Arachnoid cyst
| Arachnoid cyst | ||
 | ||
|---|---|---|
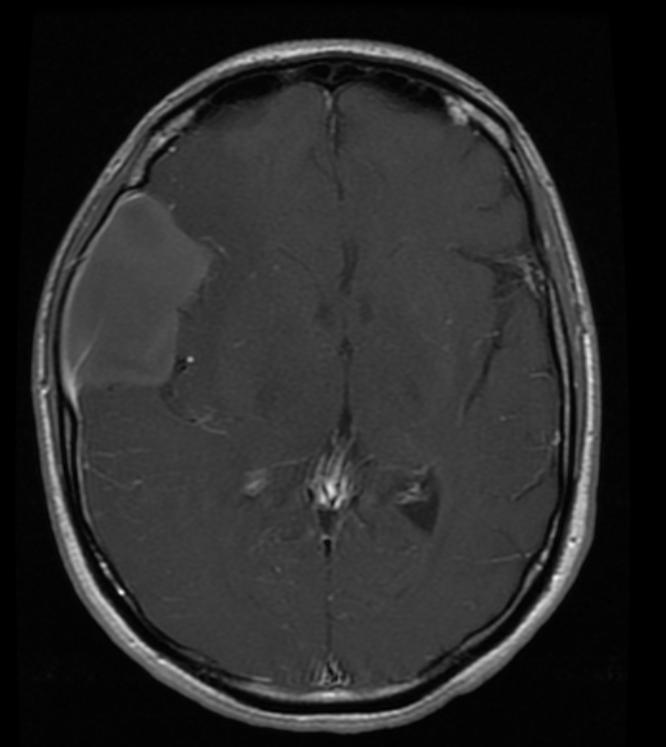
| Suprasellar Arachnoid Cyst; Extension into posterior fossa and displacing the pons (T1 - MRI) Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology | ||
| ICD-10 | Q04.6 | |
| ICD-9 | 348.0 | |
| OMIM | 207790 | |
| DiseasesDB | 33219 | |
| MeSH | D016080 | |
|
Arachnoid cyst Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Arachnoid cyst On the Web |
|
American Roentgen Ray Society Images of Arachnoid cyst |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [3]
Overview
Arachnoid cysts are cerebrospinal fluid covered by arachnoidal cells and collagen[1] that may develop between the surface of the brain and the cranial base or on the arachnoid membrane, one of the three membranes that cover the brain and the spinal cord.[2] Arachnoid cysts are a congenital disorder,[3] and most cases begin during infancy; however, onset may be delayed until adolescence.[2]
Classification
Arachnoid cysts can be intracranial (in the cranium), or on the spine. Intracranial arachnoid cysts usually occur adjacent to the arachnoidal cistern.[4] Spinal arachnoid cysts may be extradural, intradural, or perineural and tend to present with signs and symptoms indicative of a radiculopathy.[4]
Arachnoid cysts can be relatively asymptomatic or present with insidious symptoms; for this reason, diagnosis is often delayed.
Signs and symptoms
Patients with arachnoid cysts may never show symptoms, even in some cases where the cyst is large. Therefore, while the presence of symptoms may provoke further clinical investigation, symptoms independent of further data cannot -- and should not -- be interpreted as evidence of a cyst's existence, size or location.
Symptoms vary by the size and location of the cyst(s), though small cysts usually have no symptoms and are discovered only incidentally.[2] On the other hand, a number of symptoms may result from large cysts:
- Cranial deformation or macrocephaly (enlargement of the head), particularly in children[5]
- Cysts in the suprasellar region in children have presented as bobbing and nodding of the head called Bobble-Head Doll Syndrome.[5]
- Cysts in the left middle cranial fossa have been associated with ADHD in a study on affected children.[6]
- Headaches.[2] While the most common symptom, a patient experiencing a headache does not necessarily have an arachnoid cyst.
- In a 2002 study involving 78 patients with a migraine or tension-type headache, CT scans showed abnormalities in over a third of the patients, though arachnoid cysts only accounted for 2.6% of patients in this study.[7]
- A study found 18% of patients with intracranial arachnoid cysts had non-specific headaches. The cyst was in the temporal location in 75% of these cases.[8]
- Seizures[2]
- Hydrocephalus (excessive accumulation of cerebrospinal fluid)[2]
- Increased intracranial pressure[2]
- Developmental delay[2]
- Behavioral changes[2]
- Hemiparesis (weakness or paralysis on one side of the body)[2]
- Ataxia (lack of muscle control)[2]
- Musical hallucination[9]
- Pre-senile dementia,[10] a condition often associated with Alzheimer's disease
- In elderly patients (>65 years old) symptoms were similar to chronic subdural hematoma or normal pressure hydrocephalus:[11]
- Dementia
- Urinary incontinence
- Hemiparesis
- Headache
- Seizures
Location-specific symptoms
- The following list of location-specific symptoms should be interpreted in the context of what they represent: results from several independent, unrelated studies.
- A supratentorial arachnoid cyst can mimic a Ménière's disease attack.[12]
- Frontal arachnoid cysts have been associated with depression.[13]
- Cysts on the left temporal lobe have been associated with psychosis.[14] [15] A left fronto-temporal cyst more specifically showed symptoms of alexithymia.[16]
- Cyst on the right sylvian fissure resulted in new onset of schizophrenia-like symptoms at age 61.[17]
- A patient with a cyst on the left middle cranial fossa had auditory hallucinations, migraine-like headaches, and periodic paranoia[8]
- Patients with left temporal lobe cysts had mood disturbances similar to manic depression (bipolar disorder)[18]
Causes
The exact cause of arachnoid cysts is not known. Researchers believe that most cases of arachnoid cysts are developmental malformations that arise from the unexplained splitting or tearing of the arachnoid membrane. According to the medical literature, cases of arachnoid cysts have run in families (familial cases) suggesting that a genetic predisposition may play a role in the development of arachnoid cysts in some individuals.
In some cases, arachnoid cysts occurring in the middle fossa are accompanied by underdevelopment (hypoplasia) or compression of the temporal lobe. The exact role that temporal lobe abnormalities play in the development of middle fossa arachnoid cysts is unknown.
In a few rare cases, intracranial arachnoid cysts may be inherited as an autosomal recessive trait. In recessive disorders, the condition does not appear unless a person inherits the same defective gene for the same trait from each parent. If an individual receives one normal gene and one gene for the disease, the person will be a carrier for the disease, but usually will not show symptoms. The risk of transmitting the disease to the children of a couple, both of whom are carriers for a recessive disorder, is 25 percent. Fifty percent of their children risk being carriers of the disease, but generally will not show symptoms of the disorder. Twenty-five percent of their children may receive both normal genes, one from each parent, and will be genetically normal (for that particular trait). The risk is the same for each pregnancy.
In a few rare cases, spinal intradural arachnoid cysts may be inherited as an autosomal dominant trait..
Some complications of arachnoid cysts can occur when a cyst is damaged because of minor head trauma. Trauma can cause the fluid within a cyst to leak into other areas (e.g., subarachnoid space). Blood vessels on the surface of a cyst may tear and bleed into the cyst (intracystic hemorrhage), increasing its size. If a blood vessel bleeds on the outside of a cyst, a collection of blood (hematoma) may result. In the cases of intracystic hemorrhage and hematoma, the individual may have symptoms of increased pressure within the cranium and signs of compression of nearby nerve (neural) tissue.
Arachnoid cysts can also occur secondary to other disorders such as Marfan’s syndrome, arachnoiditis, or agenesis of the corpus callosum. (For more information on these disorders, choose the specific disorder name as your search term in the Rare Disease Database.)[4]
Diagnosis
Diagnosis is principally by MRI. Frequently, arachnoid cysts are incidental findings on MRI scans performed for other clinical reasons. In practice, diagnosis of symptomatic arachnoid cysts requires symptoms to be present, and many with the disorder never develop symptoms.
Additional clinical assessment tools that may be useful in evaluating a patient with arachnoid cysts include the mini-mental state examination (MMSE), a brief questionnaire-based test used to assess cognition.[10] Myelograms are contraindicated for people with arachnoid cysts.
MRI
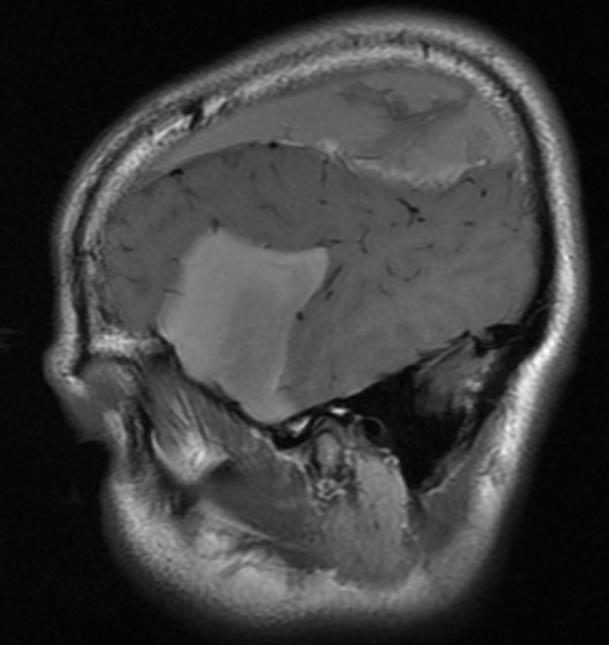
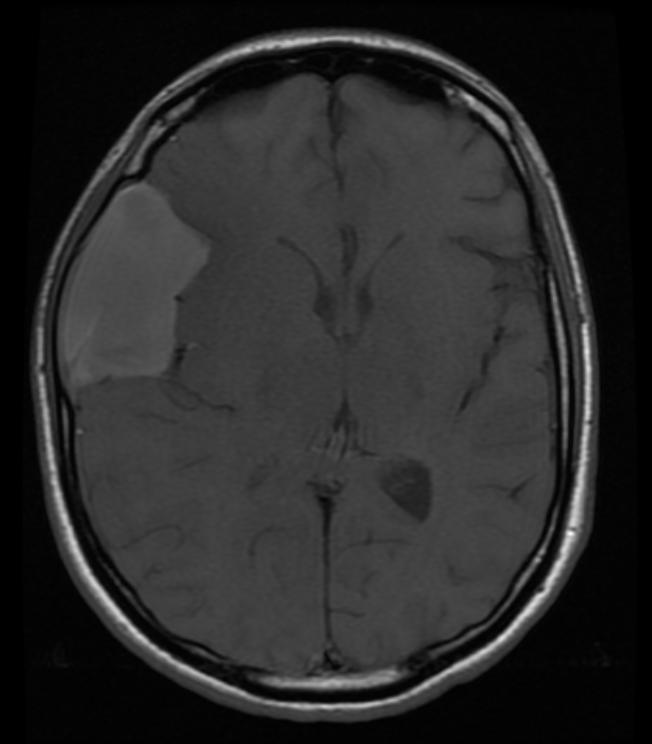
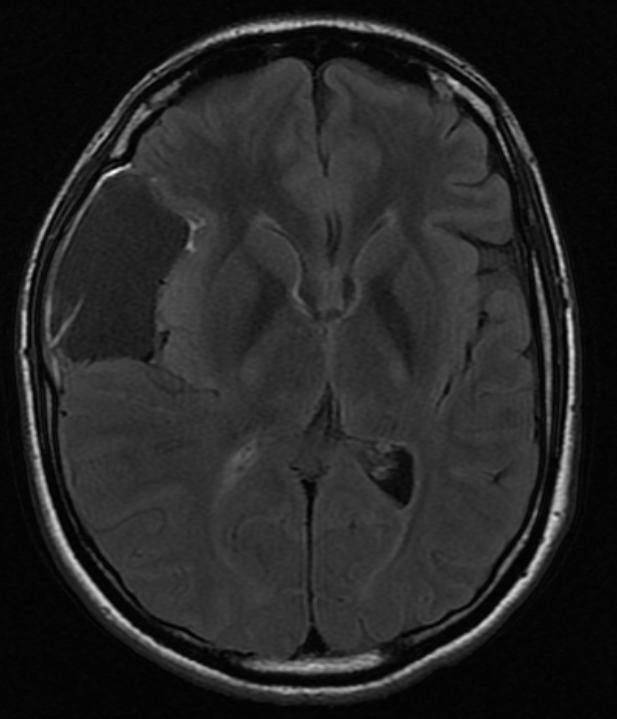
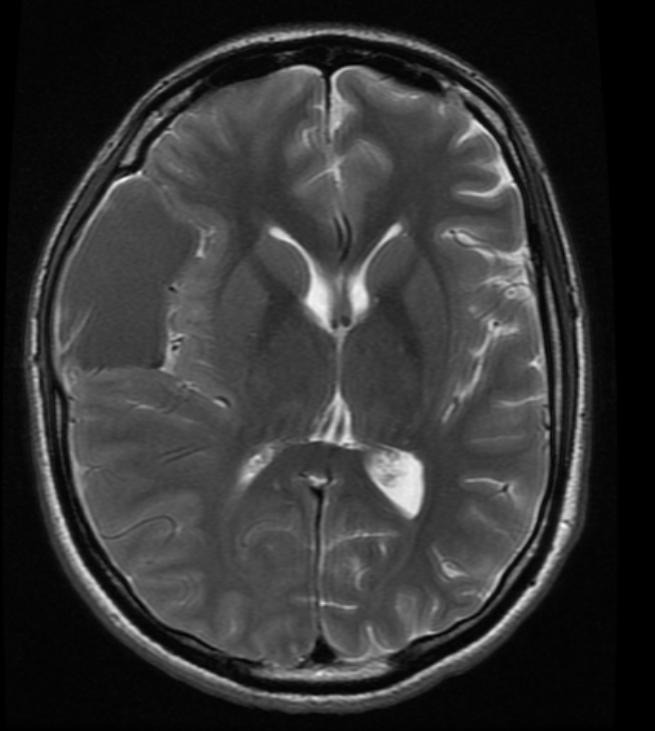
Patient #1: Left middle cranial fossa arachnoid cyst
-
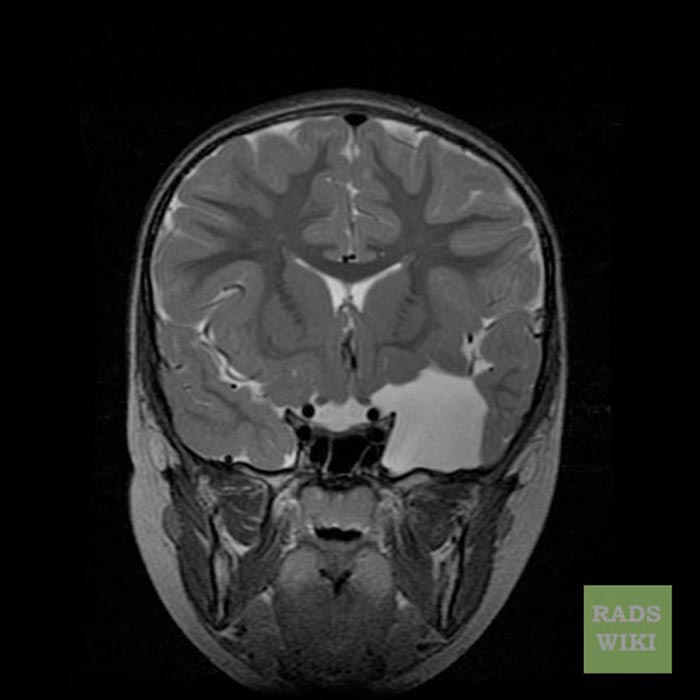
Cor T2
-
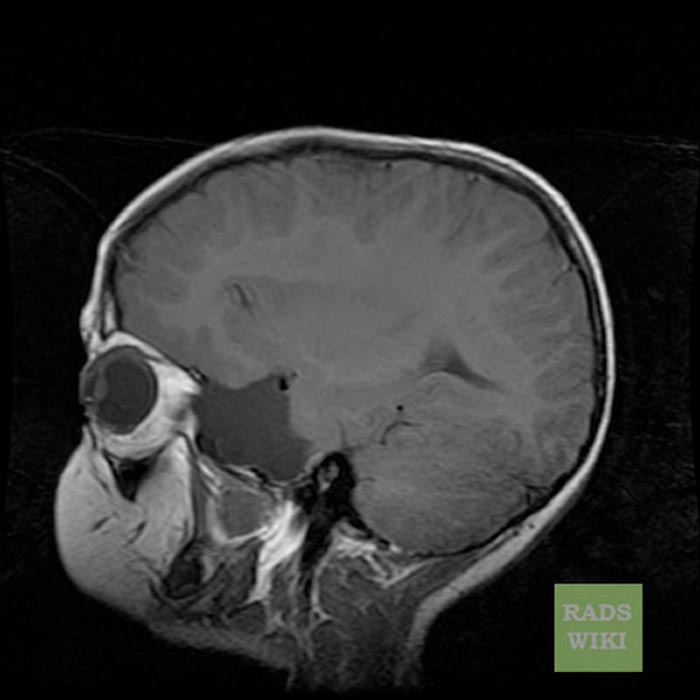
Sag T1
-
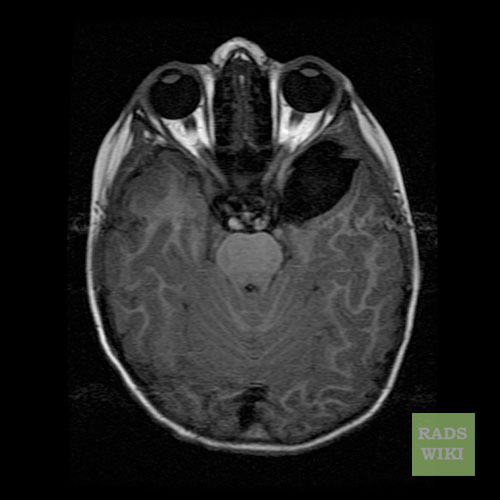
Axial T1 FLAIR
-
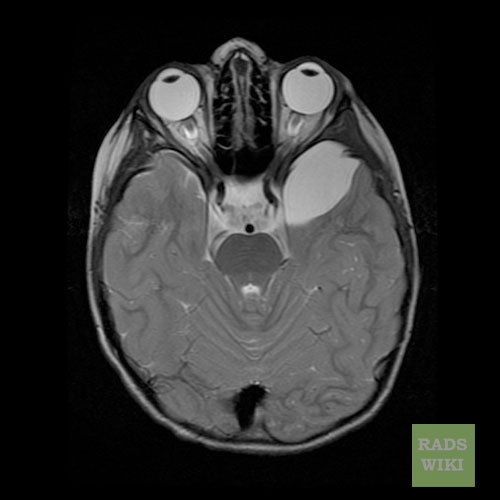
Axial T2




Patient #2: CT and MR images demonstrate a hemorrhagic arachnoid cyst
-

CT
-
Sag T1
-
Ax T1
-
Ax FLAIR
-
Ax T2
-
Ax T1 with GAD






Treatment/Management
Treatment for arachnoid cysts occurs when symptoms present themselves.[2] A variety of procedures may be used to decompress (remove pressure from) the cyst.
- Surgical placement of a cerebral shunt:[19]
- An internal shunt drains into the subdural compartment.[20]
- A cystoperitoneal shunt drains to the peritoneal cavity.
- Fenestration:
- Craniotomy with excision
- Various endoscopic techniques are proving effective,[21] including laser-assisted techniques.[22]
- Drainage by needle aspiration or burr hole. While these procedures are relatively simple, there is a high incidence of recurrence.
- Capsular resection[11]
- Pharmacological treatments may address specific symptoms such as seizures or pain.
A 1994 study found surgery necessary for good outcome in patients >65 years old when the cysts began displaying symptoms.[23]
Sleep aids are often necessary as most people with Arachnoid Cysts do not sleep.
Prognosis
Untreated, arachnoid cysts may cause permanent severe neurological damage due to the progressive expansion of the cyst(s) or hemorrhage (bleeding).[2] With treatment most individuals with arachnoid cysts do well with the double edge sword of developing surgical arachnoiditis which can cause its own specific problems and can lead to "popping" another cyst.
More specific prognoses are listed below:
- Patients with arachnoid cysts of the left temporal fossa who experienced impaired preoperative cognition had postoperative improvement.[24]
- Surgery can resolve psychiatric manifestations in selected cases.[25]
Epidemiology
Arachnoid cysts are seen in 4% of the population.[26] Only 20% of these have symptoms, usually from secondary hydrocephalus.[26]
A study that looked at 2,536 healthy young males found a prevalence of 1.7% (95% CI 1.2 to 2.3%). Only a small percentage of the detected abnormalities require urgent medical attention.[27]
See also
- Acoustic Neuroma
- Arachnoiditis
- Brain Tumors, General
- Dandy-Walker Syndrome
- Empty Sella Syndrome
- Epidermoids
- Midline Caves of the Brain
- Porencephaly
- Syringomyelia
- Bobble-Head Doll Syndrome
- Hyperprolactinemia
- Panhypopituitarism
- Arnold-Chiari Malformation
Patient Information
What are Arachnoid Cysts?
Arachnoid cysts are cerebrospinal fluid-filled sacs that are located between the brain or spinal cord and the arachnoid membrane, one of the three membranes that cover the brain and spinal cord. Primary arachnoid cysts are present at birth and are the result of developmental abnormalities in the brain and spinal cord that arise during the early weeks of gestation. Secondary arachnoid cysts are not as common as primary cysts and develop as a result of head injury, meningitis, or tumors, or as a complication of brain surgery. The majority of arachnoid cysts form outside the temporal lobe of the brain in an area of the skull known as the middle crania fossa. Arachnoid cysts involving the spinal cord are rarer. The location and size of the cyst determine the symptoms and when those symptoms begin. Most individuals with arachnoid cysts develop symptoms before the age of 20, and especially during the first year of life, but some people with arachnoid cysts never have symptoms. Males are four times more likely to have arachnoid cysts than females.
Typical symptoms of an arachnoid cyst around the brain include headache, nausea and vomiting, seizures, hearing and visual disturbances, vertigo, and difficulties with balance and walking. Arachnoid cysts around the spinal cord compress the spinal cord or nerve roots and cause symptoms such as progressive back and leg pain and tingling or numbness in the legs or arms. Diagnosis usually involves a brain scan using diffusion-weighted MRI (magnetic resonance imaging) which helps distinguish fluid-filled arachnoid cysts from other types of cysts.
Is there any treatment?
There has been active debate about how to treat arachnoid cysts. The need for treatment depends mostly upon the location and size of the cyst. If the cyst is small, not disturbing surrounding tissue, and not causing symptoms, some doctors will refrain from treatment. In the past, doctors placed shunts in the cyst to drain its fluid. Now with microneurosurgical techniques and endoscopic tools that allow for minimally invasive surgery, more doctors are opting to surgically remove the membranes of the cyst or open the cyst so its fluid can drain into the cerebrospinal fluid and be absorbed.
What is the prognosis?
Untreated, arachnoid cysts may cause permanent severe neurological damage when progressive expansion of the cyst(s) or hemorrhage injures the brain or spinal cord. Symptoms usually resolve or improve with treatment.
What research is being done?
The National Institute of Neurological Disorders and Stroke (NINDS) conducts research related to brain abnormalities and disorders of the nervous system such as arachnoid cysts in laboratories at the National Institutes of Health (NIH), and supports additional research through grants to major medical institutions across the country. Much of this research focuses on finding better ways to prevent, treat, and ultimately cure neurological disorders such as arachnoid cysts.
References
- ↑ Ariai S, Koerbel A, Bornemann A, Morgala M, Tatagiba M. "Cerebellopontine angle arachnoid cyst harbouring ectopic neuroglia", Pediatr Neurosurg. 2005 Jul-Aug;41(4):220-3. (PMID 16088260)
- ↑ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 2.10 2.11 2.12 http://www.ninds.nih.gov/disorders/arachnoid_cysts/arachnoid_cysts.htm NINDS Arachnoid Cysts Information Page
- ↑ Gelabert-Gonzalez M. "Intracranial arachnoid cysts", Rev Neurol., 2004 Dec 16-31;39(12):1161-6. (PMID 15625636)
- ↑ 4.0 4.1 Arachnoid cyst. (n.d.). Gale Encyclopedia of Neurological Disorders. Retrieved September 10, 2006, from Answers.com Web site: http://www.answers.com/topic/arachnoid-cyst
- ↑ 5.0 5.1 Barker RA, Scolding N, Rowe D, Larner AJ. The A-Z of Neurological Practice: A Guide to Clinical Neurology Cambridge University Press 2005 Jan 10, p61. (ISBN 0-521-62960-8)
- ↑ Millichap JG. "Temporal lobe arachnoid cyst-attention deficit disorder syndrome: role of the electroencephalogram in diagnosis", Neurology 1997 May;48(5):1435-9. (PMID 9153486)
- ↑ Valença MM, Valença LP, Menezes TL. "Computed tomography scan of the head in patients with migraine or tension-type headache", Arq Neuropsiquiatr. 2002 Sep;60(3-A):542-7. (PMID 12244387)
- ↑ 8.0 8.1 Cameron AD. "Psychotic phenomena with migraine and an arachnoid cyst", Progress in Neurology and Psychiatry 2002 Mar-Apr 6(2) http://www.escriber.com/Progress/Features.asp? Action=View&Archive=True&ID=67&GroupID=&Page=11
- ↑ Griffiths TD. "Musical hallucinosis in acquired deafness. Phenomenology and brain substrate.", Brain, 2000 Oct;123 ( Pt 10):2065-76. (PMID 11004124)
- ↑ 10.0 10.1 Richards G, Lusznat RM. "An arachnoid cyst in a patient with pre-senile dementia", Progress in Neurology and Psychiatry, 2001 May-June;5(3) http://www.escriber.com/Progress/Features.asp? Action=View&Archive=True&ID=29&GroupID=&Page=18
- ↑ 11.0 11.1 Yamakawa H, Ohkuma A, Hattori T, Niikawa S, Kobayashi H. "Primary intracranial arachnoid cyst in the elderly: a survey on 39 cases", Acta Neurochir (Wien). 1991;113(1-2):42-7. (PMID 1799142)
- ↑ Buongiorno G, Ricca G. "Supratentorial arachnoid cyst mimicking a Ménière's disease attack", J Laryngol Otol. 2003 Sep;117(9):728-30. (PMID 14561365)
- ↑ Cummings JL, Mega MS. Neuropsychiatry and Behavioral Neuroscience, Oxford University Press, USA; 2Rev Ed, 2003 Jan 23;208. (ISBN 0-19-513858-9)
- ↑ Alves da Silva J, Alves A, Talina M, Carreiro S, Guimarães J, Xavier M. "Arachnoid cyst in a patient with psychosis: a case report" Annals of General Psychiatry 2007, 6:16) [1]
- ↑ Vakis AF, Koutentakis DI, Karabetsos DA, Kalostos GN. "Psychosis-like syndrome associated with intermittent intracranial hypertension caused by a large arachnoid cyst of the left temporal lobe", Br J Neurosurg. 2006 Jun;20(3):156-9. (PMID 16801049)
- ↑ Blackshaw S, Bowen RC. "A case of atypical psychosis associated with alexithymia and a left fronto-temporal lesion: possible correlations", Can J Psychiatry 1987 Nov;32(8):688-92. (PMID 3690485)
- ↑ Cullum CM, Heaton RK, Harris MJ, Jeste DV. "Neurobehavioral and neurodiagnostic aspects of late-onset psychosis", Arch Clin Neuropsychol. 1994 Oct;9(5):371-82. (PMID 14589653)
- ↑ Heinrichs, RW. In Search of Madness: Schizophrenia and Neuroscience Oxford University Press, USA (March 29, 2001); p129. (ISBN 0-19-512219-4)
- ↑ Strojnik T. "Different approaches to surgical treatment of arachnoid cysts", Wiener Klinische Wochenschrift.[2] 2006;118 Suppl 2:85-8. (PMID 16817052)
- ↑ Helland CA, Wester K. "Arachnoid cysts in adults: long-term follow-up of patients treated with internal shunts to the subdural compartment", Surg Neurol. 2006 Jul;66(1):56-61; discussion 61. (PMID 16793443)
- ↑ Greenfield JP, Souweidane MM. "Endoscopic management of intracranial cysts", Neurosurg Focus. 2005 Dec 15;19(6):E7. (PMID 16398484)
- ↑ Van Beijnum J, Hanlo PW, Han KS, Ludo Van der Pol W, Verdaasdonk RM, Van Nieuwenhuizen O. "Navigated laser-assisted endoscopic fenestration of a suprasellar arachnoid cyst in a 2-year-old child with bobble-head doll syndrome", J Neurosurg. 2006 May;104(5 Suppl):348-51. (PMID 16848093)
- ↑ Caruso R, Salvati M, Cervoni L. "Primary intracranial arachnoid cyst in the elderly", Neurosurg Rev. 1994;17(3):195-8. (PMID 7838397)
- ↑ Wester K, Hugdahl K. "Arachnoid cysts of the left temporal fossa: impaired preoperative cognition and postoperative improvement." J Neurol Neurosurg Psychiatry 1995 Sep;59(3):293-8. (PMID 7673959)
- ↑ Kohn R, Lilly RB, Sokol MS, Malloy PF. "Psychiatric presentations of intracranial cysts", J Neuropsychiatry Clin Neurosci 1989; 1:60-66. (PMID 2577719)
- ↑ 26.0 26.1 Flaherty AW. The Massachusetts General Hospital Handbook of Neurology 2000 Jan 1;105. (ISBN 0-683-30576-X)
- ↑ Weber F, Knopf H. "Incidental findings in magnetic resonance imaging of the brains of healthy young men", J Neurol Sci. 2006 Jan 15;240(1-2):81-4. Epub 2005 Oct 26. (PMID 16256141)
External links
Patient support sites: