Multiple sclerosis pathophysiology
| https://https://www.youtube.com/watch?v=yzH8ul5PSZ8 |350}} |
|
Multiple sclerosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Multiple sclerosis pathophysiology On the Web |
|
American Roentgen Ray Society Images of Multiple sclerosis pathophysiology |
|
Risk calculators and risk factors for Multiple sclerosis pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Pathophysiology
Although much is known about how multiple sclerosis causes damage, the reasons why multiple sclerosis occurs are not known. Multiple sclerosis is a disease in which the myelin (a fatty substance which covers the axons of nerve cells) degenerates. According to the view of most researchers, a special subset of lymphocytes, called T cells, plays a key role in the development of MS.
According to a strictly immunological explanation of MS, the inflammatory process is triggered by the T cells. T cells gain entry into the brain via the blood-brain barrier (a capillary system that should prevent entrance of T-cells into the nervous system). The blood brain barrier is normally not permeable to these types of cells, unless triggered by either infection or a virus, where the integrity of the tight junctions forming the blood-brain barrier is decreased. When the blood brain barrier regains its integrity (usually after infection or virus has cleared) the T cells are trapped inside the brain. These lymphocytes recognize myelin as foreign and attack it as if it were an invading virus. That triggers inflammatory processes, stimulating other immune cells and soluble factors like cytokines and antibodies. Leaks form in the blood-brain barrier. These leaks, in turn, cause a number of other damaging effects such as swelling, activation of macrophages, and more activation of cytokines and other destructive proteins such as matrix metalloproteinases. A deficiency of uric acid has been implicated in this process.[1]
It is known that a repair process, called remyelination, takes place in early phases of the disease, but the oligodendrocytes that originally formed a myelin sheath cannot completely rebuild a destroyed myelin sheath. The newly-formed myelin sheaths are thinner and often not as effective as the original ones. Repeated attacks lead to successively fewer effective remyelinations, until a scar-like plaque is built up around the damaged axons, according to four different damage patterns.[2] The central nervous system should be able to recruit oligodendrocyte stem cells capable of turning into mature myelinating oligodendrocytes, but it is suspected that something inhibits stem cells in affected areas.
The axons themselves can also be damaged by the attacks.[3] Often, the brain is able to compensate for some of this damage, due to an ability called neuroplasticity. MS symptoms develop as the cumulative result of multiple lesions in the brain and spinal cord. This is why symptoms can vary greatly between different individuals, depending on where their lesions occur.
-
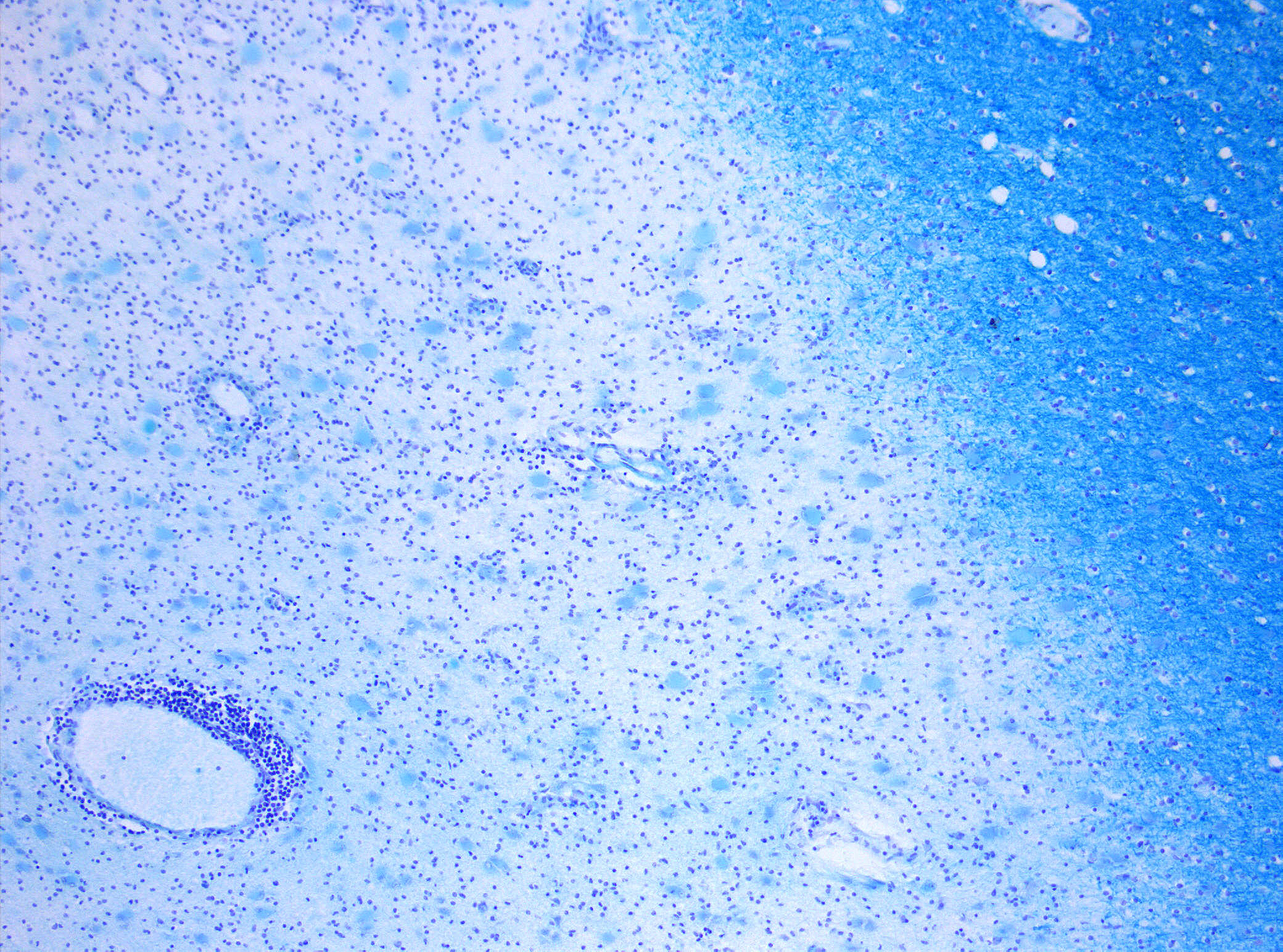
Demyelinization in MS. On Klüver-Barrera myelin staining, decoloration in the area of the lesion can be appreciated (Original scale 1:100)
-
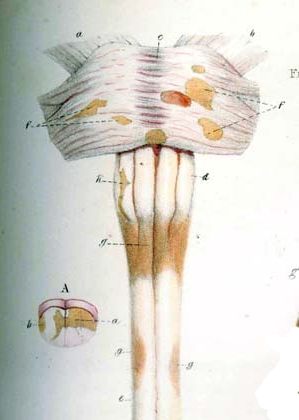
Detail of drawing from Carswell book depicting multiple sclerosis lesions in the brain stemand spinal cord (1838)


References
- ↑ Rentzos M, Nikolaou C, Anagnostouli M, Rombos A, Tsakanikas K, Economou M, Dimitrakopoulos A, Karouli M, Vassilopoulos D (2006). "Serum uric acid and multiple sclerosis". Clinical neurology and neurosurgery. 108 (6): 527–31. PMID 16202511.
- ↑ Lucchinetti, C. Bruck, W. Parisi, J. Scherhauer, B. Rodriguez, M. Lassmann, H.Heterogeneity of multiple sclerosis lesions: implications for the pathogenesis of demyelination Ann Neurol, 2000; 47(6):707-17. PMID 10852536
- ↑ Pascual AM, Martínez-Bisbal MC, Boscá I; et al. (2007). "Axonal loss is progressive and partly dissociated from lesion load in early multiple sclerosis". Neurology. 69 (1): 63–7. doi:10.1212/01.wnl.0000265054.08610.12. PMID 17606882.