Renal ectopia
| Renal ectopia | |
| ICD-10 | Q63.2 |
|---|---|
| ICD-9 | 753.3 |
|
WikiDoc Resources for Renal ectopia |
|
Articles |
|---|
|
Most recent articles on Renal ectopia Most cited articles on Renal ectopia |
|
Media |
|
Powerpoint slides on Renal ectopia |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Renal ectopia at Clinical Trials.gov Trial results on Renal ectopia Clinical Trials on Renal ectopia at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Renal ectopia NICE Guidance on Renal ectopia
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Renal ectopia Discussion groups on Renal ectopia Patient Handouts on Renal ectopia Directions to Hospitals Treating Renal ectopia Risk calculators and risk factors for Renal ectopia
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Renal ectopia |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Contributors: Cafer Zorkun M.D., PhD.
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [2] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Overview
Renal ectopia or ectopic kidney describes a kidney that is not located in its usual position. It results from the kidney failing to ascend from its origin in the true pelvis or from a superiorly ascended kidney located in the thorax.
Crossed-fused renal ectopia
- Crossed ectopy = kidney located on the opposite side of the midline from its ureter. [1] [2] [3] [4]
- In 90% of crossed ectopy, there is at least partial fusion of the kidneys (the remainder demonstrate two discrete kidneys on the same side, crossed-unfused ectopy)
- Due to improper renal ascent in embryogenesis (4th-8th week of fetal life - normally, the kidney reaches its appropriate position at L2 level at the end of the 2nd month)
- Fusion of the kidneys within the pelvis leads to crossed-fused renal ectopia.
- Abnormally situated umbilical artery prevents normal cephalic migration. Another theory is that the ureteric bud crosses to the opposite side and induces nephron formation in the contralateral metanephric blastema.
Epidemiology
- Incidence: 1 out of 1,000 births.
- 2:1 male to female ratio
- A single renal mass with two collecting systems is located on one side of the abdomen.
- Left-to-right ectopy three times more common.
Pathogenesis
- Normal ascent of the kidneys is required for formation of the extraperitoneal perirenal fascial planes.
- Ectopia (or renal agenesis) results in failure of development of fascial layers in the flanks on the side not occupied by renal tissue.
- Lack of restraining fascia leads to possible malposition of bowel into the extraperitoneal fat of the empty renal fossa and relaxation of mesenteric supports for bowel loops in this region.
Diagnostic Findings
- Readily detected on conventional urography.
- CT and US very useful.
- On US, identified by characteristic anterior or posterior "notch" between the two fused kidneys.
- Anterograde or retrograde ureterogram most often demonstrates normal bladder trigone without ureteral ectopy.
- Blood supply usually anomalous.
- Angiography recommended before surgical intervention.
- Findings on CT or barium contrast studies of the bowel should be interpreted in light of bowel laxity in the region of the empty renal fossa (discussed above). In particular, distinction must be made from internal hernia.
Patient #1: CT images demonstrate cross-fused renal ectopia
-
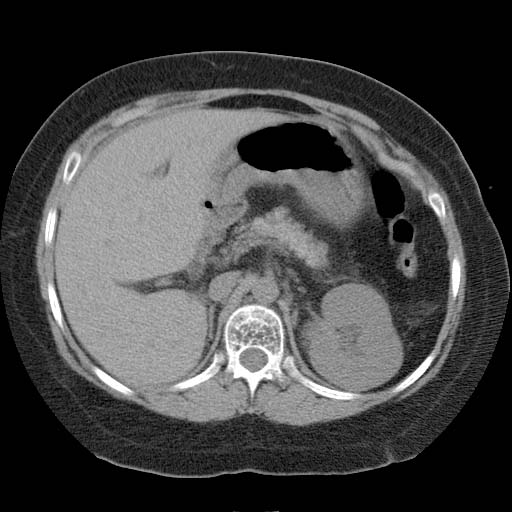 Kidney 1
Kidney 1 -

-
 Kidney 2
Kidney 2



Patient #2: Renal scan images demonstrate cross-fused renal ectopia



Complications
- In a crossed fused renal ectopic kidney, complications such as nephrolithiasis, infection, and hydronephrosis approaches 50%.
References
- ↑ Dunnick, N.R., Sandler, C.M., Newhouse, J.H., and Amis, E.S. Textbook of uroradiology, 3rd Edition. Lippincott Williams and Wilkins, 2001.
- ↑ Dyer, R.B., Chen, M.Y., and Zagoria, R.J. Classic signs in uroradiology. Radiographics, 2004; 24:S247-S280.
- ↑ Gay, S.B., Armistead, J.P. Weber, M.E., and Williamson, B.R.J. Left infrarenal region: anatomic variants, pathologic conditions, and diagnostic pitfalls. Radiographics 1991; 11: 549-570.
- ↑ Meyers, M.A., Whalen, J.P., Evans, J.A. and Viamonte, M. Malposition and displacement of the bowel in renal agenesis and ectopia: new observations. AJR, 1972; 117,2: 323-333.