Kidney stone classification scheme
|
Kidney stone Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Kidney stone classification scheme On the Web |
|
American Roentgen Ray Society Images of Kidney stone classification scheme |
|
Risk calculators and risk factors for Kidney stone classification scheme |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Classification
85% of renal stones are made of calcium oxalate.
Calcium Oxalate Stones
The most common type of kidney stone is composed of calcium oxalate crystals, and factors that promote the precipitation of crystals in the urine are associated with the development of these stones.
Conventional wisdom and common sense have long held that consumption of too much calcium could promote the development of calcium kidney stones. However, current evidence suggests that the consumption of low-calcium diets is actually associated with a higher overall risk for the development of kidney stones. This is perhaps related to the role of calcium in binding ingested oxalate in the gastrointestinal tract. As the amount of calcium intake decreases, the amount of oxalate available for absorption into the bloodstream increases; this oxalate is then excreted in greater amounts into the urine by the kidneys. In the urine, oxalate is a very strong promoter of calcium oxalate precipitation, about 15 times stronger than calcium.
Other Types
Other types of kidney stones are composed of struvite (magnesium, ammonium and phosphate); uric acid; calcium phosphate; and cystine.
- The formation of struvite stones is associated with the presence of urea-splitting bacteria, most commonly Proteus mirabilis (but also Klebsiella, Serratia, Providencia species). These organisms are capable of splitting urea into ammonia, decreasing the acidity of the urine and resulting in favorable conditions for the formation of struvite stones. Stuvite stones are always associated with urinary tract infections.
- The formation of uric acid stones is associated with conditions that cause high blood uric acid levels, such as gout, leukemias/lymphomas treated by chemotherapy (secondary gout from the death of leukemic cells), and acid/base metabolism disorders where the urine is excessively acid resulting in uric acid precipitation.
- The formation of calcium phosphate stones is associated with conditions such as hyperparathyroidism and renal tubular acidosis.
- The formation of cystine stones is uniquely associated with people suffering from cystinuria, who accumulate cystine in their urine.
-
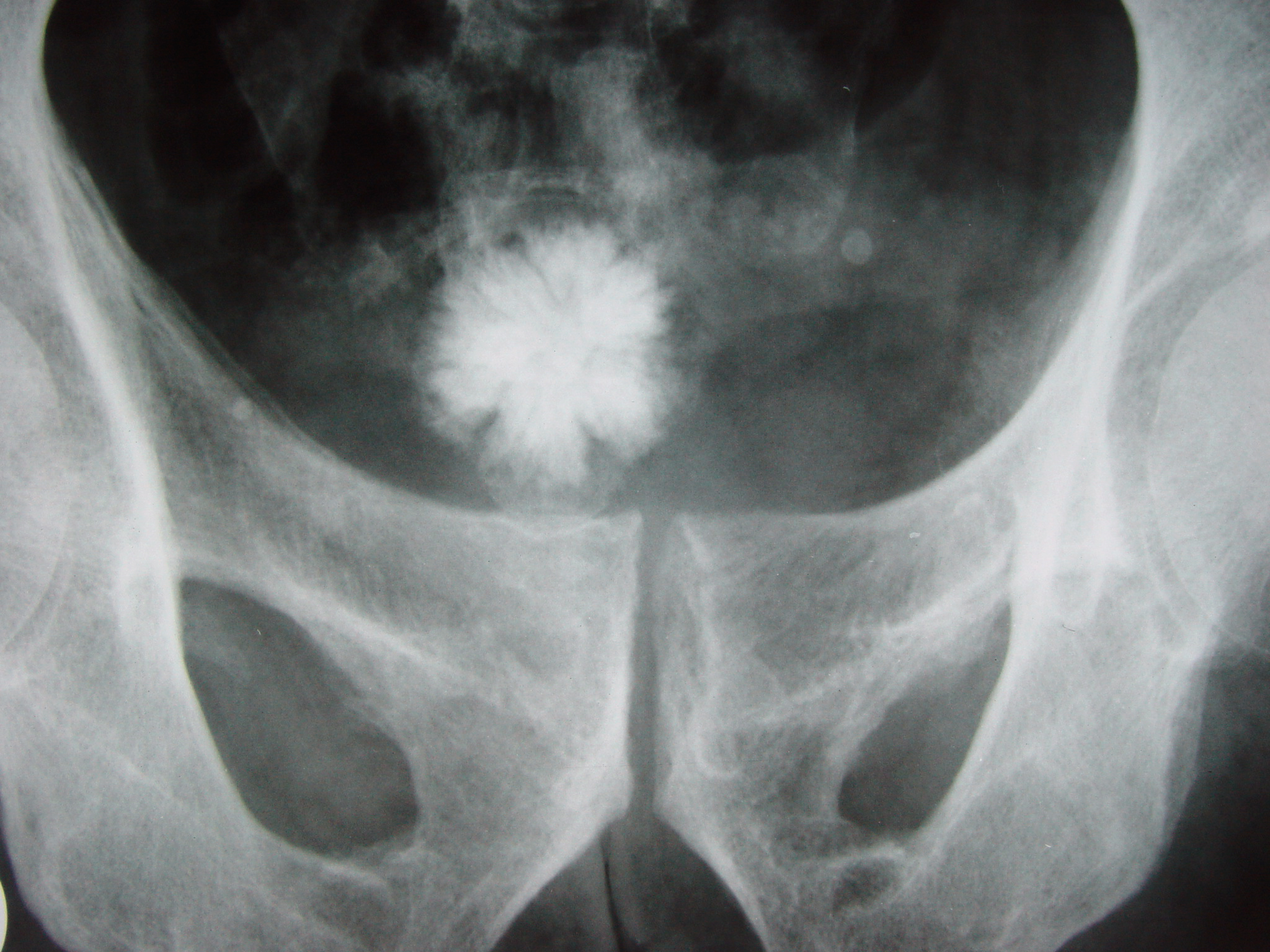
Star shaped bladder urolith
-

Staghorn calculus (struvite stone)

