[Disease name] was first discovered by [name of scientist], a [nationality + occupation], in [year]/during/following [event].
The association between [important risk factor/cause] and [disease name] was made in/during [year/event].
In [year], [scientist] was the first to discover the association between [risk factor] and the development of [disease name].
In [year], [gene] mutations were first implicated in the pathogenesis of [disease name].
There have been several outbreaks of [disease name], including -----.
In [year], [diagnostic test/therapy] was developed by [scientist] to treat/diagnose [disease name].
==Classification==
There is no established system for the classification of [disease name].
OR
[Disease name] may be classified according to [classification method] into [number] subtypes/groups: [group1], [group2], [group3], and [group4].
OR
[Disease name] may be classified into [large number > 6] subtypes based on [classification method 1], [classification method 2], and [classification method 3].
[Disease name] may be classified into several subtypes based on [classification method 1], [classification method 2], and [classification method 3].
OR
Based on the duration of symptoms, [disease name] may be classified as either acute or chronic.
OR
If the staging system involves specific and characteristic findings and features:
According to the [staging system + reference], there are [number] stages of [malignancy name] based on the [finding1], [finding2], and [finding3]. Each stage is assigned a [letter/number1] and a [letter/number2] that designate the [feature1] and [feature2].
OR
The staging of [malignancy name] is based on the [staging system].
OR
There is no established system for the staging of [malignancy name].
==Pathophysiology==
The exact pathogenesis of [disease name] is not fully understood.
OR
It is thought that [disease name] is the result of / is mediated by / is produced by / is caused by either [hypothesis 1], [hypothesis 2], or [hypothesis 3].
OR
[Pathogen name] is usually transmitted via the [transmission route] route to the human host.
OR
Following transmission/ingestion, the [pathogen] uses the [entry site] to invade the [cell name] cell.
OR
[Disease or malignancy name] arises from [cell name]s, which are [cell type] cells that are normally involved in [function of cells].
OR
The progression to [disease name] usually involves the [molecular pathway].
OR
The pathophysiology of [disease/malignancy] depends on the histological subtype.
==Causes==
Disease name] may be caused by [cause1], [cause2], or [cause3].
OR
Common causes of [disease] include [cause1], [cause2], and [cause3].
OR
The most common cause of [disease name] is [cause 1]. Less common causes of [disease name] include [cause 2], [cause 3], and [cause 4].
OR
The cause of [disease name] has not been identified. To review risk factors for the development of [disease name], click [[Pericarditis causes#Overview|here]].
==Differentiating ((Page name)) from Other Diseases==
[Disease name] must be differentiated from other diseases that cause [clinical feature 1], [clinical feature 2], and [clinical feature 3], such as [differential dx1], [differential dx2], and [differential dx3].
OR
[Disease name] must be differentiated from [[differential dx1], [differential dx2], and [differential dx3].
==Epidemiology and Demographics==
The incidence/prevalence of [disease name] is approximately [number range] per 100,000 individuals worldwide.
OR
In [year], the incidence/prevalence of [disease name] was estimated to be [number range] cases per 100,000 individuals worldwide.
OR
In [year], the incidence of [disease name] is approximately [number range] per 100,000 individuals with a case-fatality rate of [number range]%.
Patients of all age groups may develop [disease name].
OR
The incidence of [disease name] increases with age; the median age at diagnosis is [#] years.
OR
[Disease name] commonly affects individuals younger than/older than [number of years] years of age.
OR
[Chronic disease name] is usually first diagnosed among [age group].
There is no racial predilection to [disease name].
OR
[Disease name] usually affects individuals of the [race 1] race. [Race 2] individuals are less likely to develop [disease name].
[Disease name] affects men and women equally.
OR
[Gender 1] are more commonly affected by [disease name] than [gender 2]. The [gender 1] to [gender 2] ratio is approximately [number > 1] to 1.
The majority of [disease name] cases are reported in [geographical region].
OR
[Disease name] is a common/rare disease that tends to affect [patient population 1] and [patient population 2].
==Risk Factors==
There are no established risk factors for [disease name].
OR
The most potent risk factor in the development of [disease name] is [risk factor 1]. Other risk factors include [risk factor 2], [risk factor 3], and [risk factor 4].
OR
Common risk factors in the development of [disease name] include [risk factor 1], [risk factor 2], [risk factor 3], and [risk factor 4].
OR
Common risk factors in the development of [disease name] may be occupational, environmental, genetic, and viral.
==Screening==
There is insufficient evidence to recommend routine screening for [disease/malignancy].
OR
According to the [guideline name], screening for [disease name] is not recommended.
OR
According to the [guideline name], screening for [disease name] by [test 1] is recommended every [duration] among patients with [condition 1], [condition 2], and [condition 3].
==Natural History, Complications, and Prognosis==
If left untreated, [#]% of patients with [disease name] may progress to develop [manifestation 1], [manifestation 2], and [manifestation 3].
OR
Common complications of [disease name] include [complication 1], [complication 2], and [complication 3].
OR
Prognosis is generally excellent/good/poor, and the 1/5/10-year mortality/survival rate of patients with [disease name] is approximately [#]%.
==Diagnosis==
===Diagnostic Study of Choice===
The diagnosis of [disease name] is made when at least [number] of the following [number] diagnostic criteria are met: [criterion 1], [criterion 2], [criterion 3], and [criterion 4].
OR
The diagnosis of [disease name] is based on the [criteria name] criteria, which include [criterion 1], [criterion 2], and [criterion 3].
OR
The diagnosis of [disease name] is based on the [definition name] definition, which includes [criterion 1], [criterion 2], and [criterion 3].
OR
There are no established criteria for the diagnosis of [disease name].
===History and Symptoms===
The majority of patients with [disease name] are asymptomatic.
OR
The hallmark of [disease name] is [finding]. A positive history of [finding 1] and [finding 2] is suggestive of [disease name]. The most common symptoms of [disease name] include [symptom 1], [symptom 2], and [symptom 3]. Common symptoms of [disease] include [symptom 1], [symptom 2], and [symptom 3]. Less common symptoms of [disease name] include [symptom 1], [symptom 2], and [symptom 3].
===Physical Examination===
Patients with [disease name] usually appear [general appearance]. Physical examination of patients with [disease name] is usually remarkable for [finding 1], [finding 2], and [finding 3].
OR
Common physical examination findings of [disease name] include [finding 1], [finding 2], and [finding 3].
OR
The presence of [finding(s)] on physical examination is diagnostic of [disease name].
OR
The presence of [finding(s)] on physical examination is highly suggestive of [disease name].
===Laboratory Findings===
An elevated/reduced concentration of serum/blood/urinary/CSF/other [lab test] is diagnostic of [disease name].
OR
Laboratory findings consistent with the diagnosis of [disease name] include [abnormal test 1], [abnormal test 2], and [abnormal test 3].
OR
[Test] is usually normal among patients with [disease name].
OR
Some patients with [disease name] may have elevated/reduced concentration of [test], which is usually suggestive of [progression/complication].
OR
There are no diagnostic laboratory findings associated with [disease name].
===Electrocardiogram===
There are no ECG findings associated with [disease name].
OR
An ECG may be helpful in the diagnosis of [disease name]. Findings on an ECG suggestive of/diagnostic of [disease name] include [finding 1], [finding 2], and [finding 3].
===X-ray===
There are no x-ray findings associated with [disease name].
OR
An x-ray may be helpful in the diagnosis of [disease name]. Findings on an x-ray suggestive of/diagnostic of [disease name] include [finding 1], [finding 2], and [finding 3].
OR
There are no x-ray findings associated with [disease name]. However, an x-ray may be helpful in the diagnosis of complications of [disease name], which include [complication 1], [complication 2], and [complication 3].
===Echocardiography or Ultrasound===
There are no echocardiography/ultrasound findings associated with [disease name].
OR
Echocardiography/ultrasound may be helpful in the diagnosis of [disease name]. Findings on an echocardiography/ultrasound suggestive of/diagnostic of [disease name] include [finding 1], [finding 2], and [finding 3].
OR
There are no echocardiography/ultrasound findings associated with [disease name]. However, an echocardiography/ultrasound may be helpful in the diagnosis of complications of [disease name], which include [complication 1], [complication 2], and [complication 3].
===CT scan===
There are no CT scan findings associated with [disease name].
OR
[Location] CT scan may be helpful in the diagnosis of [disease name]. Findings on CT scan suggestive of/diagnostic of [disease name] include [finding 1], [finding 2], and [finding 3].
OR
There are no CT scan findings associated with [disease name]. However, a CT scan may be helpful in the diagnosis of complications of [disease name], which include [complication 1], [complication 2], and [complication 3].
===MRI===
There are no MRI findings associated with [disease name].
OR
[Location] MRI may be helpful in the diagnosis of [disease name]. Findings on MRI suggestive of/diagnostic of [disease name] include [finding 1], [finding 2], and [finding 3].
OR
There are no MRI findings associated with [disease name]. However, a MRI may be helpful in the diagnosis of complications of [disease name], which include [complication 1], [complication 2], and [complication 3].
===Other Imaging Findings===
There are no other imaging findings associated with [disease name].
OR
[Imaging modality] may be helpful in the diagnosis of [disease name]. Findings on an [imaging modality] suggestive of/diagnostic of [disease name] include [finding 1], [finding 2], and [finding 3].
===Other Diagnostic Studies===
There are no other diagnostic studies associated with [disease name].
OR
[Diagnostic study] may be helpful in the diagnosis of [disease name]. Findings suggestive of/diagnostic of [disease name] include [finding 1], [finding 2], and [finding 3].
OR
Other diagnostic studies for [disease name] include [diagnostic study 1], which demonstrates [finding 1], [finding 2], and [finding 3], and [diagnostic study 2], which demonstrates [finding 1], [finding 2], and [finding 3].
==Treatment==
===Medical Therapy===
There is no treatment for [disease name]; the mainstay of therapy is supportive care.
OR
Supportive therapy for [disease name] includes [therapy 1], [therapy 2], and [therapy 3].
OR
The majority of cases of [disease name] are self-limited and require only supportive care.
OR
[Disease name] is a medical emergency and requires prompt treatment.
OR
The mainstay of treatment for [disease name] is [therapy].
OR
The optimal therapy for [malignancy name] depends on the stage at diagnosis.
OR
[Therapy] is recommended among all patients who develop [disease name].
OR
Pharmacologic medical therapy is recommended among patients with [disease subclass 1], [disease subclass 2], and [disease subclass 3].
OR
Pharmacologic medical therapies for [disease name] include (either) [therapy 1], [therapy 2], and/or [therapy 3].
OR
Empiric therapy for [disease name] depends on [disease factor 1] and [disease factor 2].
OR
Patients with [disease subclass 1] are treated with [therapy 1], whereas patients with [disease subclass 2] are treated with [therapy 2].
===Surgery===
Surgical intervention is not recommended for the management of [disease name].
OR
Surgery is not the first-line treatment option for patients with [disease name]. Surgery is usually reserved for patients with either [indication 1], [indication 2], and [indication 3]
OR
The mainstay of treatment for [disease name] is medical therapy. Surgery is usually reserved for patients with either [indication 1], [indication 2], and/or [indication 3].
OR
The feasibility of surgery depends on the stage of [malignancy] at diagnosis.
OR
Surgery is the mainstay of treatment for [disease or malignancy].
===Primary Prevention===
There are no established measures for the primary prevention of [disease name].
OR
There are no available vaccines against [disease name].
OR
Effective measures for the primary prevention of [disease name] include [measure1], [measure2], and [measure3].
OR
[Vaccine name] vaccine is recommended for [patient population] to prevent [disease name]. Other primary prevention strategies include [strategy 1], [strategy 2], and [strategy 3].
===Secondary Prevention===
There are no established measures for the secondary prevention of [disease name].
OR
Effective measures for the secondary prevention of [disease name] include [strategy 1], [strategy 2], and [strategy 3].
Uterine leiomyoma was first discovered by Hippocrates in 460-375 B.C and called it “uterine stone”. Uterine leiomyoma may be classified according to their location into 3 subtypes: submucosal, subserous, and intramural. The pathogenesis of leiomyoma is characterized by benignsmooth muscleneoplasm. They can occur in any organ, but the most common forms occur in the uterus, small bowel and the esophagus. Chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q has been associated with the development of leiomyoma. Uterine leiomyoma must be differentiated from other diseases that cause uterine mass, such as: uterine adenomyoma, pregnancy, hematometra, uterine sarcoma, uterine carcinosarcoma, and metastasis. Leiomyoma is more commonly observed among patients aged 40 years and older. Common risk factors in the development of uterine leiomyoma include African-American race, early menarche, prenatal exposure to diethylstilbestrol, having one or more pregnancies extending beyond 20 weeks, obesity, significant consumption of beef and other reds meats, hypertension, family history, and alcohol consumption. Physical examination may be remarkable for enlarged, mobile uterus with an irregular contour on bimanual pelvic examination. The mainstay of therapy for uterine leiomyoma is oral contraceptive pills, either combination pills or progestin-only, Gonadotropin-releasing hormone analogs. Surgery is also part of mainstay therapy for uterine leiomyoma.
Historical Perspective
Uterine leiomyoma was first discovered by Hippocrates in 460-375 B.C and called it “uterine stone”.
In the second century AD, Galen described the lesion as "scleromas".[1]
In 1860 and 1863, Rokitansky and Klob coined the term fibroid.
In 1854, Virchow, a German pathologist demonstrated that those tumors originated from the uterine smooth muscle. Thus, the term "myoma" became current in clinical use.
In 1809, the first laparotomy consequent to myoma indication was conducted by Ephraim McDowell to treat leiomyoma in Danville, USA.
The first successful myomectomy was performed by Amussat in 1840, after a clinical diagnosis of ovarian tumor because pelvic examination showed a pediculate and large uterine leiomyoma.
The first scientific report of a uterus conserving myomectomy through the vagina appeared in 1845 in the American Journal of Medical Science, accomplished by Washington Atlee, in Pennsylvania.
In 1898, Alexander Adam presented 11 cases of myomectomy through an abdominal route, in Liverpool.
In 1940, Carlos R. Círio proposed a technique of the myometrium emptying, called myometrectomy.
Classification
Uterine leiomyoma may be classified into 3 subtypes according to location:
The chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q have been associated with the development of leiomyoma.[2]
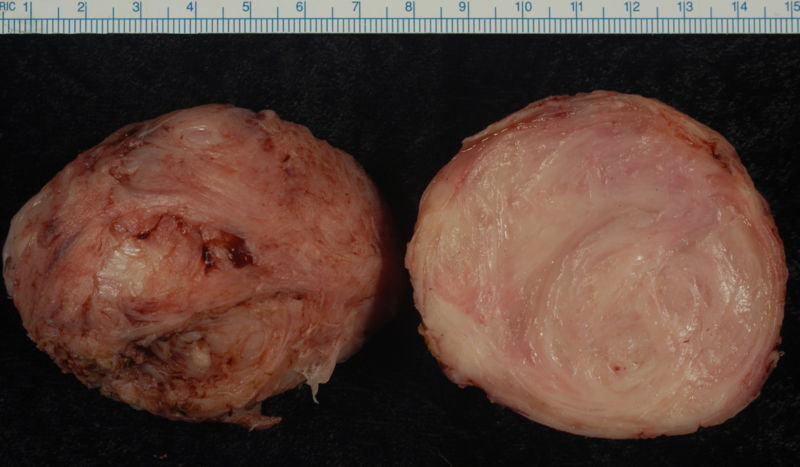
On gross pathology, round, well circumscribed (but not encapsulated), solid nodules that are white or tan, and whorled are characteristic findings of leiomyoma .
On microscopic histopathological analysis, elongated, spindle-shaped cells with a cigar-shaped nucleus are characteristic findings of leiomyoma.
Uterine Leiomyomata
Uterine fibroids are leiomyomata of the uterine smooth muscle. As with other leiomyomata, they are benign, but may lead to excessive menstrual bleeding (menorrhagia), often cause anemia and may lead to infertility. Enucleation is removal of fibroids without removing the uterus (hysterectomy), which is also commonly performed. Laser surgery (called myolysis) is increasingly used, and provides a viable alternative to surgery. Estrogen and progesterone usually stimulate their growth, and hormone suppression may hence decrease their size.
Esophageal
Leiomyoma of the esophagus is the most common benignesophagealtumour, though this accounts for less than 1% of esophageal neoplasms. The remainder consists mainly of carcinomas. Although the vast majority of benign esophageal tumors are clinically silent and go undetected, large or strategically located tumors may become symptomatic. [3]
Leiomyoma of Jejunum
Leiomyoma is the most common benign tumor of small bowel. Approximately 50% of cases are found in the jejunum, followed by the ileum in 31% of cases. Almost one half of all lesions are less than 5 centimeters. [4]
Leiomyoma enucleated from a uterus. External surface on left; cut surface on right
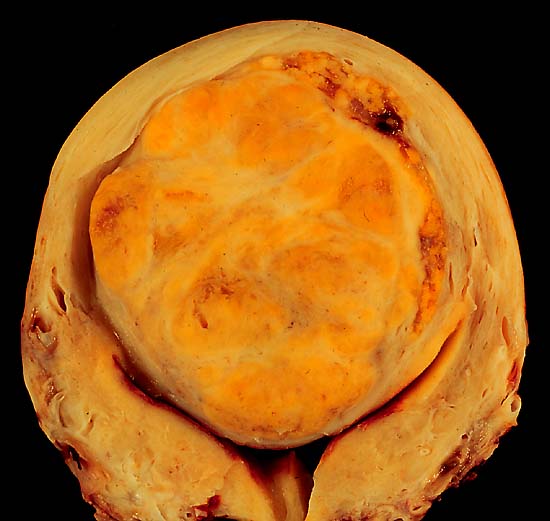
A large, solitary leiomyoma in the uterus, distoring the endometrial cavity into a Y shape by splaying and pressing it downwards. (Image courtesy of Ed Uthman, MD)
Causes
Chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q have been associated with the development of leiomyoma.
Differentiating Leiomyoma from other Diseases
Leiomyoma is a cause of abnormal uterine bleeding and can result in infertility. There are several diseases which can result in excessive uterine bleeding and the following table is a description of various causes of excessive uterine bleeding.
Enlarged, mobile uterus with an irregular contour on bimanual pelvic examination
Imaging Findings
On ultrasound imaging, uterine leiomyoma is characterized by the fibroids as focal masses with a heterogeneous texture, which usually cause shadowing of the ultrasound beam.
Patient #1: MR images demonstrate large degenerating leiomyomas
Patient #2: MR images demonstrate a leiomyoma prolapsing into the endometrial canal
Hysterosalpingogram(HSG) reveals a submucosal leiomyoma
Treatment
Medical Therapy
The mainstay of therapy for uterine leiomyoma is oral contraceptive pills, either combination pills or progestin-only, Gonadotropin-releasing hormone analogs.
Surgery
Surgery is the mainstay of therapy for uterine leiomyoma.
↑James C. Chou, MD & Frank G. Gress, MD. "Benign Esophageal Tumors". Esophageal Cancer Overview (Cancer of the Esophagus). Retrieved 2007-03-21. Unknown parameter |publsiher= ignored (|publisher= suggested) (help)CS1 maint: Multiple names: authors list (link)
↑By Michael P. Buetow, M.D. "Leiomyoma of Jejunum". Retrieved 2007-03-21. Unknown parameter |publsiher= ignored (|publisher= suggested) (help)