|
|
| (28 intermediate revisions by 6 users not shown) |
| Line 1: |
Line 1: |
| | '''For patient information click [[{{PAGENAME}} (patient information)|here]]''' |
| {{Infobox_Disease | | | {{Infobox_Disease | |
| Name = {{PAGENAME}} | | | Name = {{PAGENAME}} | |
| Image = 448.jpg|
| |
| Caption = Cor Triatriatum: Gross right atrium tricuspid valve and right ventricle note right ventricular hypertrophy <br> <small> [http://www.peir.net Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] </small> |
| |
| DiseasesDB = 31741 | | | DiseasesDB = 31741 | |
| ICD10 = {{ICD10|Q|24|2|q|20}} | | | ICD10 = {{ICD10|Q|24|2|q|20}} | |
| Line 9: |
Line 8: |
| OMIM = | | | OMIM = | |
| MedlinePlus = | | | MedlinePlus = | |
| eMedicineSubj = ped | | | eMedicineSubj = | |
| eMedicineTopic = 2507 | | | eMedicineTopic = | |
| eMedicine_mult = {{eMedicine2|med|458}} | | | eMedicine_mult = | |
| MeshID = D003310 | | | MeshID = D003310 | |
| }} | | }} |
| {{SI}} | | {{Cor triatriatum}} |
| {{WikiDoc Cardiology Network Infobox}}
| | {{CMG}}; '''Associate Editors-In-Chief:''' [[Priyamvada Singh|Priyamvada Singh, MBBS]] [mailto:psingh13579@gmail.com]; {{CZ}}; [[User:KeriShafer|Keri Shafer, M.D.]] [mailto:kshafer@bidmc.harvard.edu]; [[Sandeep Basnet|Sandeep Basnet, MBBS]]; '''Assistant Editor(s)-In-Chief:''' [[Kristin Feeney|Kristin Feeney, B.S.]] [mailto:kfeeney@elon.edu] |
| {{CMG}} | |
| | |
| '''Associate Editors-In-Chief:''' {{CZ}}; [[User:KeriShafer|Keri Shafer, M.D.]] [mailto:kshafer@bidmc.harvard.edu] | |
| | |
| {{Editor Join}}
| |
|
| |
|
| '''Synonyms:''' Subdivided left atrium, accessory atrium, heart with 3 atria, triatrial heart, cor triatriatum sinister, cor triatriatum sinistrum, cor triatriatum dexter, cor triatriatum dextrum. | | '''Synonyms:''' Subdivided left atrium, accessory atrium, heart with 3 atria, triatrial heart, cor triatriatum sinister, cor triatriatum sinistrum, cor triatriatum dexter, cor triatriatum dextrum. |
|
| |
|
| ==Overview== | | ==[[Cor triatriatum overview|Overview]]== |
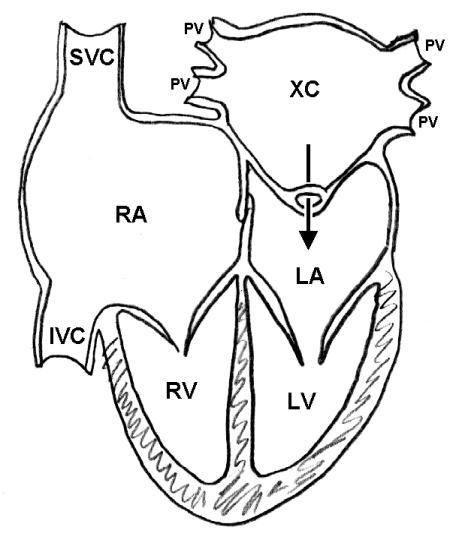
| '''Cor triatriatum''' is a rare [[congenital heart defect]] where a fibromuscular septum subdivides the [[left atrium]] into two chambers. Associated cardiovascular malformations are common and include [[atrial septal defect]] and [[patent ductus arteriosus]]. The proximal or accessory chamber lies posteriorly, and usually receives blood from each of the [[pulmonary vein]]s. The distal or true [[left atrial]] chamber lies anterior, connects to the left atrial appendage, and empties into the [[left ventricle]] through the [[mitral valve]]. The two atrial chambers communicate through an opening in the membrane which divides the two chambers. This opening may be single and stenotic, fenestrated, and either small or large. <ref>[http://radiographics.rsnajnls.org/cgi/reprint/8/6/1227 Jolles H, A case report Volume 8, Number 6 November, 1988 RadioGraphics]</ref>
| |
| | |
| ==Epidemiology and Demographics==
| |
| | |
| The incidence ranges from approximately 0.1% to 0.4% of all infants with congenital heart disease. The male to female ratio is 1.4:1.
| |
| | |
| ==Anatomy==
| |
| The [[pulmonary veins]] enter the proximal [[left atrial]] chamber and are separated from distal left atrial chamber by a diaphragm. A small hole in this diaphragm allows some communication to the distal chamber. The [[right ventricle]] is enlarged. The [[fossa ovalis]] is patent, which allows left-to-right shunting. This interatrial connection usually communicates with the proximal chamber of the [[right atrium]] and occasionally the distal chamber communicates with the [[right atrium]]. The distal chamber contains the [[mitral valve]] and the [[left atrial]] appendage.
| |
| | |
| ==Pathogenesis==
| |
| | |
| ===Cor triatriatum sinistrum===
| |
| ====Malincorporation Theory====
| |
| It has been hypothesized that cor triatriatum sinister occurs when the common [[pulmonary vein]] fails to incorporate the [[pulmonary circulation]] into the [[left atrium]]. As a result, the common pulmonary venous ostium remains narrow. The anatomic result is a septumlike structure that divides the [[left atrium]] into two compartments. However, this theory fails to explain the following:
| |
| #The presence of the [[fossa ovalis]] and atrial muscle fibers within the walls of the proximal chamber where only a venous wall should be present.
| |
| #Furthermore, several cases have been reported in which 1 or 2 [[pulmonary veins]] drain into the proximal (or accessory) chamber and the others drain directly into the true [[left atrium]].
| |
| | |
| ====Malseptation Theory====
| |
| A second alternate hypothesis is that the membrane dividing the [[left atrium]] is an abnormal growth of the [[septum primum]].
| |
| | |
| ====Entrapment Theory====
| |
| A third hypothesis asserts that the right horn of the embryonic [[sinus venosus]] entraps the common [[pulmonary vein]] and thereby prevents its incorporation into the [[left atrium]].
| |
| | |
| The significance of a prominent or persistent left [[superior vena cava]] in the pathogenesis of cor triatriatum is unclear.
| |
|
| |
|
| ===Cor triatriatum dextrum=== | | ==[[Cor triatriatum anatomy|Anatomy]]== |
|
| |
|
| In normal development, the right horn of the [[sinus venosus]] is gradually incorporated into the [[right atrium]]. This forms the smooth posterior portion of the [[right atrium]]. The original embryologic [[right atrium]] ultimately becomes the trabeculated anterior portion of the [[right atrium]].
| | ==[[Cor triatriatum epidemiology and demographics|Epidemiology and demographics]]== |
|
| |
|
| The embryologic [[right atrium]] and the right horn of the [[sinus venosus]] are then connected through the sinoatrial orifice. The sinoatrial orifice is surrounded on either side by the two valvular folds (the right and left venous valves). The [[right atrium]] is divided in two by the right horn of the [[sinus venosus]]. This right valve forms a sheet that serves to direct the oxygenated venous return from the inferior [[vena cava]] across the [[foramen ovale]] to the left side of the heart during fetal life as the Chiari network.
| | ==[[Cor triatriatum natural history|Natural history, Complications, and Prognosis]]== |
|
| |
|
| Normally, this network regresses and leaves behind the [[crista terminalis]] superiorly and the [[eustachian valve]] of the [[inferior vena cava]] and the [[thebesian valve]] of the [[coronary sinus]] inferiorly.
| | ==[[Cor triatriatum causes|Causes]]== |
|
| |
|
| Complete persistence of the right sinus valve of embryonic life results in separation of the smooth and trabeculated portions of the right atrium and constitutes cor triatriatum dextrum. If this membrane is extensively fenestrated and weblike in appearance, then it is referred to as the Chiari network.
| | ==[[Cor triatriatum differential diagnosis|Differentiating Cor triatriatum from other Disorders]]== |
|
| |
|
| ==Diagnosis== | | ==Diagnosis== |
| ==Symptoms==
| |
| The severity of symptoms depends upon the size of the hole in the diaphragm separating the two atrial chambers and the integrity of the interatrial septum. Pulmonary venous hypertension develops in infancy. Signs and symptoms of low [[cardiac output]], [[pallor]], [[tachypnea]], and growth failure. If there is an associated [[PFO]] or [[ASD]] then this may decompress the pressure in the [[pulmonary vein]]s by diverting blood into the [[right atrium]]. If the [[ASD]] is located superior to the [[diaphragm]], there will be a large shunt. In contrast, if the [[ASD]] is located below the [[diaphragm]], the signs and symptoms may be similar to [[mitral stenosis]].
| |
|
| |
| ===Physical Examination===
| |
| Again, the findings on physical examination depends upon the size of the hole in the diaphragm separating the two atrial chambers and the integrity of the interatrial septum.
| |
|
| |
| ===Electrocardiogram===
| |
| The EKG findings in cor triatriatum are nonspecific and variable, but [[right axis deviation]] with [[right atrial enlargement]] and [[right ventricular hypertrophy]] may be present.
| |
|
| |
| ===Chest x-ray===
| |
| * When cor triatriatum occurs as an isolated defect, the hemodynamic derangement is identical to that of [[mitral stenosis]] and the chest radiography shows a normal sized heart with changes of chronic interstitial edema.
| |
| * Findings are usually nonspecific but may include pulmonary congestion with diffuse haziness or Kerley B lines and the ground glass pattern of acute pulmonary edema in hilar areas.
| |
| * Patients may have mild cardiac enlargement and prominence of the pulmonary arterial segment.
| |
| * The dilated proximal chamber may produce the appearance of left atrial enlargement.
| |
| * Presence of an atrial septal defect or of an associated partial anomalous pulmonary venous connection adds pulmonary overcirculation to the pulmonary venous obstruction. The radiograph may then show significant right ventricular enlargement.
| |
|
| |
| ===Echocardiography===
| |
| Echocardiography is the diagnostic imaging modality of choice and easily identifies a diaphragm dividing the [[left atrial]] chambers and can also identify the presence of an associated [[atrial septal defect]]. It is also very important to identify the origin of each of the [[pulmonary veins]] to exclude the presence of anomalous pulmonary venous return which may coexist with the disorder. Cor triatriatum may indeed be difficult to distinguish from a [[total anomalous pulmonary venous connection]] to the [[coronary sinus]].
| |
|
| |
| ====Echocardiographic differentiation between cor triatriatum and supravalvular mitral ring:====
| |
| A cor triatriatum membrane tends to:
| |
| #Be more curved.
| |
| #Moves toward the [[mitral valve]] plane in diastole
| |
| #All pulmonary veins drain proximal to the membrane
| |
| #The [[left atrial]] appendage and the [[foramen ovale]] are distal to the membrane
| |
|
| |
|
| A supramitral ring tends to:
| |
| #Attach to the base of the [[mitral valve]] past the [[left atrial]] appendage and past the [[foramen ovale]]
| |
| #Move away from the [[mitral valve]] in diastole
| |
| #Be associated with abnormal mitral leaflet motion and a prolonged Doppler pressure half time
| |
|
| |
|
| ===[[Cardiac catheterization]]===
| | [[Cor triatriatum history and symptoms|History and Symptoms]] | [[Cor triatriatum physical examination|Physical Examination]] | [[Cor triatriatum laboratory tests|Laboratory Tests]] | [[Cor triatriatum electrocardiogram | Electrocardiogram]] | [[Cor triatriatum chest x ray|Chest X Ray]] | [[Cor triatriatum MRI|MRI]] | [[Cor triatriatum CT|CT]] | [[Cor triatriatum echocardiography|Echocardiography]] | [[Cor triatriatum other imaging findings|Other Imaging Findings]] | [[Cor triatriatum other diagnostic studies|Other Diagnostic Studies]] |
| *Generally indicated to assess pulmonary venous return and pulmonary arterial pressures. Approximately 10% of patients have partial anomalous venous return, and angiography is helpful in defining the precise venous anatomy.
| |
| *Catheterization generally reveals [[pulmonary hypertension]] in a degree that varies directly with the severity of obstruction to pulmonary venous drainage. Demonstration of a pressure gradient between the left atrium and capillary wedge pressure is an important finding.
| |
| *The proximal chamber is visualized during the venous phase, and a delay then occurs before the true left atrium and left ventricle are visualized. The proximal chamber then remains opacified and does not contract with the distal chamber.
| |
| | |
| ==Differential Diagnosis of Cor Triatriatum==
| |
| | |
| * [[Mitral Stenosis]] (Supravalvular Ring)
| |
| * Partial Anomaly of Pulmonary Venous Connection
| |
| * Idiopathic [[Pulmonary Hypertension]]
| |
| * Persistent [[Pulmonary Hypertension]] in newborn
| |
| * Pulmonary Hypoplasia
| |
| * [[Total Anomalous Pulmonary Venous Connection]]
| |
| | |
| ==Prognosis==
| |
| | |
| Cor triatriatum is usually fatal within the first two years of life. The prognosis is related to timely surgical intervention, the degree of obstruction between the two left atria, and the presence or absence of associated anomalies. The majority of postoperative deaths occur in the first 30 days. | |
| | |
| Long-term results are excellent, with survival of more than 80% in patients surviving surgery.
| |
| | |
| Survivors have excellent functional results without residual sequelae and a life expectancy that approaches the general population.
| |
|
| |
|
| ==Treatment== | | ==Treatment== |
|
| |
|
| * Medical therapy is primarily supportive to manage pulmonary venous congestion until surgical resection can be performed.
| | '''Medical:''' [[Cor triatriatum medical therapy|Medical Therapy]] |
| * The role of percutaneous balloon dilation in managing this condition remains to be determined.
| |
| * It can be treated surgically by removing the membrane dividing the atrium.
| |
| | |
| A. '''Left atrial approach'''
| |
| *Better if the patient is older, and defect is larger
| |
| *Excise the obstructing diaphragm
| |
| *Enlarge the left atrium as needed and close the interatrial connection
| |
| | |
| B. '''Right atrial approach'''
| |
| *Better if the patient is younger, and defect is smaller
| |
| *Locate the diaphragm through the [[ASD]]
| |
| *Excise the obstructing diaphragm
| |
| *Close the [[ASD]]
| |
|
| |
|
| ==Images==
| | '''Surgical:''' [[Cor triatriatum surgery|Surgery]] |
| Images shown below are courtesy of Professor Peter Anderson DVM PhD and Published with permission [http://www.peir.net © PEIR, University of Alabama at Birmingham, Department of Pathology]
| |
|
| |
|
| <div align="left">
| | [[Cor triatriatum primary prevention|Primary Prevention]] | [[Cor triatriatum secondary prevention|Secondary Prevention]] | [[Cor triatriatum cost-effectiveness of therapy|Cost-Effectiveness of Therapy]] | [[Cor triatriatum future or investigational therapies|Future or Investigational Therapies]] |
| <gallery heights="175" widths="175">
| |
| Image:445.jpg|Cor Triatriatum: Gross left ventricular outflow tract appears normal
| |
| Image:Cor Triatriatum 446.jpg|Cor Triatriatum: Gross left atrial inlet chamber with probe extending through narrow connection to true left atrium below
| |
| </gallery>
| |
| </div>
| |
| | |
| | |
| <div align="left">
| |
| <gallery heights="175" widths="175">
| |
| Image:448.jpg|Cor Triatriatum: Gross right atrium tricuspid valve and right ventricle note right ventricular hypertrophy
| |
| Image:1477.jpg|Cor Triatriatum: Gross
| |
| </gallery>
| |
| </div>
| |
| | |
| | |
| <div align="left">
| |
| <gallery heights="175" widths="175">
| |
| Image:8612.jpg|Cor Triatriatum: Gross fixed tissue opened left atrium mitral valve and left ventricle
| |
| Image:8597.jpg|Lung: Abnormal Lobation: Gross fixed tissue posterior view both lungs with many lobes case of cor triatriatum
| |
| </gallery>
| |
| </div>
| |
| | |
| | |
| <div align="left">
| |
| <gallery heights="175" widths="175">
| |
| Image:5863.jpg|Cor Triatriatum: Gross fixed tissue opened superior atrial chamber
| |
| Image:5862.jpg|Cor Triatriatum: Gross fixed tissue opened infant heart with the two chambered left atrium
| |
| </gallery>
| |
| </div>
| |
|
| |
|
| ==References== | | ==References== |
| {{Reflist}} | | {{reflist|2}} |
| | |
| ==Additional Reading==
| |
| | |
| * Moss and Adams' Heart Disease in Infants, Children, and Adolescents Hugh D. Allen, Arthur J. Moss, David J. Driscoll, Forrest H. Adams, Timothy F. Feltes, Robert E. Shaddy, 2007 ISBN 0781786843
| |
|
| |
|
| ==External Links== | | ==External Links== |
| | * [http://www.nejm.org/doi/full/10.1056/NEJMicm990415/ Images in Clinical Medicine] in NEJM, 2004 |
| * [http://info.med.yale.edu/intmed/cardio/chd/e_cor_triat/ Image] at Yale University | | * [http://info.med.yale.edu/intmed/cardio/chd/e_cor_triat/ Image] at Yale University |
| * [http://www.hawaii.edu/medicine/pediatrics/pemxray/v4c03d.jpg Diagram] at University of Hawaii | | * [http://www.hawaii.edu/medicine/pediatrics/pemxray/v4c03d.jpg Diagram] at University of Hawaii |
| Line 182: |
Line 57: |
| * [http://escuela.med.puc.cl/paginas/Cursos/tercero/AnatomiaPatologica/Imagenes_AP/fotos001-010/010.jpg Cor triatriatum sinistrum: A pathomorphological image] | | * [http://escuela.med.puc.cl/paginas/Cursos/tercero/AnatomiaPatologica/Imagenes_AP/fotos001-010/010.jpg Cor triatriatum sinistrum: A pathomorphological image] |
| * [http://www.cardioaragon.com/doc.php?op=revista3&id=110 Angiography: Cor triatriatum dexter] | | * [http://www.cardioaragon.com/doc.php?op=revista3&id=110 Angiography: Cor triatriatum dexter] |
| * [http://www.emedicine.com/PED/topic2507.htm Cor Triatriatum] at eMedicine, edited by Manuel Caceres
| |
| * [http://www.emedicine.com/med/topic458.htm Cor Triatriatum] at eMedicine, edited by Jamshid Shirani
| |
|
| |
|
| {{Congenital malformations and deformations of circulatory system}}
| |
| {{SIB}}
| |
| [[Category:Congenital heart disease]] | | [[Category:Congenital heart disease]] |
| [[Category:Cardiology]] | | [[Category:Cardiology]] |
| | [[Category:Pediatrics]] |
|
| |
|
| {{WikiDoc Help Menu}} | | {{WikiDoc Help Menu}} |
| {{WikiDoc Sources}} | | {{WikiDoc Sources}} |
{kind=link}
{kind=link}
{kind=link}