Follicular lymphoma pathophysiology
|
Follicular lymphoma Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Follicular lymphoma pathophysiology On the Web |
|
American Roentgen Ray Society Images of Follicular lymphoma pathophysiology |
|
Risk calculators and risk factors for Follicular lymphoma pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Sowminya Arikapudi, M.B,B.S. [2]
Overview
Genes involved in the pathogenesis of follicular lymphoma include BCL-2 and BCL-6. The progression to follicular lymphoma involves microRNAs (miRNAs). On microscopic histopathological analysis, centrocytes and centroblasts are characteristic findings of follicular lymphoma.
Pathophysiology
Physiology
- Follicular helper T cells (Tfh) are specialized helper T cells that are predominantly located in germinal centers and provide help to B cells.
- Follicular lymphoma is the second most common non-Hodgkin lymphoma.
- The disease is characterized by the clonal proliferation of neoplastic lymphoid cells that share morphological, immunophenotypic and molecular genetic attributes of germinal centre B cells.
- The development of FL tumors in adults is dependent upon the overexpression of B cell leukemia/lymphoma 2 (BCL-2) located on chromosome band 18q21.
- BCL-2 is an oncogene that blocks programmed cell death (apoptosis). As such, overexpression results in prolonged cell survival.
- These tumours contain a mixture of neoplastic centrocytes and centroblasts along with various non-neoplastic cells including T cells, follicular dendritic cells, and macrophages.
- FL can be designated as low grade (1 and 2) or higher grade (3A and 3B) disease, depending on the number of centroblasts per high-power field [6].
Pathogenisis
- In follicular lymphoma, a single follicular B cell acquires all of the genetic and epigenetic alterations needed for malignant transformation.
- The most common cause is reciprocal translocation t(14;18)(q32;q21). in 80-85% of cases.
- This somatic rearrangement, which constitutes the first step of lymphomagenesis, is initiated within the bone marrow during B-cell lymphopoiesis and results from immunoglobulin heavy chain gene (IGH) rearrangement.
- The t(14;18) translocation leads to placement of the B cell lymphoma 2 (BCL2) gene under the inductive influence of transcriptional enhancers associated with IGH, resulting in overexpression of anti-apoptotic BCL2 leading to increased cell survival and uncontrolled cell proliferation in germinal centres.
- BCL2, along with other anti-apoptotic proteins, inhibits apoptosis by binding and neutralizing activated pro-apoptotic proteins including the mitochondrial outer membrane permeabilizers BAX and BAK, as well as the intracellular stress sensors BIM and PUMA which activate BAX and BAK.
- Mutations in chromatin-modifying genes occur, affecting histone methyltransferases, histone acetyltransferases or histone linker proteins.
- These mutations act to promote lymphomagenesis
- Genes encoding components of vacuolar H+-ATPase, or RRAGC, a guanine nucleotide binding protein, regulate mTOR activation.
- Mutations in these genes upregulate mTOR (mammalian target of rapamycin) signaling in FL cells. These mutations are found in approximately 15 to 20 percent of cases.
- Upregulated mTOR directs many cellular processes including growth, differentiation, survival, and adhesion or cellular migration, and resulting in follicular lymphoma development.
- KMT2D, CREBBP, EZH2, EP300, HIST1H1E, KMT2C, ARID1A, and SMARCA4 are some of the other genomes which undergo mutations in a very few cases.
- The tumor microenvironmen comprised of T cells and dendritic cells, may influence the development and progression of Follicular lymphoma.
- Communication between the tumor cells and the microenvironment involves chemokines, chemokine receptors and adhesion molecules, the balance of which determines whether there is tumor cell growth promotion or inhibition.
- MicroRNA expression- short non-coding RNAs named microRNAs (miRNAs) have important functions in follicular lymphoma biology.
- In malignant B cells miRNAs participate in pathways fundamental to B cell development like
- B cell receptor (BCR) signalling
- B cell migration/adhesion, cell-cell interactions in immune niches
- The production and class-switching of immunoglobulins.[1]
- MiRNAs influence B cell maturation, generation of pre marginal zone, follicular, B1, plasma and memory B cells[1]
Genetics
- A translocation between chromosome 14 and 18 results in the overexpression of the BCL-2 gene.[2]
- The BCL-2 gene is normally found on chromosome 18, and the translocation moves the gene near to the site of the immunoglobulin heavy chain enhancer element on chromosome 14.
- Translocations of BCL6 at 3q27 can also be involved.[3]
- It is positive for the B-cell markers CD10, CD19, CD22, and usually CD20,[4] but almost always negative for CD5.[5]
Gross Pathology
-

Classic appearance of spleen involved by follicular lymphoma, namely the presence of discrete, miliary, small, white "pearly" nodules throughout the whole parenchyma.
-

Follicular lymphoma replacing a lymph node.


Microscopic Pathology
The tumor is composed of follicles containing a mixture of the following:
- Centrocytes (small cleaved cells without nucleoli)
- Centroblasts (larger noncleaved cells with moderate cytoplasm, open chromatin and multiple nucleoli)
- These follicles are surrounded by non-malignant cells, mostly T-cells.
Within the follicles, centrocytes typically predominate; centroblasts are usually scarce.
-
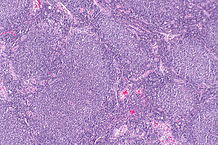
Micrograph of a follicular lymphoma, showing the characteristically abnormal lymphoid follicles. H&E stain

Grading
According to the WHO criteria, the disease is morphologically graded into:[6]
- grade 1 (<5 centroblasts per high-power field (hpf))
- grade 2 (6–15 centroblasts/hpf)
- grade 3 (>15 centroblasts/hpf)
- grade 3A (centrocytes still present)
- grade 3B (the follicles consist almost entirely of centroblasts)
The WHO 2008 update provided the following grading for follicular lymphoma:
- Grades 1 and 2 now as low grade follicular lymphoma
- Grade 3A as high grade follicular lymphoma
- Grade 3B as diffuse large B Cell lymphoma
References
- ↑ 1.0 1.1 Musilova, K; Mraz, M (2014). "MicroRNAs in B cell lymphomas: How a complex biology gets more complex". Leukemia. doi:10.1038/leu.2014.351. PMID 25541152.
- ↑ Bosga-Bouwer AG, van Imhoff GW, Boonstra R; et al. (February 2003). "Follicular lymphoma grade 3B includes 3 cytogenetically defined subgroups with primary t(14;18), 3q27, or other translocations: t(14;18) and 3q27 are mutually exclusive". Blood. 101 (3): 1149–54. doi:10.1182/blood.V101.3.1149. PMID 12529293.
- ↑ Bosga-Bouwer AG, Haralambieva E, Booman M; et al. (November 2005). "BCL6 alternative translocation breakpoint cluster region associated with follicular lymphoma grade 3B". Genes Chromosomes Cancer. 44 (3): 301–4. doi:10.1002/gcc.20246. PMID 16075463.
- ↑ Overview at UMDNJ
- ↑ Barekman CL, Aguilera NS, Abbondanzo SL (July 2001). "Low-grade B-cell lymphoma with coexpression of both CD5 and CD10. A report of 3 cases". Arch. Pathol. Lab. Med. 125 (7): 951–3. doi:10.1043/0003-9985(2001)125<0951:LGBCLW>2.0.CO;2. PMID 11419985.
- ↑ "Follicular Lymphomas". Retrieved 2008-07-26.