Fungal meningitis laboratory findings: Difference between revisions
Prince Djan (talk | contribs) |
Prince Djan (talk | contribs) |
||
| Line 57: | Line 57: | ||
Histoplasma_capsulatum.jpg|Histoplama capsulatum | Histoplasma_capsulatum.jpg|Histoplama capsulatum | ||
</gallery> | </gallery> | ||
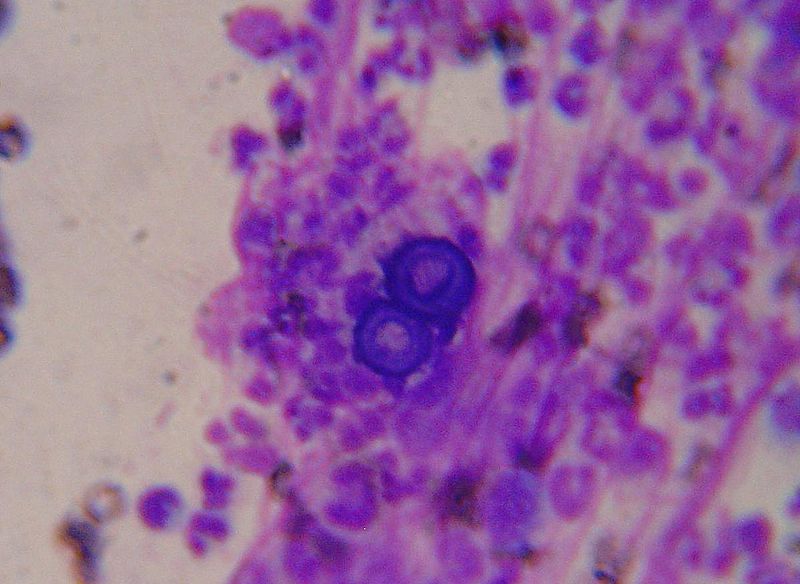
====Cryptococcosis (PAS stain)==== | |||
{{#ev:youtube|ZG0AcmtBLe4}} | |||
==References== | ==References== | ||
Revision as of 16:24, 13 February 2017
|
Fungal meningitis Microchapters |
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Fungal meningitis laboratory findings On the Web |
|
American Roentgen Ray Society Images of Fungal meningitis laboratory findings |
|
Risk calculators and risk factors for Fungal meningitis laboratory findings |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Rim Halaby; Prince Tano Djan, BSc, MBChB [2]
Overview
A lumbar puncture is essential for the diagnosis of fungal meningitis and initiation of the appropriate treatment. The cerebrospinal fluid (CSF) of a patient having bacterial meningitis is distinguished by the presence of lymphocytosis, low glucose level and high proteins level. Specific CSF stains and cultures as well as serologies help in determining the specific nature of the causative fungi.
Biopsy of skin lesions, chest radiography, ophthalmologic examination, computed tomography or MRI of the brain, in addition to cultures of CSF, blood, and sputum, may provide essential diagnostic clues.
Laboratory Findings
The General Characteristic CSF Findings in Fungal Meningitis:
Analysis of the CSF in suspected fungal meningitis should include:[1][2][3][4]
- Opening pressure measurement
This has prognostic and therapeutic value especially in cryptococcal meningitis although it is not commonly done or recorded.
- Cell count with differential,
Most patients have mononuclear pleocytosis in the range of 20 to 500 cells/mm3 however some patients have polymorphonuclear neutrophils as the predominant cell type in caese os aspergillosis and eosinophilia when Cryptococcus immitis is suspected[1][2] In patients who are immunosuppressed, the cell count may be markedly decreased to less than 20 cells/mm3.
- Glucose concentration
Glucose concentrations are usually decreased by may vary depending on the clinical state of the patient.
- Protein concentrations
CSF protein levels are usually increased
- Gram’s stain,
- India ink,
- Culture.
Other CSF Findings and Serology Tests Specific to Each Particular Fungi
- Aspergillus spp.
- CSF culture may grow Aspergillus fumigatus complex or may be sterile[5]
- Gomori-Grocott staining may reveale hyaline septate hyphae[5]
- Baseline serum and CSF 1,3-β-d-glucan (BDG) measurements are positive whereas serum and CSF galactomannan (GM) antigen test results are negative in an Aspergillus fumigatus-specific PCR assay.[5]
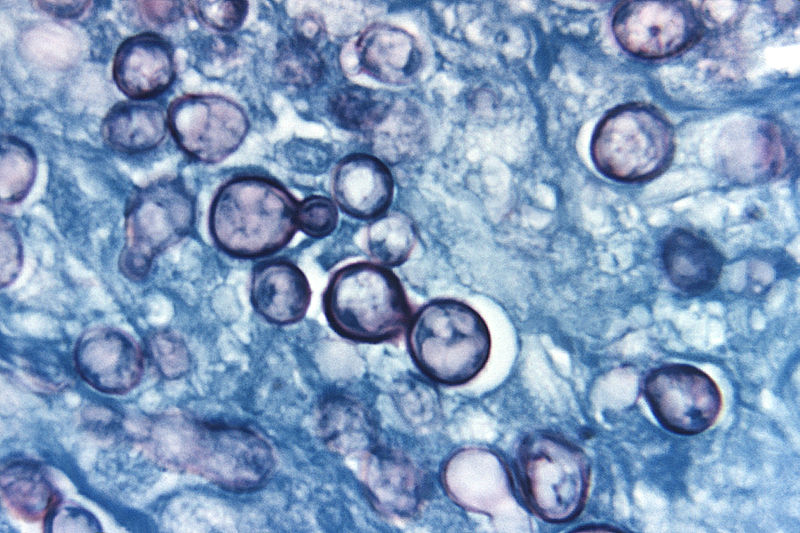
- Blastomyces dermatitidis
- Fungal stain and culture of CSF
- Biopsy and culture of skin and lung lesions
- Antibody detection in serum
- Cryptococcus neoformans
- India ink or fungal wet mount of CSF (budding yeast)
- Mucicarmine stain provides specific staining of the polysaccharide cell wall
- Blood and urine cultures
- Antigen detection in CSF
- Coccidioides immitis
- Antibody detection in CSF and serum
- Candida sp.
- Fungal stain and culture of CSF
- Histoplasma capsulatum
- Fungal stain and culture of large volumes of CSF
- Antigen detection in CSF, serum, and urine
- Antibody detection in serum and CSF
- Sporothrix schenckii
- Antibody detection in CSF and serum
- CSF culture[6]
Fungal Stains
-
Blastomyces: Broad based budding
-
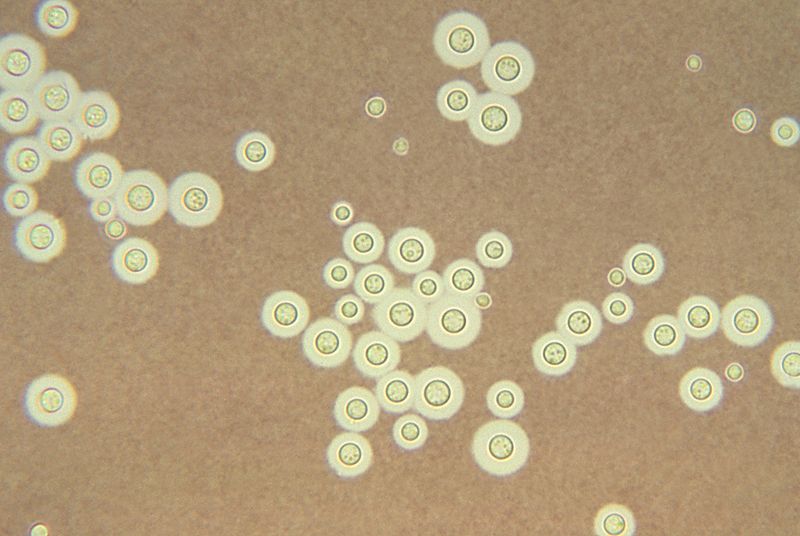
Cryptococcus: clear halo visualized by the india ink stain
-
Histoplama capsulatum



Cryptococcosis (PAS stain)
{{#ev:youtube|ZG0AcmtBLe4}}
References
- ↑ 1.0 1.1 White M, Cirrincione C, Blevins A, Armstrong D (1992). "Cryptococcal meningitis: outcome in patients with AIDS and patients with neoplastic disease". J Infect Dis. 165 (5): 960–3. PMID 1569350.
- ↑ 2.0 2.1 Pettit AC, Kropski JA, Castilho JL, Schmitz JE, Rauch CA, Mobley BC; et al. (2012). "The index case for the fungal meningitis outbreak in the United States". N Engl J Med. 367 (22): 2119–25. doi:10.1056/NEJMoa1212292. PMID 23083311.
- ↑ Gottfredsson M, Perfect JR (2000). "Fungal meningitis". Semin Neurol. 20 (3): 307–22. doi:10.1055/s-2000-9394. PMID 11051295.
- ↑ Banarer M, Cost K, Rychwalski P, Bryant KA (2005). "Chronic lymphocytic meningitis in an adolescent". J Pediatr. 147 (5): 686–90. doi:10.1016/j.jpeds.2005.07.010. PMID 16291364.
- ↑ 5.0 5.1 5.2 Morgand M, Rammaert B, Poirée S, Bougnoux ME, Tran H, Kania R; et al. (2015). "Chronic Invasive Aspergillus Sinusitis and Otitis with Meningeal Extension Successfully Treated with Voriconazole". Antimicrob Agents Chemother. 59 (12): 7857–61. doi:10.1128/AAC.01506-15. PMC 4649149. PMID 26392507.
- ↑ Koroshetz WJ. Chapter 382. Chronic and Recurrent Meningitis. In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, eds. Harrison's Principles of Internal Medicine. 18th ed. New York: McGraw-Hill; 2012.