Naloxone
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Vignesh Ponnusamy, M.B.B.S. [2]
Disclaimer
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Overview
Naloxone is an opioid antagonist that is FDA approved for the treatment of known or suspected opioid overdose, as manifested by respiratory and/or central nervous system depression. Common adverse reactions include hypotension, hypertension, ventricular tachycardia, ventricular fibrillation, dyspnea, pulmonary edema, cardiac arrest, death, coma, and encephalopathy.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Opioid Overdose
- Naloxone is an opioid antagonist indicated for the emergency treatment of known or suspected opioid overdose, as manifested by respiratory and/or central nervous system depression.
- Naloxone is intended for immediate administration as emergency therapy in settings where opioids may be present.
- Naloxone is not a substitute for emergency medical care.
- Administer the initial dose of Naloxone to adult intramuscularly or subcutaneously into the anterolateral aspect of the thigh, through clothing if necessary, and seek emergency medical assistance. Administer Naloxone as quickly as possible because prolonged respiratory depression may result in damage to the central nervous system or death. The requirement for repeat doses of Naloxone depends upon the amount, type, and route of administration of the opioid being antagonized.
- If the desired response is not obtained after 2 or 3 minutes, another Naloxone dose may be administered. If there is still no response and additional doses are available, additional Naloxone doses may be administered every 2 to 3 minutes until emergency medical assistance arrives. Additional supportive and/or resuscitative measures may be helpful while awaiting emergency medical assistance.
- Reversal of respiratory depression by partial agonists or mixed agonist/antagonists, such as buprenorphine and pentazocine, may be incomplete or require higher doses of naloxone.
- Injection: 0.4 mg/0.4 mL naloxone hydrochloride solution in a pre-filled auto-injector. Each Naloxone delivers 0.4 mg naloxone hydrochloride injection (0.4 mL).
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Naloxone in adult patients.
Non–Guideline-Supported Use
Opioid-induced constipation
- Naloxone 20 mg or 40 mg.[1]
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
Opioid Overdose
- Naloxone is an opioid antagonist indicated for the emergency treatment of known or suspected opioid overdose, as manifested by respiratory and/or central nervous system depression.
- Naloxone is intended for immediate administration as emergency therapy in settings where opioids may be present.
- Naloxone is not a substitute for emergency medical care.
- Administer the initial dose of Naloxone to pediatric patients intramuscularly or subcutaneously into the anterolateral aspect of the thigh, through clothing if necessary, and seek emergency medical assistance. Administer Naloxone as quickly as possible because prolonged respiratory depression may result in damage to the central nervous system or death. The requirement for repeat doses of Naloxone depends upon the amount, type, and route of administration of the opioid being antagonized.
- If the desired response is not obtained after 2 or 3 minutes, another Naloxone dose may be administered. If there is still no response and additional doses are available, additional Naloxone doses may be administered every 2 to 3 minutes until emergency medical assistance arrives. Additional supportive and/or resuscitative measures may be helpful while awaiting emergency medical assistance.
- Reversal of respiratory depression by partial agonists or mixed agonist/antagonists, such as buprenorphine and pentazocine, may be incomplete or require higher doses of naloxone.
- In pediatric patients under the age of one, the caregiver should pinch the thigh muscle while administering Naloxone.
- Injection: 0.4 mg/0.4 mL naloxone hydrochloride solution in a pre-filled auto-injector. Each Naloxone delivers 0.4 mg naloxone hydrochloride injection (0.4 mL).
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Naloxone in pediatric patients.
Non–Guideline-Supported Use
Antidiarrheal overdose, Diphenoxylate
- Naloxone 0.05 mg IM.[2]
Contraindications
- Naloxone is contraindicated in patients known to be hypersensitive to naloxone hydrochloride or to any of the other ingredients.
Warnings
Precautions
- Duration of Effect
- The duration of action of most opioids is likely to exceed that of Naloxone resulting in a return of respiratory and/or central nervous system depression after an initial improvement in symptoms. Therefore, it is necessary to seek immediate emergency medical assistance after delivering the first dose of Naloxone, keep the patient under continued surveillance, and repeat doses of Naloxone as necessary. Additional supportive and/or resuscitative measures may be helpful while awaiting emergency medical assistance.
- Limited Efficacy with Partial Agonists or Mixed Agonist/Antagonists
- Reversal of respiratory depression by partial agonists or mixed agonist/antagonists such as buprenorphine and pentazocine, may be incomplete. Large doses of naloxone hydrochloride are required to antagonize buprenorphine because the latter has a long duration of action due to its slow rate of binding and subsequent slow dissociation from the opioid receptor. Buprenorphine antagonism is characterized by a gradual onset of the reversal effects and a decreased duration of action of the normally prolonged respiratory depression.
- Precipitation of Severe Opioid Withdrawal
- The use of Naloxone in patients who are opioid dependent may precipitate an acute abstinence syndrome characterized by the following signs and symptoms: body aches, diarrhea, tachycardia, fever, runny nose, sneezing, piloerection, sweating, yawning, nausea or vomiting, nervousness, restlessness or irritability, shivering or trembling, abdominal cramps, weakness, and increased blood pressure. In neonates, opioid withdrawal may be life-threatening if not recognized and properly treated and may include the following signs and symptoms: convulsions, excessive crying, and hyperactive reflexes.
- Abrupt postoperative reversal of opioid depression after using naloxone hydrochloride may result in nausea, vomiting, sweating, tremulousness, tachycardia, hypotension, hypertension, seizures, ventricular tachycardia and fibrillation, pulmonary edema, and cardiac arrest. Death, coma, and encephalopathy have been reported as sequelae of these events. These events have occurred in patients most of whom had pre-existing cardiovascular disorders or received other drugs which may have similar adverse cardiovascular effects. Although a direct cause and effect relationship has not been established, after use of naloxone hydrochloride, patients with pre-existing cardiac disease or patients who have received medications with potential adverse cardiovascular effects should be monitored for hypotension, ventricular tachycardia or fibrillation, and pulmonary edema in an appropriate healthcare setting. It has been suggested that the pathogenesis of pulmonary edema associated with the use of naloxone hydrochloride is similar to neurogenic pulmonary edema, i.e., a centrally mediated massive catecholamine response leading to a dramatic shift of blood volume into the pulmonary vascular bed resulting in increased hydrostatic pressures.
Adverse Reactions
Clinical Trials Experience
- The following adverse reactions have been identified during post-approval use of naloxone hydrochloride in the post-operative setting. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure: Hypotension, hypertension, ventricular tachycardia and fibrillation, dyspnea, pulmonary edema, and cardiac arrest. Death, coma, and encephalopathy have been reported as sequelae of these events. Excessive doses of naloxone hydrochloride in post-operative patients have resulted in significant reversal of analgesia and have caused agitation.
- Abrupt reversal of opioid effects in persons who were physically dependent on opioids has precipitated an acute withdrawal syndrome. Signs and symptoms have included: body aches, fever, sweating, runny nose, sneezing, piloerection, yawning, weakness, shivering or trembling, nervousness, restlessness or irritability, diarrhea, nausea or vomiting, abdominal cramps, increased blood pressure, tachycardia. In the neonate, opioid withdrawal signs and symptoms also included: convulsions, excessive crying, hyperactive reflexes.
Postmarketing Experience
There is limited information regarding Postmarketing Experience of Naloxone in the drug label.
Drug Interactions
There is limited information regarding Naloxone Drug Interactions in the drug label.
Use in Specific Populations
Pregnancy
- Pregnancy Category B
- Risk Summary
- There are no adequate and well-controlled studies with Naloxone in pregnant women. Animal studies were conducted with naloxone hydrochloride given during organogenesis in mice and rats at doses 4-times and 8-times, respectively, the dose of a 50 kg human given 10 mg/day. These studies demonstrated no embryotoxic or teratogenic effects due to naloxone hydrochloride. Because animal reproduction studies are not always predictive of human response, Naloxone should be used during pregnancy only if clearly needed.
- Clinical Considerations
- Naloxone hydrochloride crosses the placenta, and may precipitate withdrawal in the fetus as well as in the opioid-dependent mother. The fetus should be evaluated for signs of distress after Naloxone is used. Careful monitoring is needed until the fetus and mother are stabilized.
- Data
- Animal Data
- Naloxone hydrochloride was administered during organogenesis to mice and rats at doses 4-times and 8-times, respectively, the dose of 10 mg/day given to a 50 kg human (when based on body surface area or mg/m2). These studies demonstrated no embryotoxic or teratogenic effects due to naloxone hydrochloride.
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Naloxone in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Naloxone during labor and delivery.
Nursing Mothers
- It is not known whether naloxone hydrochloride is present in human milk. Because many drugs are present in human milk, exercise caution when Naloxone is administered to a nursing woman.
Pediatric Use
- The safety and effectiveness of Naloxone (for intramuscular and subcutaneous use) have been established in pediatric patients for known or suspected opioid overdose, as manifested by respiratory and/or central nervous system depression. Use of naloxone hydrochloride in pediatric patients is supported by evidence from adequate and well-controlled studies of naloxone hydrochloride in adults with additional data from 15 clinical studies (controlled and uncontrolled) in which neonates and pediatric patients received parenteral naloxone in doses ranging from 0.005 mg/kg to 0.01 mg/kg. Safety and effectiveness are also supported by use of other naloxone hydrochloride products in the post-marketing setting as well as data available in the medical literature and clinical practice guidelines.
- Absorption of naloxone hydrochloride following subcutaneous or intramuscular administration in pediatric patients may be erratic or delayed. Even when the opiate-intoxicated pediatric patient responds dramatically to naloxone hydrochloride injection, he/she must be carefully monitored for at least 24 hours as a relapse may occur as naloxone is metabolized. In opioid-dependent pediatric patients, (including neonates), administration of naloxone may result in an abrupt and complete reversal of opioid effects, precipitating an acute opioid withdrawal syndrome. Neonatal opioid withdrawal syndrome, unlike opioid withdrawal syndrome in adults, may be life-threatening and should be treated according to protocols developed by neonatology experts.
- In neonates and pediatric patients less than 1 year of age, careful observation of the administration site for evidence of residual needle parts and/or signs of infection is warranted.
Geriatic Use
- Geriatric patients have a greater frequency of decreased hepatic, renal, or cardiac function and of concomitant disease or other drug therapy. Therefore, the systemic exposure of naloxone can be higher in these patients.
- Clinical studies of naloxone hydrochloride did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients.
Gender
There is no FDA guidance on the use of Naloxone with respect to specific gender populations.
Race
There is no FDA guidance on the use of Naloxone with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Naloxone in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Naloxone in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Naloxone in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Naloxone in patients who are immunocompromised.
Administration and Monitoring
Administration
- Intramuscular
- Subcutaneous
Monitoring
There is limited information regarding Monitoring of Naloxone in the drug label.
IV Compatibility
There is limited information regarding IV Compatibility of Naloxone in the drug label.
Overdosage
Chronic Overdose
There is limited information regarding Chronic Overdose of Naloxone in the drug label.
Pharmacology


Mechanism of Action
- Naloxone hydrochloride is an opioid antagonist that antagonizes opioid effects by competing for the same receptor sites.
- Naloxone hydrochloride reverses the effects of opioids, including respiratory depression, sedation, and hypotension. Also, it can reverse the psychotomimetic and dysphoric effects of agonist-antagonists such as pentazocine.
Structure
- Naloxone (naloxone hydrochloride injection, USP) is a pre-filled, single-use auto-injector. Naloxone is not made with natural rubber latex. Chemically, naloxone hydrochloride is the hydrochloride salt of 17-Allyl-4,5α-epoxy-3,14-dihydroxymorphinan-6-one hydrochloride with the following structure:
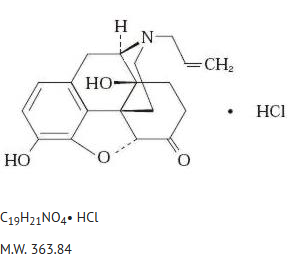
This image is provided by the National Library of Medicine.

- Naloxone hydrochloride occurs as a white to slightly off-white powder, and is soluble in water, in dilute acids, and in strong alkali; slightly soluble in alcohol; practically insoluble in ether and in chloroform.
- Each 0.4 mL in Naloxone contains inactive ingredients of 3.34 mg of sodium chloride, hydrochloric acid to adjust pH, and water for injection. The pH range is 3.0 to 4.5.
Pharmacodynamics
- When naloxone hydrochloride is administered intravenously, the onset of action is generally apparent within two minutes. The time to onset of action is shorter for intravenous compared to subcutaneous or intramuscular routes of administration.
- The duration of action is dependent upon the dose and route of administration of naloxone hydrochloride.
Pharmacokinetics
- In one pharmacokinetic study in 30 healthy subjects, a single 0.4 mg subcutaneous or intramuscular naloxone injection administered using Naloxone provides equivalent naloxone AUC and 15% greater naloxone Cmax in comparison to a single 0.4 mg subcutaneous or intramuscular naloxone injection administered using a standard syringe.
- Following a single Naloxone injection, the median Tmax of naloxone was reached at 15 minutes (range 5 minutes to 1.2 hours), with a mean (± SD) Cmax value of 1.24 (± 0.64) ng/mL. The mean (± SD) plasma half-life of naloxone in healthy adults was 1.28 (± 0.48) hours. In the same study, following administration of a single dose of 0.4 mg naloxone injection using a standard syringe, the median Tmax was 20 minutes (range 5 minutes to 2.03 hours) and the mean (± SD) Cmax value was 1.07 (± 0.48) ng/mL. The mean (± SD) plasma half-life was 1.36 (± 0.32) hours.
- Distribution
- Following parenteral administration, naloxone is distributed in the body and readily crosses the placenta. Plasma protein binding occurs but is relatively weak. Plasma albumin is the major binding constituent but significant binding of naloxone also occurs to plasma constituents other than albumin. It is not known whether naloxone is excreted into human milk.
- Metabolism
- Naloxone hydrochloride is metabolized in the liver, primarily by glucuronide conjugation with naloxone-3-glucoronide as the major metabolite.
- Elimination
- After an oral or intravenous dose, about 25-40% of naloxone is excreted as metabolites in urine within 6 hours, about 50% in 24 hours, and 60-70% in 72 hours. Following a single Naloxone injection, the mean (± SD) plasma half-life of naloxone in healthy adults was 1.28 (± 0.48) hours. In a neonatal study of naloxone injection, the mean (± SD) plasma half-life was observed to be 3.1 (± 0.5) hours.
Nonclinical Toxicology
- Carcinogenesis
- Long-term animal studies to evaluate the carcinogenic potential of naloxone have not been completed.
- Mutagenesis
- Naloxone was weakly positive in the Ames mutagenicity and in the in vitro human lymphocyte chromosome aberration test but was negative in the in vitro Chinese hamster V79 cell HGPRT mutagenicity assay and in the in vivo rat bone marrow chromosome aberration study.
- Impairment of Fertility
- Reproduction studies conducted in mice and rats at doses 4-times and 8-times, respectively, the dose of a 50 kg human given 10 mg/day (when based on surface area or mg/m2), demonstrated no adverse effect of naloxone hydrochloride on fertility.
Clinical Studies
There is limited information regarding Clinical Studies of Naloxone in the drug label.
How Supplied
- Carton containing two Naloxone (naloxone hydrochloride injection, USP) 0.4 mg auto-injectors and a single Trainer for Naloxone - NDC 60842-030-01
- Storage and Handling
- Store Naloxone in the outer case provided.
- Store at controlled room temperature 15°C to 25°C (59°F to 77°F) excursions permitted between 4°C and 40°C (between 39°F and 104°F).
- Before using, check to make sure the solution in the auto-injector is not discolored. Replace Naloxone if the solution is discolored or contains a precipitate.
Storage
There is limited information regarding Naloxone Storage in the drug label.
Images
Drug Images
{{#ask: Page Name::Naloxone |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Naloxone |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
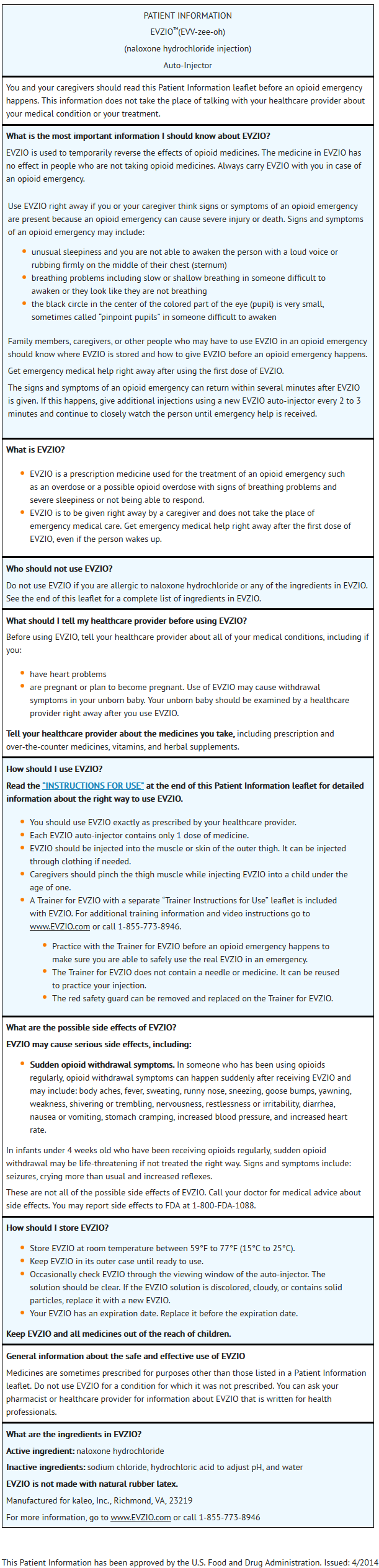
Patient Counseling Information
- Advise the patient and family members or caregivers to read the FDA-approved patient labeling (Instructions for Use).
- Instruct patients and their family members or caregivers to:
- Become familiar with the following information contained in the carton as soon as they receive EVZIO:
- EVZIO Instructions for Use
- Trainer for EVZIO Instructions for Use
- Trainer for EVZIO
- Become familiar with the following information contained in the carton as soon as they receive EVZIO:
- Practice using the Trainer before EVZIO is needed.
- Each EVZIO (which is purple and yellow) can only be used one time; however, the Trainer (which is black and white) can be re-used for training purposes and its red safety guard can be removed and replaced.
- Both EVZIO and the Trainer for EVZIO incorporate the electronic voice instruction system.
- Practice using the Trainer before EVZIO is needed.
- Make sure EVZIO is present whenever persons may be intentionally or accidentally exposed to an opioid to treat serious opioid overdose (i.e., opioid emergencies).
- Instruct the patients and their family members or caregivers how to recognize the signs and symptoms of an opioid overdose requiring the use of EVZIO such as the following:
- Extreme sleepiness - inability to awaken a patient verbally or upon a firm sternal rub.
- Breathing problems - this can range from slow or shallow breathing to no breathing in a patient who cannot be awakened.
- Other signs and symptoms that may accompany sleepiness and breathing problems include the following:
- Extremely small pupils (the black circle in the center of the colored part of the eye) sometimes called “pinpoint pupils.”
- Slow heartbeat and/or low blood pressure.
- Instruct them that when in doubt, if a patient is unresponsive, and an opioid overdose is suspected, administer EVZIO as quickly as possible because prolonged respiratory depression may result in damage to the central nervous system or death. Instruct them to seek emergency medical assistance after administering the first dose of EVZIO.
- Duration of Effect
- Instruct patients and their family members or caregivers that since the duration of action of most opioids may exceed that of naloxone, seek immediate emergency medical assistance, keep the patient under continued surveillance, and administer repeated doses of EVZIO as necessary.
- Limited Efficacy for/with Partial Agonists or Mixed Agonist/Antagonists
- Instruct patients and their family members or caregivers that the reversal of respiratory depression by partial agonists or mixed agonist/antagonists such as buprenorphine and pentazocine, may be incomplete.
- Precipitation of Severe Opioid Withdrawal
- Instruct patients and their family members or caregivers that the use of EVZIO in patients who are opioid dependent may precipitate an acute abstinence syndrome characterized by the following signs and symptoms: body aches, diarrhea, tachycardia, fever, runny nose, sneezing, piloerection, sweating, yawning, nausea or vomiting, nervousness, restlessness or irritability, shivering or trembling, abdominal cramps, weakness, and increased blood pressure. In neonates, opioid withdrawal may be life threatening if not recognized and properly treated, and may include the following signs and symptoms: convulsions, excessive crying, and hyperactive reflexes.
- Administration Instructions
- Instruct patients and their family members or caregivers about the following important information:
- EVZIO is user actuated and may be administered through clothing [e.g., pants, jeans, etc.] if necessary.
- Inject EVZIO while pressing into the anterolateral aspect of the thigh. In pediatric patients less than 1 year of age, pinch the thigh muscle while administering EVZIO.
- Upon actuation, EVZIO automatically inserts the needle intramuscularly or subcutaneously, delivers the naloxone, and retracts the needle fully into its housing. The needle is not visible before, during, or after injection.
- Each EVZIO can only be used one time.
- If the electronic voice instruction system on EVZIO does not work properly, EVZIO will still deliver the intended dose of naloxone hydrochloride when used according to the printed instructions on its label.
- The electronic voice instructions are independent of activating EVZIO and are not required to wait for the voice instructions to be completed prior to moving to the next step in the injection process.
- Post-injection, the black base locks in place, a red indicator appears in the viewing window and electronic visual and audible instructions signal that EVZIO has delivered the intended dose of naloxone hydrochloride.
- EVZIO’s red safety guard should not be replaced under any circumstances. However, the Trainer is designed for re-use and its red safety guard can be removed and replaced.
- It is recommended that patients and caregivers become familiar with the training device provided and read the Instructions for Use; however, untrained caregivers or family members should still attempt to use EVZIO during a suspected opioid overdose while awaiting definitive emergency medical care.
- Periodically visually inspect the naloxone solution through the viewing window. If the solution is discolored, cloudy, or contains solid particles, replace it with a new EVZIO.
- Replace EVZIO before its expiration date.
- Instruct patients and their family members or caregivers about the following important information:
This image is provided by the National Library of Medicine.


This image is provided by the National Library of Medicine.


This image is provided by the National Library of Medicine.

Precautions with Alcohol
- Alcohol-Naloxone interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- EVZIO®[3]
Look-Alike Drug Names
- naloxone® — Lanoxin®[4]
- Narcan® — Norcuron®[4]
Drug Shortage Status
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
- ↑ Meissner W, Leyendecker P, Mueller-Lissner S, Nadstawek J, Hopp M, Ruckes C; et al. (2009). "A randomised controlled trial with prolonged-release oral oxycodone and naloxone to prevent and reverse opioid-induced constipation". Eur J Pain. 13 (1): 56–64. doi:10.1016/j.ejpain.2008.06.012. PMID 18762438.
- ↑ McCarron MM, Challoner KR, Thompson GA (1991). "Diphenoxylate-atropine (Lomotil) overdose in children: an update (report of eight cases and review of the literature)". Pediatrics. 87 (5): 694–700. PMID 2020516.
- ↑ "EVZIO naloxone hydrochloride injection, solution".
- ↑ 4.0 4.1 "http://www.ismp.org". External link in
|title=(help)
{{#subobject:
|Page Name=Naloxone
|Pill Name=No image.jpg
|Drug Name=
|Pill Ingred=|+sep=;
|Pill Imprint=
|Pill Dosage={{{dosageValue}}} {{{dosageUnit}}}
|Pill Color=|+sep=;
|Pill Shape=
|Pill Size (mm)=
|Pill Scoring=
|Pill Image=
|Drug Author=
|NDC=
}}
{{#subobject:
|Label Page=Naloxone |Label Name=Naloxone05.png
}}
{{#subobject:
|Label Page=Naloxone |Label Name=Naloxone06.png
}}
{{#subobject:
|Label Page=Naloxone |Label Name=Naloxone07.png
}}
{{#subobject:
|Label Page=Naloxone |Label Name=Naloxone08.png
}}
{{#subobject:
|Label Page=Naloxone |Label Name=Naloxone09.png
}}
{{#subobject:
|Label Page=Naloxone |Label Name=Naloxone10.png
}}
{{#subobject:
|Label Page=Naloxone |Label Name=Naloxone11.png
}}