duct
- Theorized that choledochal cysts form as the result of reflux of pancreatic secretions into the bile duct via anomalous pancreaticobiliary junction.
- Cyst should be resected completely to prevent associated complications (i.e. ascending cholangitis and malignant transformation).
Type 2: Diverticulum
Isolated diverticulum protruding from the CBD.
- Accounts for 3% of all bile duct cysts
- Represents a true diverticulum.
- Saccular outpouchings arising from the supraduodenal extrahepatic bile duct or the intrahepatic bile ducts.
Type 3: Choledochocele[4]
Arise from dilatation of duodenal portion of CBD or where pancreatic duct meets.
- Accounts for 5% of all bile duct cysts
- Represents protrusion of a focally dilated, intramural segment of the distal common bile duct into the duodenum.
- Choledochoceles may be successfully managed with endoscopic sphincterotomy, surgical excision, or both, in symptomatic patients.
- Often present with pain and obstructive jaundice; many have pancreatitis.
Type 4: Multiple Communicating Intra and Extrahepatic Duct Cysts
Dilatation of both intrahepatic and extrahepatic biliary duct.
- Second most common type of bile duct cysts (10%)
- Subdivided into subtypes A and B.
- Type 4A: Fusiform dilation of the entire extrahepatic bile duct with extension of dilation of the intrahepatic bile ducts
- Type 4B: Multiple cystic dilations involving only the extrahepatic bile duct.
-
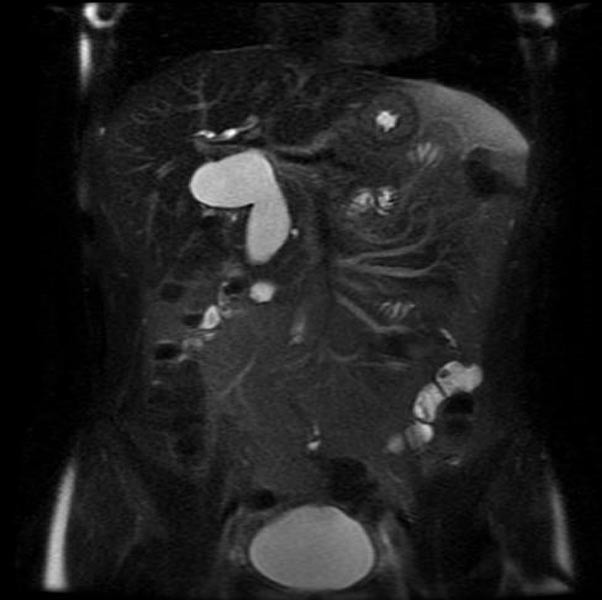
MRI - T2: Type 4 bile duct cyst
-
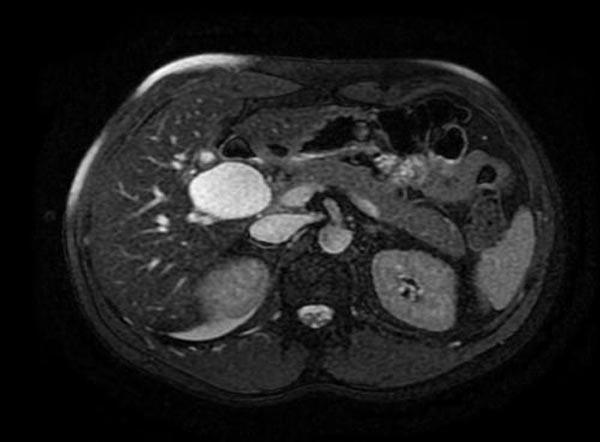
MRI - T2: Type 4 bile duct cyst
-

MRI - T2: Type 4 bile duct cyst
-
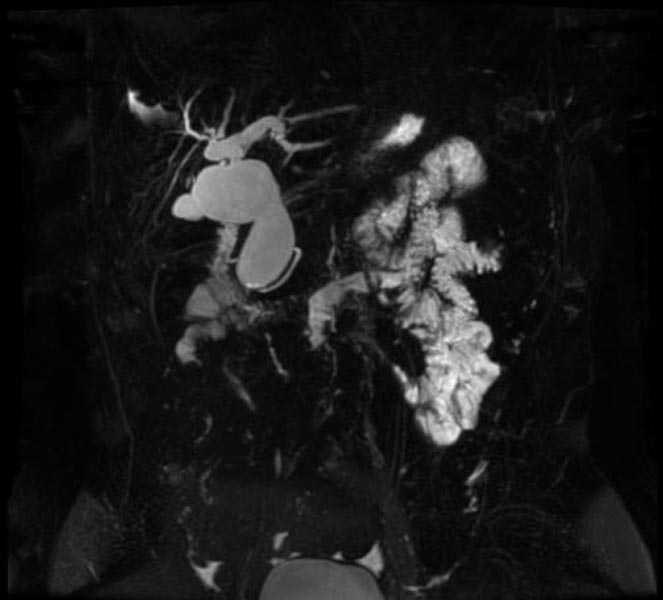
MRCP: Type 4 bile duct cyst



Type 5: Caroli's Disease
Cystic dilatation of intra hepatic biliary ducts. [4] [5] [6] [7] [8] [9] [10]
- Caroli's disease is a rare form of congenital biliary cystic disease manifested by cystic dilations of intrahepatic bile ducts
- Association with benign renal tubular ectasia and other forms of renal cystic disease.
Pathophysiology
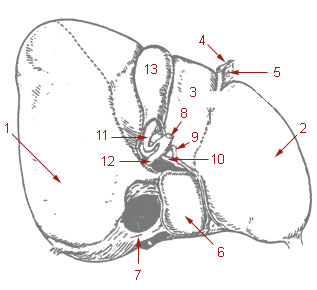
Bile Duct Anatomy
The path is as follows: Bile canaliculi → Canals of Hering → interlobular bile ducts → intrahepatic bile ducts → left and right hepatic ducts merge to form → common hepatic duct exits liver and joins → cystic duct (from gall bladder) forming → common bile duct → joins with pancreatic duct → forming ampulla of Vater → enters duodenum
-
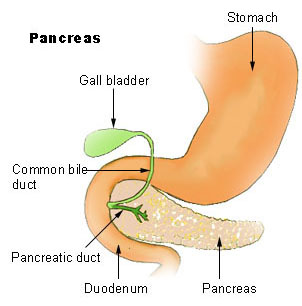
Region of pancreas
-
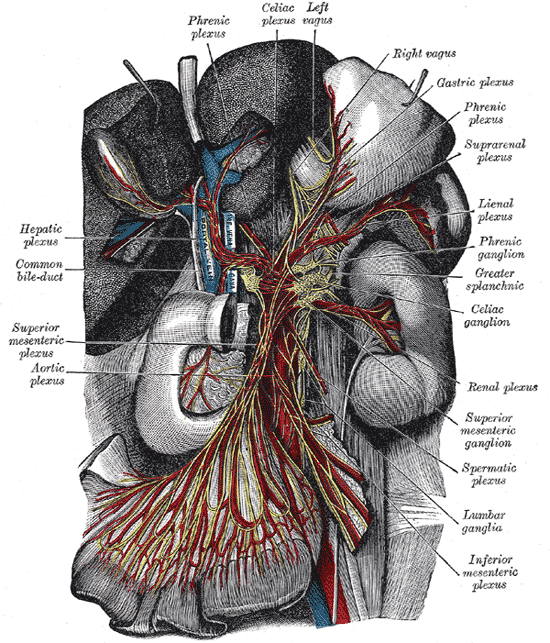
The celiac ganglia with the sympathetic plexuses of the abdominal viscera radiating from the ganglia.
-
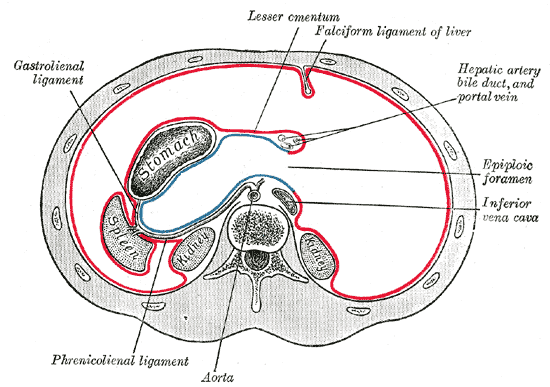
Horizontal disposition of the peritoneum in the upper part of the abdomen.
-
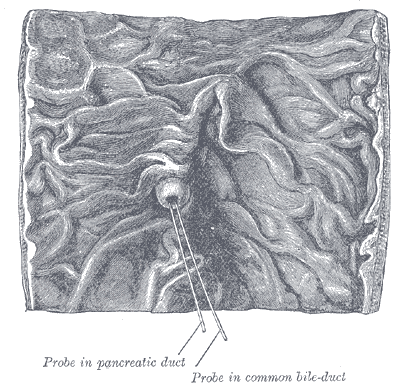
Interior of the descending portion of the duodenum, showing bile papilla.
-
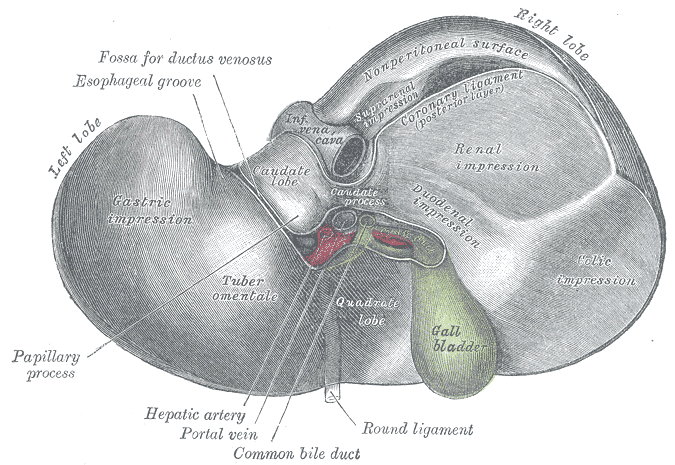
Inferior surface of the liver.
-
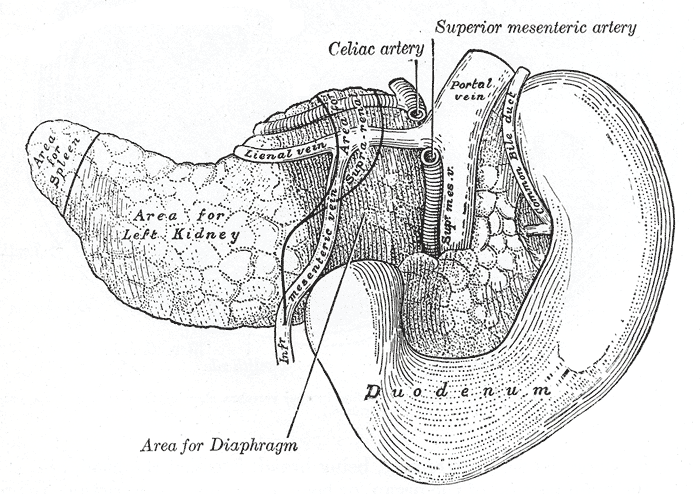
The pancreas and duodenum from behind.
-
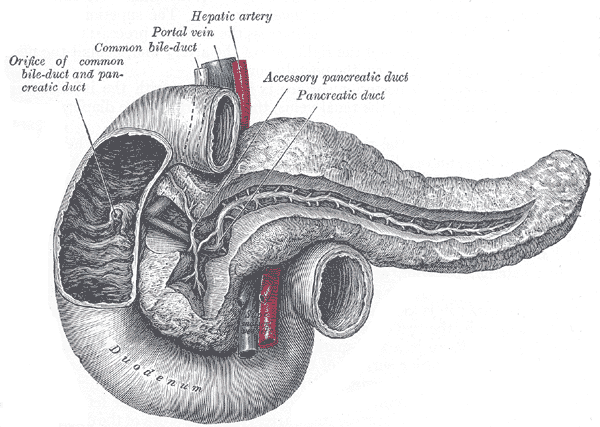
The pancreatic duct.
-
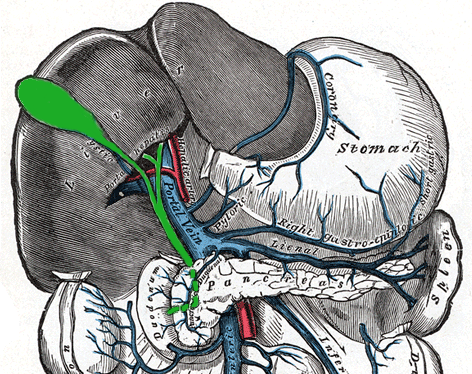
The portal vein and its tributaries.
-
Liver and gallbladder









Causes
Many biliary cysts are congenitally acquired, perhaps as a consequence of unequal proliferation of epithelial cells during embryonic biliary duct development. Some biliary cysts are acquired, and some may develop in association with anatomic variations that lead to abnormally high ductal pressures in association with other predisposing factors.
Natural history, Complications and Prognosis
Future complications include cholangitis and a 2% risk of malignancy, which may develop in any part of the biliary tree.
Diagnosis
History and Symptoms
Most of them present in 1st year of life; adult presentation is rare and usually at this stage is associated with complication.
Classic triad (listed below) is found only in minority of patients:
A hepatic cyst may be present, as may short stature. A fever of unknown origin may be observed. Pancreatitis may be present.
MRI and CT
- Abdominal CT scans are also often diagnostic.
Ultrasonography
- Ultrasound is often adequate for the diagnosis of biliary cysts, except for Type III choledochoceles. Biliary cysts can often even be picked up in utero.
Other Imaging Findings
- Cholescintigraphy (HIDA scans) is also quite useful for all but Type III choledochoceles. Findings include biliary tract dilatation and tracer retention after 24 hours. It gives data on excretory function, which is also useful post surgical repair.
- Endoscopic Retrograde Cholangio-Pancreatography (ERCP) provides excellent visualization.
- ERCP is particularly useful for type III choledochoceles, demonstrating a clubbed distal common bile duct (CBD) and a round, cyst-like, contrast-filled structure in the terminal CBD often extending into the duodenal lumen.
- Magnetic resonance cholangiopancreatography (MRCP) is also a available for evaluation.
Treatment
Biliary duct cysts are treated by surgical excision of the cyst with the formation of a roux-en-Y anastamosis to the biliary duct.
- Intrahepatic biliary cyst treatment depends on degree of involvement.
- Segmental disease can be potentially cured with lobectomy. The risks and benefits of undergoing this surgery, versus the associated risks of future cholangitis, stone disease, pancreatitis, and liver abscess if not treated surgically have to be weighed in individual patients.
- If both lobes are involved, surgical resection may not be an option.
- If patients have recurrent cholangitis, a trial of prophylactic antibiotics could be considered.
- Liver transplant is a final option.
- Cholecystectomy is indicated because it reduces the likelihood of cholangitis, and because the gallbladder is at increased risk of malignancy in patients with biliary cysts.
- A report in the Lancet describes a significant improvement in stone disease in Caroli’s disease patients treated with ursodeoxycholic acid (Actigall) 10-20 mg/kg/d.
- Extrahepatic biliary cysts are often treated with surgical repair due to risks of cyst rupture with secondary peritonitis, cholangitis and liver cirrhosis.
- Surgical options include primary cyst excision, and internal drainage procedures, such as choledochoduodenostomy and Roun-en-Y choledochojejunostomy. The down sides of internal drainage include a high complication rate and risk of malignancy in the abnormal region (2.5%).
References
- ↑ Liu YB, Wang JW, Devkota KR; et al. (2007). "Congenital choledochal cysts in adults: twenty-five-year experience". Chin. Med. J. 120 (16): 1404–7. PMID 17825168.
- ↑ Yu, Jinxing, Turner, Mary Ann, Fulcher, Ann S., Halvorsen, Robert A. Congenital Anomalies and Normal Variants of the Pancreaticobiliary Tract and the Pancreas in Adults: Part 1, Biliary Tract. Am. J. Roentgenol. 2006 187: 1536-1543
- ↑ Todani T, Watanabe Y, Narusue M, Tabuchi K, Okajima K (1977). "Congenital bile duct cysts: Classification, operative procedures, and review of thirty-seven cases including cancer arising from choledochal cyst". Am. J. Surg. 134 (2): 263–9. PMID 889044.
- ↑ Caroli, J, et al. La dilatation polykystique congenitale des voies biliaires intrahepatiques. Essai del classification. Sem Hop Paris 1958;34:488
- ↑ Lu, S.C. et al. Diseases of the biliary tree. Textbook of Gastroenterology 1995:2212.
- ↑ Tandon, RK, et al. Caroli’s disease: A heterogeneous entity. Amer J Gastroent 1990;85:170. PMID 2301339
- ↑ Chalasani, N, et al. Spontaneous rupture of a bile duct. Amer J Gastroent 1997;92:1062. PMID 9177539
- ↑ Miller, WJ, et al. Imaging findings in Caroli’s disease. Am J Roenth 1995;165:333. PMID 7618550
- ↑ Torra, R, et al. Autosomal dominant polycystic kidney disease and Caroli’s disease. Kidney Int 1997;52:33. PMID 9211343
- ↑ Ros, E, et al. Ursodeoxycholic acid treatment of primary hepatolithiasis in Caroli’s syndrome. Lancet 1993;342:404. PMID 8101905