Wilms' tumor other diagnostic studies: Difference between revisions
Jump to navigation
Jump to search
Sargun Walia (talk | contribs) (→Biopsy) |
Ahmed Younes (talk | contribs) No edit summary |
||
| (8 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
__NOTOC__ | __NOTOC__ | ||
{{Wilms' tumor}} | {{Wilms' tumor}} | ||
{{CMG}}; {{AE}} {{ | {{CMG}}; {{AE}} {{SSW}} | ||
==Overview== | ==Overview== | ||
Other diagnostic studies for Wilms tumor include [[PET scan]] and histology of biopsy samples taken. | |||
==Other Diagnostic Studies== | ==Other Diagnostic Studies== | ||
Other diagnostic studies for | Other diagnostic studies for Wilms tumor include: | ||
* '''PET scan'''<ref name="pmid27001573">{{cite journal |vauthors=Hildebrandt MG, Gerke O, Baun C, Falch K, Hansen JA, Farahani ZA, Petersen H, Larsen LB, Duvnjak S, Buskevica I, Bektas S, Søe K, Jylling AM, Ewertz M, Alavi A, Høilund-Carlsen PF |title=[18F]Fluorodeoxyglucose (FDG)-Positron Emission Tomography (PET)/Computed Tomography (CT) in Suspected Recurrent Breast Cancer: A Prospective Comparative Study of Dual-Time-Point FDG-PET/CT, Contrast-Enhanced CT, and Bone Scintigraphy |journal=J. Clin. Oncol. |volume=34 |issue=16 |pages=1889–97 |date=June 2016 |pmid=27001573 |doi=10.1200/JCO.2015.63.5185 |url=}}</ref> | * '''PET scan'''<ref name="pmid27001573">{{cite journal |vauthors=Hildebrandt MG, Gerke O, Baun C, Falch K, Hansen JA, Farahani ZA, Petersen H, Larsen LB, Duvnjak S, Buskevica I, Bektas S, Søe K, Jylling AM, Ewertz M, Alavi A, Høilund-Carlsen PF |title=[18F]Fluorodeoxyglucose (FDG)-Positron Emission Tomography (PET)/Computed Tomography (CT) in Suspected Recurrent Breast Cancer: A Prospective Comparative Study of Dual-Time-Point FDG-PET/CT, Contrast-Enhanced CT, and Bone Scintigraphy |journal=J. Clin. Oncol. |volume=34 |issue=16 |pages=1889–97 |date=June 2016 |pmid=27001573 |doi=10.1200/JCO.2015.63.5185 |url=}}</ref> | ||
** 18F-fluorodeoxyglucose (FDG)-positron emission tomography (PET)-CT. | ** 18F-fluorodeoxyglucose (FDG)-positron emission tomography (PET)-CT. | ||
** Wilms tumor is 18F-FDG avid, and 18F-FDG-PET-CT imaging adds clinically applicable information to conventional imaging. | ** Wilms tumor is 18F-FDG avid, and 18F-FDG-PET-CT imaging adds clinically applicable information to conventional imaging. | ||
** This may be particularly helpful in patients with bilateral disease or those receiving preoperative chemotherapy. | ** This may be particularly helpful in patients with bilateral disease or those receiving [[Chemotherapy|preoperative chemotherapy]]. | ||
** 18F-FDG-PET-CT highlights FDG-avid areas in the tumor and metastases. | ** 18F-FDG-PET-CT highlights FDG-avid areas in the [[tumor]] and [[metastases]]. | ||
** This corresponds to histologically confirmed active disease. | ** This corresponds to histologically confirmed active disease. | ||
* '''Biopsy''' | * '''Biopsy''' | ||
** Histology of the biopsy sample taken during surgery is the gold standard for the diagnosis of | ** Histology of the [[biopsy]] sample taken during surgery is the [[Gold standard (test)|gold standard]] for the diagnosis of Wilms tumor.<ref name="pmid4728859">{{cite journal |vauthors=Tentzeris M, Fritz G |title=[Suction and irrigation drainage in the therapy of acute and chronic osteomyelitis] |language=German |journal=Zentralbl Chir |volume=98 |issue=21 |pages=771–4 |date=May 1973 |pmid=4728859 |doi= |url=}}</ref><ref name="pmid157385942">{{cite journal |vauthors=Stefanowicz J, Sierota D, Balcerska A, Stoba C |title=[Wilms' tumour of unfavorable histology--results of treatment with the SIOP 93-01 protocol at the Gdańsk centre. Preliminary report] |language=Polish |journal=Med Wieku Rozwoj |volume=8 |issue=2 Pt 1 |pages=197–200 |date=2004 |pmid=15738594 |doi= |url=}}</ref> | ||
** The following result of histology is confirmatory of | ** The following result of histology is confirmatory of Wilms tumor:<ref name="pmid373364">{{cite journal |vauthors=Hansz J, Prazmowska-Owczarek B, Nowicka G |title=[Granulocyte adherence in advanced Hodgkin's disease and its dependence on antiproliferative drugs used] |language=Polish |journal=Acta Haematol Pol |volume=10 |issue=1 |pages=7–12 |date=1979 |pmid=373364 |doi= |url=}}</ref> | ||
***Triphasic histology comprising - | ***Triphasic histology comprising - | ||
****[[Epithelial cells]] | ****[[Epithelial cells]] | ||
| Line 22: | Line 22: | ||
****[[Stromal cell|Stromal cells]] | ****[[Stromal cell|Stromal cells]] | ||
***[[Anaplasia|Anaplastic]] changes | ***[[Anaplasia|Anaplastic]] changes | ||
***Most of the tumors of the kidney have a favorable histology(90%). | ***Most of the tumors of the [[kidney]] have a favorable histology(90%). | ||
***If [[Anaplasia|anaplastic]] changes(3-7%) are found then the outcome is poor.<ref name="pmid15738594">{{cite journal |vauthors=Stefanowicz J, Sierota D, Balcerska A, Stoba C |title=[Wilms' tumour of unfavorable histology--results of treatment with the SIOP 93-01 protocol at the Gdańsk centre. Preliminary report] |language=Polish |journal=Med Wieku Rozwoj |volume=8 |issue=2 Pt 1 |pages=197–200 |date=2004 |pmid=15738594 |doi= |url=}}</ref> | ***If [[Anaplasia|anaplastic]] changes(3-7%) are found then the outcome is poor.<ref name="pmid15738594">{{cite journal |vauthors=Stefanowicz J, Sierota D, Balcerska A, Stoba C |title=[Wilms' tumour of unfavorable histology--results of treatment with the SIOP 93-01 protocol at the Gdańsk centre. Preliminary report] |language=Polish |journal=Med Wieku Rozwoj |volume=8 |issue=2 Pt 1 |pages=197–200 |date=2004 |pmid=15738594 |doi= |url=}}</ref> | ||
[[File:Wilms tumour - very high mag.jpg|center|thumb|450x450px|Wilms tumor histology | |||
The images show the characteristic three components: | |||
1.Blastema component - Malignant small round (blue) cells ~ 2x the size of resting lymphocyte. | |||
2.Epithelial component - Tubular structures/rosettes. | |||
3.Stromal component - Loose paucicellular stroma with spindle cells. | |||
'''Source''':By Nephron [CC BY-SA 3.0 (<nowiki>https://creativecommons.org/licenses/by-sa/3.0</nowiki>) or GFDL (<nowiki>http://www.gnu.org/copyleft/fdl.html</nowiki>)], from Wikimedia Commons<ref>https://librepathology.org/wiki/File:Wilms_tumour_-_low_mag.jpg#filelinks</ref> | |||
]] | |||
**The surgical examination and biopsy must be performed when: | |||
*** If a case of Wilms tumor is suspected in North America, then [[nephrectomy]] is done immediately. | |||
*** Contralateral kidney is also explored to check for disease and [[lymph node]] biopsies done. | |||
*** Transcutaneous biopsy samples are almost never taken to prevent: | |||
**** Tumor spill - If this occurs then whole abdomen [[Radiation therapy|radiotherapy]] has to be done. | |||
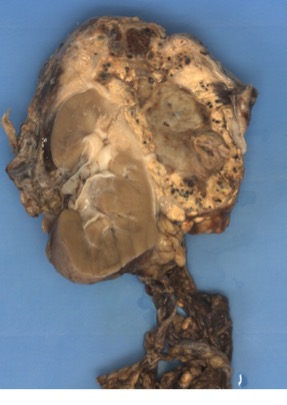
[[File:Wilms Tumour nephrectomy.jpg|center|thumb|405x405px|•Tumor is seen in the upper pole of the kidney. | |||
•Well circumscribed lesion is seen with multiple necrotic, hemorrhagic and cystic changes. | |||
'''Source:'''By Abepathology [CC BY-SA 4.0 (<nowiki>https://creativecommons.org/licenses/by-sa/4.0</nowiki>)], from Wikimedia Commons<ref>https://upload.wikimedia.org/wikipedia/commons/a/a8/Wilms_Tumour.jpg</ref> | |||
]] | |||
==References== | ==References== | ||
Latest revision as of 17:29, 10 July 2018
|
Wilms' tumor Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Wilms' tumor other diagnostic studies On the Web |
|
American Roentgen Ray Society Images of Wilms' tumor other diagnostic studies |
|
Risk calculators and risk factors for Wilms' tumor other diagnostic studies |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sargun Singh Walia M.B.B.S.[2]
Overview
Other diagnostic studies for Wilms tumor include PET scan and histology of biopsy samples taken.
Other Diagnostic Studies
Other diagnostic studies for Wilms tumor include:
- PET scan[1]
- 18F-fluorodeoxyglucose (FDG)-positron emission tomography (PET)-CT.
- Wilms tumor is 18F-FDG avid, and 18F-FDG-PET-CT imaging adds clinically applicable information to conventional imaging.
- This may be particularly helpful in patients with bilateral disease or those receiving preoperative chemotherapy.
- 18F-FDG-PET-CT highlights FDG-avid areas in the tumor and metastases.
- This corresponds to histologically confirmed active disease.
- Biopsy
- Histology of the biopsy sample taken during surgery is the gold standard for the diagnosis of Wilms tumor.[2][3]
- The following result of histology is confirmatory of Wilms tumor:[4]
- Triphasic histology comprising -
- Anaplastic changes
- Most of the tumors of the kidney have a favorable histology(90%).
- If anaplastic changes(3-7%) are found then the outcome is poor.[5]

- The surgical examination and biopsy must be performed when:
- If a case of Wilms tumor is suspected in North America, then nephrectomy is done immediately.
- Contralateral kidney is also explored to check for disease and lymph node biopsies done.
- Transcutaneous biopsy samples are almost never taken to prevent:
- Tumor spill - If this occurs then whole abdomen radiotherapy has to be done.
- The surgical examination and biopsy must be performed when:

References
- ↑ Hildebrandt MG, Gerke O, Baun C, Falch K, Hansen JA, Farahani ZA, Petersen H, Larsen LB, Duvnjak S, Buskevica I, Bektas S, Søe K, Jylling AM, Ewertz M, Alavi A, Høilund-Carlsen PF (June 2016). "[18F]Fluorodeoxyglucose (FDG)-Positron Emission Tomography (PET)/Computed Tomography (CT) in Suspected Recurrent Breast Cancer: A Prospective Comparative Study of Dual-Time-Point FDG-PET/CT, Contrast-Enhanced CT, and Bone Scintigraphy". J. Clin. Oncol. 34 (16): 1889–97. doi:10.1200/JCO.2015.63.5185. PMID 27001573.
- ↑ Tentzeris M, Fritz G (May 1973). "[Suction and irrigation drainage in the therapy of acute and chronic osteomyelitis]". Zentralbl Chir (in German). 98 (21): 771–4. PMID 4728859.
- ↑ Stefanowicz J, Sierota D, Balcerska A, Stoba C (2004). "[Wilms' tumour of unfavorable histology--results of treatment with the SIOP 93-01 protocol at the Gdańsk centre. Preliminary report]". Med Wieku Rozwoj (in Polish). 8 (2 Pt 1): 197–200. PMID 15738594.
- ↑ Hansz J, Prazmowska-Owczarek B, Nowicka G (1979). "[Granulocyte adherence in advanced Hodgkin's disease and its dependence on antiproliferative drugs used]". Acta Haematol Pol (in Polish). 10 (1): 7–12. PMID 373364.
- ↑ Stefanowicz J, Sierota D, Balcerska A, Stoba C (2004). "[Wilms' tumour of unfavorable histology--results of treatment with the SIOP 93-01 protocol at the Gdańsk centre. Preliminary report]". Med Wieku Rozwoj (in Polish). 8 (2 Pt 1): 197–200. PMID 15738594.
- ↑ https://librepathology.org/wiki/File:Wilms_tumour_-_low_mag.jpg#filelinks
- ↑ https://upload.wikimedia.org/wikipedia/commons/a/a8/Wilms_Tumour.jpg
{kind=link}
{kind=link}