WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Overview
Niacin/simvastatin is a lipid lowering agents that is FDA approved for the treatment of as an adjunct to diet when the response to a diet restricted in saturated fat and cholesterol and other nonpharmacologic measures alone has been inadequate for hyperlipidemia. Common adverse reactions include headache, pruritis, nausea, back pain, diarrhea.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Therapy with lipid-altering agents should be only one component of multiple risk factor intervention in individuals at significantly increased risk for atherosclerotic vascular disease due to hypercholesterolemia.
Drug therapy is indicated as an adjunct to diet when the response to a diet restricted in saturated fat and cholesterol and other nonpharmacologic measures alone has been inadequate.
Patients with Hypercholesterolemia Requiring Modifications of Lipid Profiles
SIMCOR is indicated to reduce Total-C, LDL-C, Apo B, non-HDL-C, TG, or to increase HDL-C in patients with primary hypercholesterolemia and mixed dyslipidemia when treatment with simvastatin monotherapy or niacin extended-release monotherapy is considered inadequate.
SIMCOR is indicated to reduce TG in patients with hypertriglyceridemia when treatment with simvastatin monotherapy or niacin extended-release monotherapy is considered inadequate.
Limitations of Use
No incremental benefit of SIMCOR on cardiovascular morbidity and mortality over and above that demonstrated for simvastatin monotherapy and niacin monotherapy has been established.
Niacin extended-release, one of the components of SIMCOR, at doses of 1,500 – 2,000 mg/day, in combination with simvastatin, did not reduce the incidence of cardiovascular events more than simvastatin in a randomized controlled trial of patients with cardiovascular disease and mean baseline LDL-C levels of 74 mg per deciliter.
The recommended maintenance dose for SIMCOR is 1000/20 mg to 2000/40 mg (two 1000/20 mg tablets) once daily depending on patient tolerability and lipid levels.
The efficacy and safety of doses of SIMCOR greater than 2000/40 mg daily have not been studied and are therefore not recommended.
If SIMCOR therapy is discontinued for an extended period of time (> 7 days), re-titration as tolerated is recommended. SIMCOR tablets should be taken whole and should not be broken, crushed, or chewed before swallowing.
Due to the increased risk of hepatotoxicity with other modified-release (sustained-release or time-release) niacin preparations or immediate-release (crystalline) niacin, SIMCOR should only be substituted for equivalent doses of niacin extended-release (NIASPAN).
Flushing [see Adverse Reactions (6.1)] may be reduced in frequency or severity by pretreatment with aspirin up to the recommended dose of 325 mg (taken approximately 30 minutes prior to SIMCOR dose).
Flushing, pruritus, and gastrointestinal distress are also reduced by gradually increasing the dose of niacin (refer to TABLE 1) and avoiding administration on an empty stomach.
Concomitant alcoholic, hot drinks or spicy foods may increase the side effects of flushing and pruritus and should be avoided around the time of SIMCOR ingestion.
Coadministration with Other Drugs
Patients taking Amiodarone, Amlodipine or Ranolazine
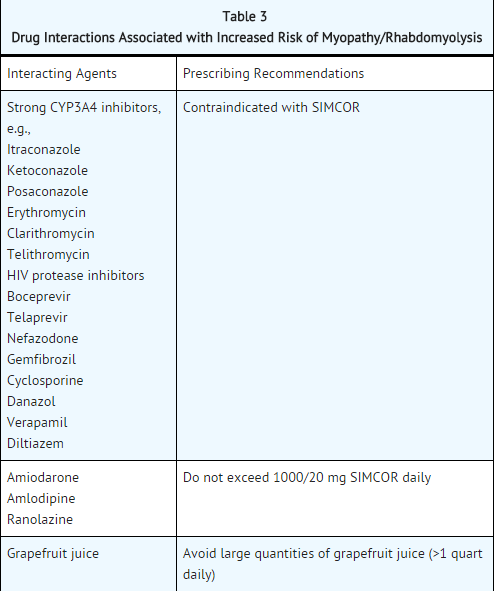
The dose of SIMCOR should not exceed 1000/20 mg/day .
Chinese Patients Taking SIMCOR
Because of an increased risk for myopathy in Chinese patients taking simvastatin 40 mg coadministered with lipid-modifying doses (≥1 g/day niacin) of niacin-containing products, caution should be used when prescribing SIMCOR in doses that exceed 1000/20 mg/day to =====Chinese patients=====
The cause of the increased risk of myopathy is not known. It is also unknown if the risk for myopathy with coadministration of simvastatin with lipid-modifying doses of niacin-containing products observed in Chinese patients applies to other Asian patients.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
Condition1
Developed by:
Class of Recommendation:
Strength of Evidence:
Dosing Information
Dosage
Condition2
There is limited information regarding Off-Label Guideline-Supported Use of Niacin/simvastatin in adult patients.
Non–Guideline-Supported Use
Condition1
Dosing Information
Dosage
Condition2
There is limited information regarding Off-Label Non–Guideline-Supported Use of Niacin/simvastatin in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
Condition1
Dosing Information
Dosage
Condition2
There is limited information regarding FDA-Labeled Use of Niacin/simvastatin in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
Condition1
Developed by:
Class of Recommendation:
Strength of Evidence:
Dosing Information
Dosage
Condition2
There is limited information regarding Off-Label Guideline-Supported Use of Niacin/simvastatin in pediatric patients.
Non–Guideline-Supported Use
Condition1
Dosing Information
Dosage
Condition2
There is limited information regarding Off-Label Non–Guideline-Supported Use of Niacin/simvastatin in pediatric patients.
Contraindications
Active liver disease, which may include unexplained persistent elevations in hepatic transaminase levels.
Patients with active peptic ulcer disease
Patients with arterial bleeding
Concomitant administration of strong CYP3A4 inhibitors (e.g. itraconazole, ketoconazole, posaconazole, HIV protease inhibitors, boceprevir, telaprevir, erythromycin, clarithromycin, telithromycin and nefazodone)
Concomitant administration of gemfibrozil, cyclosporine, or danazol
Concomitant administration of verapamil or diltiazem.
Women who are pregnant or may become pregnant. SIMCOR may cause fetal harm when administered to a pregnant woman. Serum cholesterol and triglycerides increase during normal pregnancy, and cholesterol or cholesterol derivatives are essential for fetal development.
Atherosclerosis is a chronic process and discontinuation of lipid-lowering drugs during pregnancy should have little impact on long-term outcomes of primary hypercholesterolemia therapy.
There are no adequate and well-controlled studies of SIMCOR use during pregnancy; however in rare reports congenital anomalies were observed following intrauterine exposure to HMG-CoA reductase inhibitors.
If SIMCOR is used during pregnancy or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus.
In rat and rabbit animal reproduction studies, simvastatin revealed no evidence of teratogenicity. There are no animal reproductive studies conducted with niacin.
Nursing mothers
SIMCOR contains simvastatin and nicotinic acid. Nicotinic acid is excreted into human milk and it is not known whether simvastatin is excreted into human milk; however a small amount of another drug in this class does pass into breast milk.
Because of the potential for serious adverse reactions in nursing infants, women who require SIMCOR treatment should not breastfeed their infants.
Patients with a known hypersensitivity to any component of this product. Hypersensitivity reactions including one of more of the following adverse reactions have been reported for simvastatin and/or niacin extended-release: anaphylaxis, angioedema, urticaria, fever, dyspnea, tongue edema, larynx edema, face edema, peripheral edema, laryngismus, and flushing.
Warnings
SIMCOR should not be substituted for equivalent doses of immediate-release (crystalline) niacin. For patients switching from immediate-release niacin to SIMCOR, therapy with SIMCOR should be initiated at 500/20 mg and appropriately titrated to the desired therapeutic response.
Patients already taking simvastatin 20-40 mg who need additional management of their lipid levels may be started on a SIMCOR dose of 500/40 mg once daily at bedtime. Doses of SIMCOR greater than 2000/40 mg are not recommended.
Mortality and Coronary Heart Disease Morbidity
The Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglycerides: Impact on Global Health Outcomes (AIM-HIGH) trial was a randomized placebo-controlled trial of 3414 patients with stable, previously diagnosed cardiovascular disease.
Mean baseline lipid levels were LDL-C 74 mg/dL, HDL-C 35 mg/dL, non-HDL-C 111 mg/dL and median triglyceride level of 163-177 mg/dL. Ninety-four percent of patients were on background statin therapy prior to entering the trial. All participants received simvastatin, 40 to 80 mg per day, plus ezetimibe 10 mg per day if needed, to maintain an LDL-C level of 40-80 mg/dL, and were randomized to receive niacin extended-release tablets 1500-2000 mg/day (n=1718) or matching placebo (niacin immediate-release tablets, 100-150 mg, n=1696).
On-treatment lipid changes at two years for LDL-C were -12.0% for the simvastatin plus niacin extended-release group and -5.5% for the simvastatin plus placebo group. HDL-C increased by 25.0% to 42 mg/dL in the simvastatin plus niacin extended-release group and by 9.8% to 38 mg/dL in the simvastatin plus placebo group (P<0.001). Triglyceride levels decreased by 28.6% in the simvastatin plus niacin extended-release group and by 8.1% in the simvastatin plus placebo group.
The primary outcome was an ITT composite of the first study occurrence of coronary heart disease death, nonfatal myocardial infarction, ischemic stroke, hospitalization for acute coronary syndrome or symptom-driven coronary or cerebral revascularization procedures. The trial was stopped after a mean follow-up period of 3 years owing to a lack of efficacy. The primary outcome occurred in 282 patients in the simvastatin plus niacin extended-release group (16.4%) and in 274 patients in the simvastatin plus placebo group (16.2%) (HR 1.02 [95% CI, 0.87-1.21], P=0.79.
In an ITT analysis, there were 42 cases of first occurrence of ischemic stroke reported, 27 (1.6%) in the simvastatin plus niacin extended-release group and 15 (0.9%) in the simvastatin plus placebo group, a non-statistically significant result (HR 1.79, [95%CI = 0.95-3.36], p=0.071).
The on-treatment ischemic stroke events were 19 for the simvastatin plus niacin extended-release group and 15 for the simvastatin plus placebo group.
Myopathy/Rhabdomyolysis
Simvastatin
Simvastatin occasionally causes myopathy manifested as muscle pain, tenderness or weakness with creatine kinase (CK) above ten times the upper limit of normal (ULN). Myopathy sometimes takes the form of rhabdomyolysis with or without acute renal failure secondary to myoglobinuria, and rare fatalities have occurred.
The risk of myopathy is increased by high levels of HMG-CoA reductase inhibitory activity in plasma.Predisposing factors for myopathy include advanced age (≥65 years), female gender, uncontrolled hypothyroidism, and renal impairment.
The risk of myopathy/rhabdomyolysis is dose related. In a clinical trial database in which 41,413 patients were treated with simvastatin with 24,747 (approximately 60%) of whom were enrolled in studies with a median follow-up of at least 4 years, the incidence of myopathy was approximately 0.03% and 0.08% at 20 and 40 mg/day, respectively. The incidence of myopathy with 80 mg (0.61%) was disproportionately higher than that observed at the lower doses. In these trials, patients were carefully monitored and some interacting medicinal products were excluded.
In a clinical trial in which 12,064 patients with a history of myocardial infarction were treated with ZOCOR (mean follow-up 6.7 years), the incidence of myopathy (defined as unexplained muscle weakness or pain with a serum creatine kinase [CK] >10 times upper limit of normal [ULN]) in patients on 80 mg/day was approximately 0.9% compared with 0.02% for patients on 20 mg/day; the incidence of rhabdomyolysis (defined as myopathy with a CK >40 times ULN) was approximately 0.4% in patients on 80 mg/day compared with 0% for patients on 20 mg/day.
The incidence of myopathy, including rhabdomyolysis, was highest during the first year and then notably decreased during the subsequent years of treatment. In this trial, patients were carefully monitored and some interacting medicinal products were excluded.
There have been rare reports of immune-mediated necrotizing myopathy (IMNM), an autoimmune myopathy, associated with statin use. IMNM is characterized by: proximal muscle weakness and elevated serum creatine kinase, which persist despite discontinuation of statin treatment; muscle biopsy showing necrotizing myopathy without significant inflammation; improvement with immunosuppressive agents.
All patients starting therapy with SIMCOR, or whose dose of SIMCOR is being increased, should be advised of the risk of myopathy, including rhabdomyolysis, and told to report promptly any unexplained muscle pain, tenderness or weakness particularly if accompanied by malaise or fever or if muscle signs and symptoms persist after discontinuing SIMCOR.
SIMCOR therapy should be discontinued immediately if myopathy is diagnosed or suspected. In most cases, muscle symptoms and CK increases resolved when treatment was promptly discontinued. Periodic CK determinations may be considered in patients starting therapy with SIMCOR or whose dose is being increased, but there is no assurance that such monitoring will prevent myopathy.
Many of the patients who have developed rhabdomyolysis on therapy with simvastatin have had complicated medical histories, including renal insufficiency usually as a consequence of long-standing diabetes mellitus.
Such patients merit closer monitoring. SIMCOR therapy should be discontinued if markedly elevated CPK levels occur or myopathy is diagnosed or suspected.
SIMCOR therapy should also be temporarily withheld in any patient experiencing an acute or serious condition predisposing to the development of renal failure secondary to rhabdomyolysis, e.g., sepsis; hypotension; major surgery; trauma; severe metabolic, endocrine, or electrolyte disorders; or uncontrolled epilepsy.
Drug Interactions
The risk of myopathy and rhabdomyolysis is increased by high levels of statin activity in plasma. Simvastatin is metabolized by the cytochrome P450 isoform 3A4.
Certain drugs which inhibit this metabolic pathway can raise the plasma levels of simvastatin and may increase the risk of myopathy. These include itraconazole, ketoconazole, and posaconazole, the macrolide antibiotics erythromycin and clarithromycin, and the ketolide antibiotic telithromycin, HIV protease inhibitors, boceprevir, telaprevir, the antidepressant nefazodone, or large quantities of grapefruit juice (>1 quart daily), and combination of these drugs with SIMCOR is contraindicated.
If treatment with itraconazole, ketoconazole, posaconazole, erythromycin, clarithromycin or telithromycin is unavoidable, therapy with SIMCOR must be suspended during the course of treatment.
In vitro studies have demonstrated a potential for voriconazole to inhibit the metabolism of simvastatin. Adjustment of the SIMCOR dose may be needed to reduce the risk of myopathy/rhabdomyolysis if voriconazole must be used concomitantly with simvastatin.
The combined use of SIMCOR with gemfibrozil, cyclosporine, or danazol is contraindicated.
The combined use of SIMCOR with verapamil or diltiazem is contraindicated, because dosages of simvastatin are not to exceed 10 mg when these drugs are co-administered and all doses of SIMCOR contain simvastatin in excess of 10 mg.
The combined use of SIMCOR with drugs that cause myopathy/rhabdomyolysis when given alone, such as fibrates, should be avoided [see Drug Interactions (7.3)].
Cases of myopathy, including rhabdomyolysis, have been reported with simvastatin coadministered with colchicine, and caution should be exercised when prescribing SIMCOR with colchicine [see Drug Interactions (7.8)].
The benefits of the combined use of SIMCOR with amlodipine or ranolazine should be carefully weighed against the potential risks of combination [see Drug Interactions (7.4)]. Periodic CK determinations may be considered in patients starting therapy with or increasing the dose of these agents, but there is no assurance that such monitoring will prevent myopathy.
Cases of myopathy, including rhabdomyolysis, have been observed with simvastatin coadministered with lipid-modifying doses (≥1 g/day niacin) of niacin-containing products. In an ongoing, double-blind, randomized cardiovascular outcomes trial, an independent safety monitoring committee identified that the incidence of myopathy is higher in Chinese compared with non-Chinese patients taking simvastatin 40 mg coadministered with lipid modifying doses of a niacin-containing product. Caution should be used when prescribing SIMCOR in doses that exceed 1000/20 mg/day to Chinese patients. It is unknown if the risk for myopathy with coadministration of simvastatin with lipid modifying doses of niacin-containing products observed in Chinese patients applies to other Asian patients [see Dosage and Administration (2.3)].
Prescribing recommendations for interacting agents are summarized in TABLE 3[see also Dosage and Administration (2.2), Contraindications (4), Drug Interactions (7), Clinical Pharmacology (12.3)].
This image is provided by the National Library of Medicine.
SIMCOR
Myopathy and/or rhabdomyolysis have been reported when simvastatin is used in combination with lipid-altering doses (≥ 1 gram/day) of niacin. Physicians contemplating the use of SIMCOR, a combination of simvastatin and niacin extended-release (NIASPAN), should weigh the potential benefits and risks, and should carefully monitor for any signs and symptoms of muscle pain, tenderness, or weakness, particularly during the initial month of treatment or during any period of upward dosage titration of either drug. Periodic determination of serum creatine kinase (CK) determinations may be considered in such situations, but there is no assurance that such monitoring will prevent myopathy.
Patients starting therapy with SIMCOR should be advised of the risk of myopathy, and told to report promptly unexplained muscle pain, tenderness, or weakness. A CK level above ten times the upper limit of normal (ULN) in a patient with unexplained muscle symptoms indicates myopathy. SIMCOR therapy should be discontinued if myopathy is diagnosed or suspected.
In patients with complicated medical histories predisposing to rhabdomyolysis, such as renal insufficiency, dose escalation requires caution. Also, as there are no known adverse consequences of brief interruption of therapy, treatment with SIMCOR should be stopped for a few days before elective major surgery and when any major acute medical or surgical condition supervenes (e.g., sepsis, hypotension, dehydration, major surgery, trauma, severe metabolic, endocrine, and electrolyte disorders, or uncontrolled seizures).
5.3 Liver Dysfunction
Cases of severe hepatic toxicity, including fulminant hepatic necrosis, have occurred in patients who have substituted sustained-release (modified-release, timed-release) niacin products for immediate-release (crystalline) niacin at equivalent doses. Patients previously receiving niacin products other than niacin extended-release (NIASPAN) should be started on SIMCOR at the lowest recommended starting dose [see Dosage and Administration (2)].
SIMCOR should be used with caution in patients who consume substantial quantities of alcohol and/or have a past history of liver disease. Active liver disease or unexplained transaminase elevations are contraindications to the use of SIMCOR [see Contraindications (4)].
Niacin extended-release (NIASPAN) and simvastatin can cause abnormal liver tests. In a simvastatin-controlled, 24 week study with SIMCOR in 641 patients, there were no persistent increases (to more than 3x the ULN) in serum transaminases. In three placebo-controlled clinical studies of niacin extended-release, patients with normal serum transaminases levels at baseline did not experience any transaminase elevations greater than 3x the ULN. Persistent increases (to more than 3x the ULN) in serum transaminases have occurred in approximately 1% of patients who received simvastatin in clinical studies. When drug treatment was interrupted or discontinued in these patients, the transaminases levels usually fell slowly to pretreatment levels. The increases were not associated with jaundice or other clinical signs or symptoms. There was no evidence of hypersensitivity.
It is recommended that liver enzyme tests be obtained prior to initiating therapy with SIMCOR and repeated as clinically indicated. There have been rare postmarketing reports of fatal and non-fatal hepatic failure in patients taking statins, including simvastatin. If serious liver injury with clinical symptoms and/or hyperbilirubinemia or jaundice occurs during treatment with SIMCOR, promptly interrupt therapy. If an alternate etiology is not found do not restart SIMCOR. Note that ALT may emanate from muscle, therefore ALT rising with CK may indicate myopathy [see Warnings and Precautions (5.2)].
5.4 Laboratory Abnormalities
Increase in Blood Glucose: Niacin treatment can increase fasting blood glucose. In a simvastatin-controlled, 24-week study with SIMCOR the change from baseline in glycosylated hemoglobin levels was 0.2% for SIMCOR-treated patients and 0.2% for simvastatin-treated patients. Diabetic or potentially diabetic patients should be observed closely during treatment with SIMCOR, particularly during the first few months of therapy. Adjustment of diet and/or hypoglycemic therapy or discontinuation of SIMCOR may be necessary.
Reduction in platelet count: Niacin can reduce platelet count. In a simvastatin-controlled, 24-week study with SIMCOR the mean percent change from baseline for patients treated with 2000/40 mg daily was -5.6%.
Increase in ProthrombinTime (PT): Niacin can cause small increases in PT. In a simvastatin-controlled, 24-week study with SIMCOR this effect was not seen.
Increase in Uric Acid: Elevated uric acid levels have occurred with niacin therapy. In a simvastatin-controlled, 24-week study with SIMCOR this effect was not seen. Nevertheless, in patients predisposed to gout, SIMCOR therapy should be used with caution.
Decrease in Phosphorus: Small dose-related reductions in phosphorous levels were seen in clinical studies with niacin. In a simvastatin-controlled, 24-week study with SIMCOR this effect was not seen.
5.5 Endocrine Function
Increases in HbA1c and fasting serum glucose levels have been reported with HMG-CoA reductase inhibitors, including simvastatin.
Adverse Reactions
Clinical Trials Experience
There is limited information regarding Clinical Trial Experience of Niacin/simvastatin in the drug label.
Body as a Whole
Cardiovascular
Digestive
Endocrine
Hematologic and Lymphatic
Metabolic and Nutritional
Musculoskeletal
Neurologic
Respiratory
Skin and Hypersensitivy Reactions
Special Senses
Urogenital
Miscellaneous
Postmarketing Experience
There is limited information regarding Postmarketing Experience of Niacin/simvastatin in the drug label.

{kind=link}