Musculoskeletal problems of the wrist and hand
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Anatomy
-

Right Human Posterior Distal Radius, Ulna, Carpals
-

Right Human Anterior Distal Radius, Ulna, Carpals
-
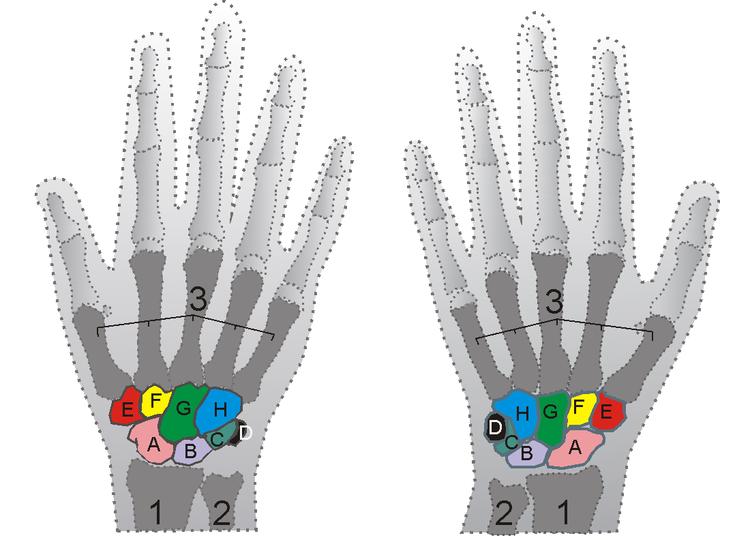
Carpus



-
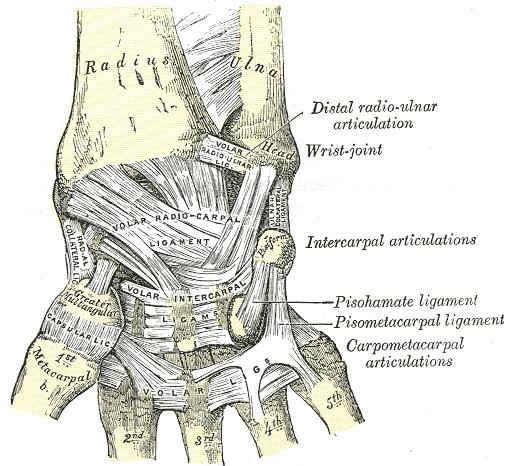
Ligaments of wrist. Anterior view
-
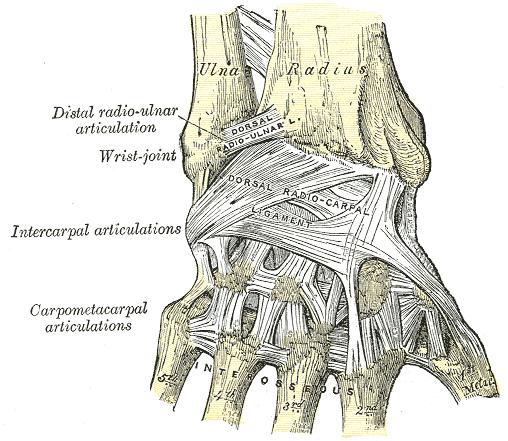
Ligaments of wrist. Posterior view.


Bones
- Distal Radius
- Styloid process adds medial stability
- Distal Ulna
- Styloid process adds lateral stability
- Proximal Carpal Row
- Distal Carpal Row
- Joint Capsules
- Seven non-communicating compartments of the wrist
- Negative findings in one compartment do not rule out pathology in another
Tendons
- Flexor Tendons
- Majority traverse palmar surface via carpal tunnel
- Lie between carpal bones dorsally and flexor retinaculum ventrally
- Extensor Tendons
- Cross the wrist covered by fascia along the dorsal surface
- Insertions
- Major wrist flexors/extensors insert at base of metacarpals, not onto carpal bones
Nerves
- Median Nerve
- Runs through carpal tunnel
- Ulnar Nerve
- Follows ulnar artery
Diagnosis
History and Symptoms
Painful Movement
- Dorsal Wrist Pain
- Most common complaint
- Traumatic Injury
- Distal Radial Fracture
- After fall on outstretched arm (Colles’ fracture)
- Common in young & in elderly with osteoporosis
- Scaphoid Fracture
- Most common bony injury
- Tenderness in anatomic snuff box
- Need scaphoid view +/- follow up films at 2 weeks to detect
- Poor blood supply--risk nonunion, avascular necrosis
- Perilunate Dislocation
- After fall on outstretched, extended wrist
- Dorsal shift of all bones due to severe ligament injury
- Only lunate remains articulated with radius
- X-ray with increased interosseous scaphoid-lunate distance
- Simple Sprain
- Injury to supporting ligaments of radiocarpal joint
- Mild pain or stiffness
- Normal range of motion (ROM) or <10% loss of flexion/extension
- Resolves within 2 weeks with conservative therapy
- Distal Radial Fracture
- Atraumatic
- Radiocarpal arthritis
- Unilateral usually due to prior trauma--secondary oseoarthritis (OA)
- Uncommon site for primary OA
- Bilateral arthritis likely due to RA or crystals
- Wrist more common site for pseudogout than gout
- Septic arthritis of wrist rare
- Pain, swelling and reduced ROM of wrist
- Radiocarpal arthritis
- Radial Wrist Pain and Grip Weakness
- DeQuervain’s Tenosynovitis
- Abductor pollicis longus and extensor pollicis (snuffbox) tendons
- Pain worst over distal radial styloid
- Pain worsened by activity, relieved by rest; history wrist/hand overuse
- CMC Arthritis
- Common, due to repetitive gripping/grasping or vibration exposure
- Wear and tear of articular cartilage at base of thumb
- Pain and swelling at base of thumb
- Gamekeeper’s Thumb
- Disruption of the ulnar collateral ligament of the MP joint
- Due to trauma (ski pole injuries) or repetitive use
- Instability of metacarpal (MP) joint, loss of pinch/opposition function/strength
- Pain and swelling on ulnar side of MP joint
- Late degenerative arthritic change
- Osteonecrosis
- Usually involves scaphoid and lunate, history trauma in 50%
- Reduced wrist flexion/extension, decreased grip strength
- Most severe tenderness over anatomical snuff box
- Can take 4-8 weeks for X-rays to show lesion; bone scan shows earlier
- DeQuervain’s Tenosynovitis
Dorsal Swelling
- Localized
- Ganglion Cyst
- Painless abnormal accumulation of synovial or tenosynovial fluid
- Due to subtle abnormalities in wrist or extensor tendon sheath
- Overproduction of fluid irritates scar tissue and causes cyst formation
- Small % of patients have pain due to cyst pressure on tendons/radial nerve
- +/- Paresthesias over back of hand/fingers (pressure on superficial radial nerve)
- Ganglion Cyst
- Diffuse
- Extensor Tenosynovitis
- Swelling from wrist to back of hand
- Pain aggravated by movement of fingers
- Extensor Tenosynovitis
Stiffness
- Rheumatoid Arthritis (RA)
- Symmetrical joint symptoms with morning stiffness
- Carpal Tunnel Syndrome (CTS)
- Can have stiffness as prominent feature
Sensory Changes with Wrist Use
- Carpal Tunnel Syndrome
- Compression neuropathy of the median nerve at the carpal ligament
- Loss of sensation at the tips of the first 3 fingers
- Grip weakness, pain at wrist +/- radiation to fingers or forearm
- Pain may awaken patient at night; may be relieved with wrist motion
- Usually idiopathic
- Can be due to reduced space in tunnel
- Tenosynovitis / inflammatory arthritis
- Acromegaly
- Pregnancy (3rd trimester)
- Hypothyroidism
- Chronic renal failure
- Amyloidosis
- Can be due to increased susceptibility to pressure
- Diabetes mellitus (DM)
- Vasculitis
- Hereditary neuropathy
Physical Examination
Wrist Function
- Range of Motion
- Radiocarpal joint flexion and extension
- Normal: flexion 90°, extension 80°
- Mild pain/stiffness + normal ROM: sprain or mild arthritis
- Moderate pain/stiffness + 20% loss ROM: arthritis
- Severe pain/stiffness + 50% loss ROM: acute gout, fracture (navicular/distal radius), dislocation
- Refusal to move: septic joint, fracture
- Loss of ROM in only one direction (due to pain)
- Tendon injury or inflammation
- Pain with passive stretching of tendon (opposite direction)
- Grip Strength
- Indirect measure of strength/integrity of forearm muscles
- Can be measured objectively using rolled up partly inflated blood pressure (BP) cuff (patient grip measured in mmHg)
- Reduced Grip Strength
- Disuse atrophy, arthritis (hand or wrist), CTS, DeQuervain’s, osteonecrosis
- May also be reduced in C8 radiculopathy, severe epicondylitis
Specific Maneuvers
- Palpation of the Radiocarpal Joint Line
- Junction of distal radius, scaphoid & lunate
- At intersection of index finger extensor tendon & distal radius
- Mild tenderness: simple sprain
- Moderate tenderness: osteoarthritis (OA)
- Severe pain: crystal-induced arthritis, Colles’ fracture, scaphoid fracture, perilunate dislocation
- Swelling: mild swelling will fill the depression over the navicular (severe swelling causes a bulge)
- Loss of ROM: significant loss (45° flexion / extension) with advanced disease
- Palpation of the Scaphoid Bone
- Scaphoid forms floor of anatomical snuff box (distal radial styloid + base of thumb + abductor pollicis longus + extensor pollicis longus)
- Tenderness in anatomical snuff box = scaphoid pathology (fracture, osteonecrosis, arthritis)
- Palpation of the Radial Styloid
- Pain suggests DeQuervain’s tenosynovitis (friction-induced irritation of anatomic snuffbox tendons)
- Confirmatory Testing
- Pain aggravated by thumb extension or abduction against resistance
- (Abduction = movement of thumb perpendicular to palm)
- Pain worse with passive stretch of tendons over radial styloid via thumb flexion
- (Finkelstein’s test)
- Pain aggravated by thumb extension or abduction against resistance
- Compression of the Base of Thumb
- Screen for CMC arthritis (or strain)
- Pain with compression of the CMC joint in the ante partum (AP) plane suggests CMC arthritis
- Pressure applied from the snuffbox is much less painful
- Swelling best seen with wrist turned radial-side-up
- Crepitation with forcible rotation of metacarpal against trapezium (mortar & pestle sign)
- Bony protuberance of metacarpal or thenar atrophy: late stages
- Palpation of Metocarpophalangeal Joint
- Detect gamekeeper’s thumb (ulnar collateral ligament injury)
- Local tenderness/swelling along ulnar side of MP joint suggests diagnosis
- Instability or pain of MP joint with valgus stress (examiner’s thumb at MP joint, index finger at interphalangeal (IP) joint)
- Loss of MP flexion (normal = 90°) and pinch strength can occur with acute symptoms/swelling
- Tests for Nerve Compression
- CTS
- Sensory loss in the first 3 fingertips: two-point discrimination, light touch, pain decreased
- Weakness of thumb opposition: best detected when pt holds thumb + 5th finger together
- Tinel Sign
- Vigorous tapping over transverse carpal ligament with wrist in extension
- Positive if reproduces pain and paresthesia
- Phalen Sign
- Both wrists held in extreme volar flexion for 30-60 seconds
- Positive if symptoms reproduced
- Pronator Teres Compression
- If no compression detected at wrist, test for proximal compression
- Apply pressure to forearm 1 to 2 inches distal to antecubital fossa
- Positive if symptoms reproduced with compression
- Sensitivity increased by resisting forearm pronation
- Note: Tests can be totally normal despite significant compression (symptoms vary over time)
- Sensitivity and specificity of provocative tests low
- Transillumination
- Distinguishes between ganglion (transilluminates) and solid mass
- Ganglion cyst should be highly mobile and fluctuant, not adherent; ROM should be full
- Aspiration of cyst yields thick, colorless fluid
X-Ray
- Plain X-Rays
- Indicated if suspected arthritis (radiocarpal, CMC) or fracture
- Usual views = Posteroanterior (PA), PA oblique, lateral
- PA ulnar deviation views views needed for suspected scaphoid fracture; may be negative for 1-2 weeks
- X-rays should be normal if:
- Simple sprain
- CMC strain (vs. CMC OA—abnormal films)
- DeQuervain’s – films not indicated
- Gamekeeper’s thumb – films not indicated
- Carpal tunnel syndrome – films not indicated
- Dorsal ganglion – films not indicated
Aspiration
- Wrist Joint
- If infection or inflammatory or crystal-induced arthritis suspected
- Dorsal Ganglion
- Confirms diagnosis (thick, clear, gelatinous fluid)
Nerve Conduction Studies
- Indicated if suspected median nerve compression
- Nerve conduction velocity (NCV) decreased in 70% of cases; high PPV, but sensitivity low
Positive Median Nerve Block/or Steroid Injection
- Can be used to confirm suspected diagnosis of CTS
- Simultaneous steroid injection is therapeutic as well as diagnostic
- Significant risk complications (nerve atrophy or necrosis): should only be performed by an expert
Differential Diagnosis
Traumatic Injury
- Fracture
- Immediate severe pain and swelling
- Colle’s fracture
- Fracture of distal radius; most common, easily seen on X-ray
- Scaphoid Fracture
- May require special X-ray views to visualize
- Ligament Rupture or Tear
- Tendon Injury
Nontraumatic
- Inflammatory Arthritis
- Septic, crystal-induced, rheumatoid arthritis (RA)
- Pain with movement of wrist through its range of motion
- Synovitis with swelling in setting of inflammatory entities
- Osteoarthritis
- Rarely involves wrist except for carpometacarpal (CMC) joint at base of thumb
- Osteonecrosis (avascular)
- Localized pain interfering with hand/wrist function
- Entrapment Syndromes
- Wrist pain radiating into hand or forearm, +/- sensory or motor deficits
- Carpal tunnel syndrome
- Ulnar or interosseous nerve entrapment
- Tenosynovitis
- Ganglion Cyst
- Referred Pain from Cervical-Spine/Shoulder
- Pain in absence of local findings
- Symptoms worsened by neck/shoulder movement
Management
Acute Trauma
- Assess ligamentous, vascular, neurologic integrity
- X-Rays
- If fracture suspected
- Scaphoid views if tenderness in anatomic snuff box
- If no fracture
- Rest, ice, splint as below; nonsteriodal anti-inflammatory drugs (NSAIDs)
- If pain persists, repeat X-rays after 2 weeks to detect fracture not seen on initial films
Empiric Treatment for Mild-Moderate Wrist Pain with Normal ROM
- Neutral position
- Avoidance of extremes of movement
- Can use veclro wrist splint to immobilize in neutral position
- Restriction of repetitive gripping/grasping and exposure to vibration
- Restriction of lifting to less than 10 pounds
- Ice: to dorsal surface of wrist for 15 minutes up to three times a day
- Stretching: passive stretching in flexion and extension
- If persistent symptoms (or if traumatic injury, moderate to severe pain or decreased ROM or grip strength), further evaluation +/- X-rays needed
Specific Treatment for Various Syndromes
- Radiocarpal Arthritis
- Mild: ice and Velcro wrist immobilizer with metal stay; NSAIDs x 3-4 weeks
- Moderate to severe: local steroid injection
- Crystal-induced: usual treatment for gout vs. pseudogout
- Start flexion/extension passive ROM exercises once acute symptoms controlled
- Gripping and wrist extension toning exercises after flare resolves
- If persistent symptoms at 3 months with loss of >50% of ROM, refer to orthopaedist
- DeQuervain’s Tenosynovitis
- Ice to radial styloid
- Restriction of thumb gripping/grasping
- Buddy-tape thumb to 1st finger
- Treat with dorsal hood splint
- Treat with Velcro thumb spica splint
- If persistent symptoms at 3-4 weeks, prescribe steroid injection
- 3/8” proximal to tip of radial styloid
- 25 gauge needle
- Depo-Medrol 80 mg/mL, ½ mL
- 2-3 mL anesthetic (lido)
- May repeat at 4-6 weeks if symptoms persist
- Once symptoms improved (3-4 weeks), gentle passive stretching exercises of thumb abductor and extensor tendons into the palm (20 stretches every day, each held for 5 seconds)
- CMC Arthritis
- Rest + NSAIDs (x 3-4 weeks) + restriction of gripping/grasping
- Oversized tools and grips
- Overlap-taping of joint, or
- Dorsal hood splint, or
- Velcro thumb spica spliint
- If symptoms persist at 3-4 weeks, prescribe steroid injection
- 3/8” proximal to base of metacarpal bone
- 25 gauge needle
- Adjacent to abductor tendon in snuffbox
- ½ mL anesthetic + ½ mL Depo-Medrol 40 mg/mL
- Repeat at 4-6 weeks if symptoms not reduced by 50%
- Once pain improved, passive stretching of thumb flexors/extensors
- Rest + NSAIDs (x 3-4 weeks) + restriction of gripping/grasping
- Gamekeeper’s Thumb
- Ice to MP joint + immobilization with overlap taping, dorsal hood splint or thumb spica splint
- Complete rest needed for 3-6 weeks to allow ligament healing/reattachment
- Once recovered
- Passive ROM flexion/extension exercises of thumb
- Isometric toning of thumb flexion (squeeze tennis ball x 5 sec, repeat 20-25 times)
- Ganglion Cyst
- Reassurance: may resolve spontaneously
- If persistent, aspirate cyst (note: 18 gauge needle needed; anesthetize via 25 gauge needle first)
- Limit repetitive wrist motions; consider Velcro wrist brace
- If recurrence after aspiration, repeat aspiration and inject Depo-Medrol 40 mg/mL
- If further recurrences, consider ortho referral for removal, though may recur even after excision
- Carpal Tunnel Syndrome
- Treat any underlying cause (diuretics, antiinflammatories, L-T4, etc.)
- Reduce repetitive wrist motion: occupational adjustments
- Velcro wrist splint at night (or day and night if severe sxs)
- Consider referral for steroid injection or surgery if inadequate symptom improvement
- Note: 90% respond to steroid injection; surgery may be avoidable with physical therapy (PT) + steroid injection
- Once symptoms improved (3-4 weeks after pain resolved), passive stretching exercises for flexor tendons