Bronchiectasis pathophysiology: Difference between revisions
No edit summary |
m (Bot: Removing from Primary care) |
||
| (34 intermediate revisions by 6 users not shown) | |||
| Line 1: | Line 1: | ||
__NOTOC__ | __NOTOC__ | ||
{{Bronchiectasis}} | {{Bronchiectasis}} | ||
{{CMG}} | {{CMG}}; {{AE}} {{HQ}}, Saarah T. Alkhairy, M.D. | ||
==Overview== | ==Overview== | ||
Bronchiectasis involves | Bronchiectasis involves cycles of [[Infection|infections]] and [[inflammation]] that result in [[Alveolus|alveolar]] damage and inelastic dilated [[Bronchus|bronchi]]. Damage to the airway results in airflow obstruction and impaired clearance of [[secretions]]. | ||
==Pathophysiology== | ==Pathophysiology== | ||
The following events summarize the pathophysiology of bronchiectasis:<ref>{{cite journal |author=Morrissey BM |title=Pathogenesis of bronchiectasis |language=English |journal=Clin Chest Med|volume=28 |issue=2 |pages=289-96 |year=2007 |pmid=17467548 |doi=}}</ref> | |||
*[[Dilation]] of the [[bronchial]] walls results in airflow obstruction and impaired clearance of secretions. | |||
*The dilated areas interrupt normal air pressure of the [[bronchial]] tubes, causing [[sputum]] to pool inside the dilated areas instead of being pushed upward. | |||
*The sputum contains [[elastase]], [[interleukin-8]], [[tumor necrosis factor alpha]] ([[Tumor necrosis factor-alpha|TNF-a]]), and [[Prostanoid|prostanoids]]. | |||
*The pooled [[sputum]] provides an environment favorable to the growth of infectious [[pathogen|pathogens]]. | |||
*Recurrent [[Infection|infections]] are followed [[inflammation]] and infiltration of [[Neutrophil|neutrophils]], [[Macrophage|macrophages]], and [[T cell|T-lymphocytes]]. | |||
*The more [[infections|infection]] that the [[Lung|lungs]] experience, leads to the sustained inflammation, consequently, damage to the [[alveoli]] in the [[lung|lungs]]. | |||
*With more injury to the [[lung]] tissue, the elasticity in the [[bronchial tube]]s is reduced and the tubes are dilated, which creates a perpetual destructive cycle | |||
===Cole's Cycle=== | |||
The following events summarize Cole's cycle (Cole's "vicious cycle hypothesis"), which is the most widely known model of the development of bronchiectasis:<ref name="pmid20037680">{{cite journal| author=King PT| title=The pathophysiology of bronchiectasis. | journal=Int J Chron Obstruct Pulmon Dis | year= 2009 | volume= 4 | issue= | pages= 411-9 | pmid=20037680 | doi= | pmc=PMC2793069 | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=20037680 }} </ref> | |||
*Two factors are required for the development of bronchiectasis: | |||
**Persistent [[infection]] | |||
**Host defense derangement | |||
*Impaired mucociliary clearance due to the genetic susceptibility may cause environmental insult. | |||
*Insults result in persistence of microbes in the sinobronchial tree. | |||
*The microbial [[infection]] can cause chronic [[inflammation]], which may result in tissue damage and impaired [[Mucociliary clearance|mucociliary]] motility. | |||
*[[Inflammation]] ensues more [[infection]], which in turn ensues more [[inflammation]]. | |||
===Immune Response=== | |||
*Bronchiectasis involves the activity of [[reactive oxygen species]] ([[Reactive oxygen species|ROS]]), [[Elastase|elastases]], and [[Matrix metalloproteinase|matrix metalloproteinases]] ([[MMP|MMPs]]): | |||
**[[Reactive oxygen species]] ([[Reactive oxygen species|ROS]]) | |||
***A by product for the metabolism of [[oxygen]] | |||
***Increased concentration may result in cell structure damage | |||
* [[Elastase]] | |||
** [[Protease]] that catalyzes the breaks down of [[elastin]]. | |||
** [[Elastin]] plus [[collagen]] determine the mechanical properties of [[connective tissue]]. | |||
* [[Matrix metalloproteinases]] ([[Matrix metalloproteinase|MMPs]]) | |||
** Responsible for the degradation of the majority of the extracellular proteins during normal tissue turn over. | |||
** [[Inflammation]] may result in epithelial injury and [[mucus]] secretion via increased concentrations of [[Reactive oxygen species|ROS]], [[elastase]] ciliotoxin, and [[mucus]] secretogogues. | |||
** [[Epithelial]] injury and [[mucus]] hypersecretion lead to chronic [[bronchial]] infection, reduced [[mucociliary clearance]], and plugging of the [[airway]] - which all eventually leads to airway damage and bronchiectasis. | |||
The diagram below depicts the immune response for bronchiectasis: | |||
<gallery widths="200px"> | |||
F1.large.jpg | Schematic representation of a vicious circle of events which occurs during chronic bronchial infection. IL: interleukin; TNF: tumour necrosis factor; LT: leukotriene; MMP: matrix metalloproteinase <br> [http://erj.ersjournals.com/content/31/2/396/F1.large.jpg <font size="-2">''European Respiratory Journal''</font>] | |||
</gallery> | |||
==Gross Pathology== | |||
[[File:Bronchiectasis-gross-pathology-1.jpg|thumb|left|369x369px|Bronchiectasis [https://radiopaedia.org/cases/bronchiectasis-gross-pathology-1 Source:Case courtesy of Dr Yale Rosen, Radiopaedia.org, rID: 9307]]] | |||
<br clear="left" /> | |||
==References== | ==References== | ||
{{Reflist|2}} | {{Reflist|2}} | ||
| |||
| |||
{{WH}} | |||
{{WS}} | |||
[[Category:Pulmonology]] | [[Category:Pulmonology]] | ||
[[Category: | [[Category:Medicine]] | ||
[[Category: | [[Category:Up-To-Date]] | ||
Latest revision as of 20:43, 29 July 2020
|
Bronchiectasis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Bronchiectasis pathophysiology On the Web |
|
American Roentgen Ray Society Images of Bronchiectasis pathophysiology |
|
Risk calculators and risk factors for Bronchiectasis pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hamid Qazi, MD, BSc [2], Saarah T. Alkhairy, M.D.
Overview
Bronchiectasis involves cycles of infections and inflammation that result in alveolar damage and inelastic dilated bronchi. Damage to the airway results in airflow obstruction and impaired clearance of secretions.
Pathophysiology
The following events summarize the pathophysiology of bronchiectasis:[1]
- Dilation of the bronchial walls results in airflow obstruction and impaired clearance of secretions.
- The dilated areas interrupt normal air pressure of the bronchial tubes, causing sputum to pool inside the dilated areas instead of being pushed upward.
- The sputum contains elastase, interleukin-8, tumor necrosis factor alpha (TNF-a), and prostanoids.
- The pooled sputum provides an environment favorable to the growth of infectious pathogens.
- Recurrent infections are followed inflammation and infiltration of neutrophils, macrophages, and T-lymphocytes.
- The more infection that the lungs experience, leads to the sustained inflammation, consequently, damage to the alveoli in the lungs.
- With more injury to the lung tissue, the elasticity in the bronchial tubes is reduced and the tubes are dilated, which creates a perpetual destructive cycle
Cole's Cycle
The following events summarize Cole's cycle (Cole's "vicious cycle hypothesis"), which is the most widely known model of the development of bronchiectasis:[2]
- Two factors are required for the development of bronchiectasis:
- Persistent infection
- Host defense derangement
- Impaired mucociliary clearance due to the genetic susceptibility may cause environmental insult.
- Insults result in persistence of microbes in the sinobronchial tree.
- The microbial infection can cause chronic inflammation, which may result in tissue damage and impaired mucociliary motility.
- Inflammation ensues more infection, which in turn ensues more inflammation.
Immune Response
- Bronchiectasis involves the activity of reactive oxygen species (ROS), elastases, and matrix metalloproteinases (MMPs):
- Reactive oxygen species (ROS)
- A by product for the metabolism of oxygen
- Increased concentration may result in cell structure damage
- Reactive oxygen species (ROS)
- Elastase
- Protease that catalyzes the breaks down of elastin.
- Elastin plus collagen determine the mechanical properties of connective tissue.
- Matrix metalloproteinases (MMPs)
- Responsible for the degradation of the majority of the extracellular proteins during normal tissue turn over.
- Inflammation may result in epithelial injury and mucus secretion via increased concentrations of ROS, elastase ciliotoxin, and mucus secretogogues.
- Epithelial injury and mucus hypersecretion lead to chronic bronchial infection, reduced mucociliary clearance, and plugging of the airway - which all eventually leads to airway damage and bronchiectasis.
The diagram below depicts the immune response for bronchiectasis:
-
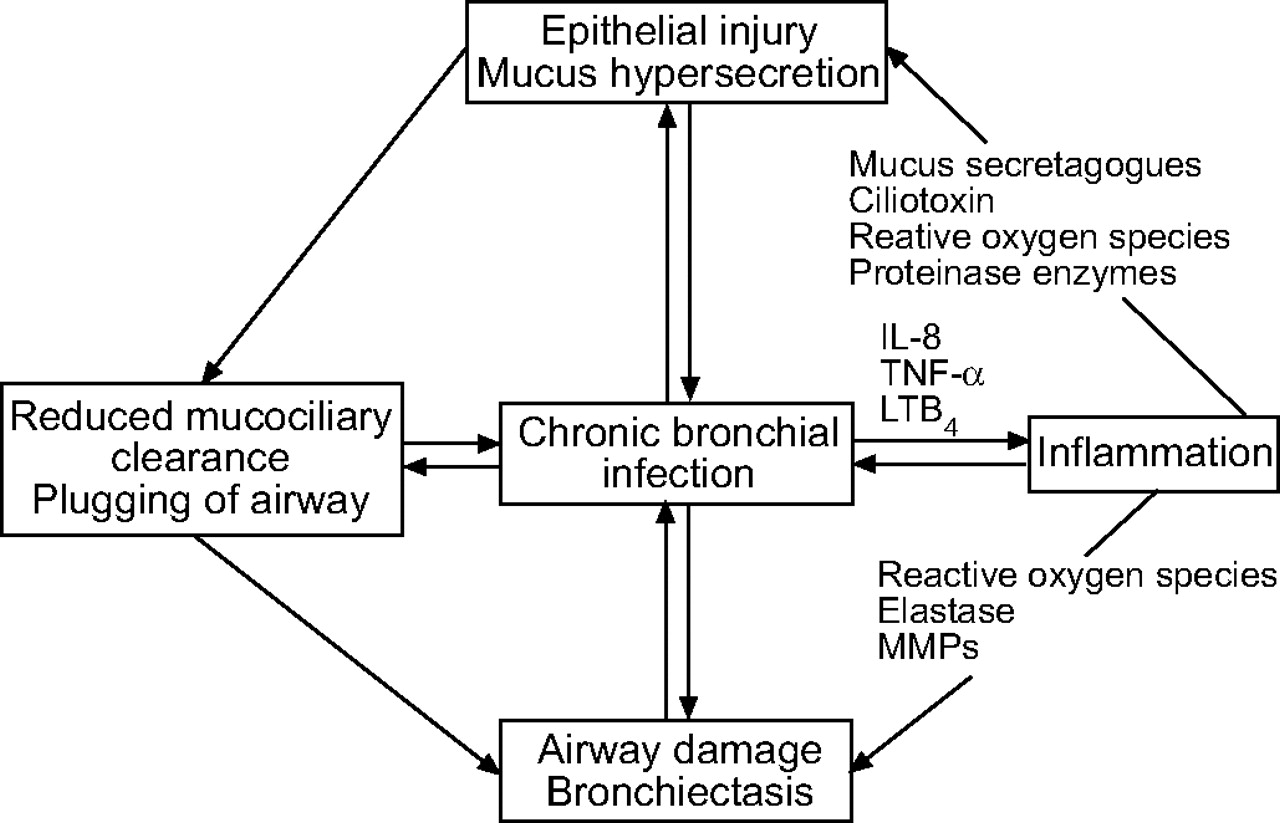
Schematic representation of a vicious circle of events which occurs during chronic bronchial infection. IL: interleukin; TNF: tumour necrosis factor; LT: leukotriene; MMP: matrix metalloproteinase
European Respiratory Journal

{kind=link}
Gross Pathology

References
Template:WH Template:WS